The Histomorphology of Tiny Lobes from the Bilobed Placenta
Two bilobed placentas were obtained of woman pregnancy at 37 and 38 weeks of gestation with newborns live and examined the villous tree with light microscope. Two small lobes were found in one placenta and other in the second placenta. Two normal placentas were taken as control. Ten histological samples by each lobe were processed with H&E stain. Five biopsies by each normal placenta were taken and three histological slides by biopsy were dyed equally. Degenerative changes at level of vessels of the placental villi were noted in stem villi: stromal lysis, multiple capillarity, congestioned vessels, and increased dilatation of vessels. Regions of immature villi, pre- infarcts, deficiency of terminal villi in mature intermediate villi, destroyed villi, in immature villi the vessels are near to the syncytium indicating extensive hypoxic villous damage. In this condition a diminution of the blood flow or events of thrombosis could to be affecting the growth of these small lobules.
Introduction
The bilobed placenta is one of unusual placenta forms between anular placenta and placenta fenestrata as so mentioned [1]. It is shaped by two lobes, of irregular form, separated by segments of membrane belonging at the chorionic plate which presents blood vessels of the umbilical cord that suffers thrombosis provoking hemorhages with fetal problems serious during the delivery [2]. There is a scanty report of the very little or tiny lobes which are associated with one of these larger lobes in the bilobed placenta [3]. These lobes can to represent to very small or tiny placentas, whose umbilical cord would be confirmed by chorionic membrane with vessels. Correspond to succenturiate lobes, accessories or aberrants of very small size [4]. The features histomorphological of these small lobes have been little studied. Our interest is in to describe if there is degenerative changes in the placental villi that could to affect the normal interchange of gases or nutrients.
The origen of the bilobed placenta is unknown. A disk is inserted in the anterior wall of the uterus and the other in the posterior wall, one of them is connected by velamentous insertion of the umbilical cord and both by the chorionic plate that contains vessels [2]. The bipartite placenta has been considered to form if there is inadequate nourishement of the decidua causing the placenta to recede and proliferate in other areas, resulting in superficial implantation or trophotropism as reported by Benirschke and Driscoll [5].
Torpin R, et al. [6] hypothesized that the morula may implant on both walls of the uterus similar to nidation of the rhesus monkey. Bilobed placenta can to be associated with first trimester bleeding, polyhydramnios, abruption and retained placenta [7]. Anomalies of placental growth with respect to its shape has been associated with adverse pregnancy outcomes in a very rare form of “H “ bilobate placental partition, in a 31 year old woman at 24 weeks of gestation [8].
There is not much literature on the pathophysiology and etiology of the bilobed placenta. Some authors use the words bilobed placenta and succenturiate placenta interchangeably. There does not appear to be any increased risk of anomaly to the fetus in this type of placentation. However a velamentous cord insertion, depending on the location, is associated with abnormal fetal growth [9]. The bipartite placenta is typical of multigravidas with five or more pregnancies and older woman, 35 years or more, history of infertility, previa placenta, adherent placenta, no increase of death rate of the offspring and birth weight, gestational age, in normal range [10].
Is a placental morphological variation, separated in two near equal lobes, not associated with an increased risk of foetal anomalie, being a risk factor the cigarette smoking. The causes that produce it are: Implantation in areas of decreased blood supply, implantation on uterine fibroid area of previous surgery or over cervical opening. The number of previous cesarean deliveries not has significative effect on their formation [11]. Is our proposal to describe the histomorphology of these tiny lobes with light microscopy reporting their placental villous tree.
Material and Methods
Two bilobed placentas were obtained of woman pregnancy in 37 and 38 weeks at term, with newborns live, for the study of these lobes with light microscope. A descriptive and retrospective study without probabilistic sampling was used. Two small lobes were found in one placenta with the following sizes: 4cm.x2.5cm.x1.5cm and 3.5cm.x2.5cm. x0.7cm and in the second placenta another with 3cm.x2.5cm. x1.3cm [3]. Ten histological samples by each lobe were processed with H&E stain. Two normal placentas were taken and 5 biopsies obtained by each placenta. Three histologycal slides by each biopsy were processed. For examine the microscopic lesions 20 camps by histological slide with the 40x objective were observed. The nomenclature of the placental villi is the used by Benirschke and Kaufmann [2].
Results
Stem villi showed changes at level of vessels with the muscular layer edematized and damaged endothelium. The stromal region is interrupted in the fibrous zone exhibiting clear spaces. These villi present ramifications with multiple capillarity (Figures 1a & 1b). The vessels were found dilated. Proliferation of congestioned vessels can to be seen in their stromal region and in mature intermediate villi. It was ocassionaly observed stem villi showing the impulsion of a wave of sanguine expansion in their vessel while that other vessel was thrombosed (Figure 2a & 2b). Some of these vessels of the placental villi could to explode and fragments of them are scattered in the intervillous space.
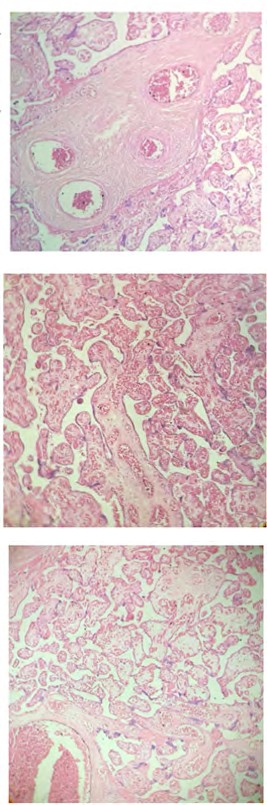
Figure 1a: Stem villi shows in their vessels dilatation and muscular layer edematized. H& E.400x.
Figure 1b: Ramifications of stem villi present multiple vascularity. H&E.400x.
Figure 2a: Stromal region of immature intermediate villi is occupied, in part, by vessels in the peripheral region. H&E.400x.
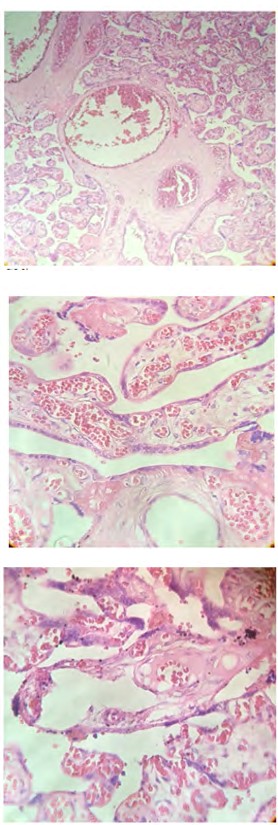
Figure 2b: An erithrocytic line (arrow) indicating a new expansion of the vessel in stem villi.H&E.400x.
Figure 3a: Mature intermediate villi with deficiency of terminal villi.H&E.400x.
Figure 3b: Villi with stromal region very damaged. H&E. 400x.
With frequency zones of immaturity are noted and conglomerate of villi when found are united by syncytial contact and them could to form Tenney-Parker sign in isquemic areas of margins of infarcts. Placental villi is seen with great loss of stromal region (Figures 3a & 3b).
The mature intermediate villi when seen had deficiency of terminal villi. During the observations a great deal of placental villi were observed destroyed and in immature zones the vessels of the stromal region are located near the syncytium.
Discussion
The changes observed in stem villi at level of vessels and stromal region are consequence of thrombosis suffered by these villi. Degenerative changes in the wall of vessels were noted with scanning electron microscopy in a preliminary study that describes a thrombosed vessel [3]. The presence of multiple capillarity is indicative of isquemic or extensive hypoxic villous damage; many vessels are near to the syncytium, treating of to absorb gases or nutrients [2].
Congestioned vessels appear in placental villi that often show evidence of continued branching angiogenesis as is the case with anemic pregnancy which reflect continued hypoxia driven activity of vascular endothelial growth factor (VEGF) [12]. The sudden arrival of a wave of sanguine expansion has provoked dilatation in the vessels as seen in Figure 2b. In this condition of hypoxia there is intermission of blood flow while the compression, during uterine contractions, is maintained in little time [13]. The expression in regions of pre-infarcts and conglomerate of villi with numerous syncytial knots shows that these, in part, were developing at the 37-38 weeks; time that corresponds to a higher number of syncytial knots [14].
The dilatation in stromal vessels can to lead to the crackling or explosion and provoke the lisis of stromal region or great loss of it. If the time of uterine contraction is very length the uterine compression originates terminal villi elongated or straight, named filiform villi, which is shaped during the detention of the blood flow in their capillars [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. The results here written reconfirm the observed in intrauterine growth restriction, rhesus incompatibility [2] and obese placenta [15].
Patients complicated by succenturiate lobes of placenta support the adverse obstetric outcomes in pregnancies as incidence of vasa previa, postpartum hemorrhage and retained placenta when the frequency of maternal age>=35 years and a history of using in vitro fertilization [16]. An irregular maternal utero-placental environment affects macroscopic placental structure causing a change in its shape [17]. The irregular placental shape in these cases is associated with deformation of the placental vascular network and diminished placental efficiency with negative perinatal outcomes [18].
The organization of placentation sites is affected by an assortment of environmental exposures, disease states, infections agents, stressors, etc. Hypoxia-inducible factor has been identified as a regulatory mechanism mediating placental adaptations to low oxygen tensions [19]. In these small lobes there is variation in the supply of nutrients to the fetus by the presence of immaturity in the placental villi. The mature intermediate villi lack of terminal villi and the nutrient flow is decreased being these regions of the placenta variable in its morphology and functional capacity with respect to larger lobes [20].
Succenturiate lobes have a tendency to infarct, to be remarkably hemorrhagic, occasionally atrophic, but the mechanism by which succenturiate lobes and duplex placentas develop is unclear. The segment of membrane that connects these small lobes with larger lobes contains membranous vessels that can thrombose and to provoke bleeding [2]. These lobes may present as placenta previa and to be retained in utero after delivery [21]. With this placental anomaly there is an increased incidence of postpartum infection and hemorrhage.
Approximately 50% of vasa previa is associated with succenturiate placenta [22]. It is conceivable that a posterior placenta with an anterior succenturiate lobe is more easily diagnosed that an anterior placenta with a posterior succenturiate lobe: The succenturiate lobe would have a greater chance to be hidden by the fetal body and remain undetected. The recognition by obstetricians and sonologists is important because of the high postpartum risk associated with retention of placental material and the possibility of catastrophic rupture of the connecting vessels during delivery [23].
So, in this morphological abnormality, fetal death may ensue [24]. These lobes have been considered as vestiges of abnormal distributions of the chorionic villi [25] and have been seen in an extrauterine ambient of abdominal pregnancy, in a case study, indicating capacity of adaptation [26]. A succenturiate lobe may be implanted low in the vicinity of the internal os (Placenta previa) with the likelihood of premature separation and attendant hemorrhage during delivery [27]. This condition increases the risks for prematurity, impaired fetal growth and cesarean delivery [28].
Conclusion
Villous maldevelopment provoked by persisting villous immaturity in these tiny lobes composed of stem and mature intermediate villi with largely lacking terminal villi indicates delayed maturation. They are in extensive hypoxic villous damage provoked by a diminution of the blood flow or thrombosis of stem villi which has inhibited their development.
References
-
Kleine HO (1956) Unusual placenta forms; anular placenta, bilobed placenta, and placenta fenestrata. Zentralbl Gynakol 78(51): 2029-2032.
-
Benirschke K, Kaufmann P (2000) Pathology of the human placenta. 4th (Edn.), Springer-Verlag, New York.
-
Castejon OC, Lopez AJ, Castejon OJ, Quiroz D (2009) Estudio microscopico de la vellosidad corionica en la placenta bilobulada. Salus 13(1): 34-38.
-
Fachin De Boni J (1962) Sobre un caso de placenta succenturiada con masa aberrante previa. Rev Obstet Ginecol Venez 21: 301-306.
-
Benirschke K, Driscoll SG (1967) the pathology of the human placenta. Springer Verlag, New York, pp: 10.
-
Torpin R, Hart BF (1941) Placenta Bilobata. Am J Obstet Gynecol 42(1): 38-49.
-
Rathbun KM, Hildebrand JP (2019) Placenta abnormalities. StatPearls (Internet) Treasure Island (FL).
-
Okolito UV, Moyosore AA, Kofo QK, James AO (2015) H´shaped bilobate placental partition: A rare placenta variation. J Clin Diagn Res 9(8): 5-6.
-
Brucks UA, Duval JR (2002) Perinatal evaluation of the bilobed placenta or bipartite placenta. J Diagn Med Sonog 18(3): 161-166.
-
Fujikura T, Benson RC, Driscoll SG (1970) The bipartite placenta and clinical features. AJOG 107(7): 1013-1017.
-
Rani BP, Kumar PG, Chowdhury M, Md Selim (2016) A rare shape of placenta: Placenta Bipartite, Bilobata, Dimidiate, Duplex: A rare case report. Bangladesh Journal of Obstetrics & Gynaecology 31(2): 101-103.
-
Kigndom JC, Kaufmann P (1999) Oxygen and placental vascular development. Adv Exp Med Biol 474: 259-275.
-
Kingdom J, Huppertz B, Seaward G, Kaufmann P (2000) Development of the placental villous tree and its consequences for fetal growth. Eur J Obstet Gynecol Reprod Biol 92(1): 35-43.
-
Loukeris K, Sola R, Baergen RN (2010) Syncytial knots as reflection of placental maturity: references values for 20 to 40 weeks gestational age. Pediatr Dev Pathol 13(4): 305-309.
-
Loardi C, Falchetti M, Prefumo F, Fachetti F, Frusca T (2016) Placental morphology in pregnancy associated with pregravid obesity. J Matern Fetal Neonatal Med 29(16): 2611-2616.
-
Suzuki S, Igarashi M (2008) Clinical significance of pregnancies with succenturiate lobes of placenta. Arch Gynecol Obstet 277(4): 299-301.
-
Biswas S, Ghosh SK (2008) Gross morphological changes of placentas associate with intrauterine growth restriction of fetuses: a case control study. Early Hum Dev 84(6): 357-362.
-
Salafia CM, Yampolsky M, Misra DP, Shlakter O, Haas D, et al. (2010) Placental surface shape, function, and effects of maternal and fetal vascular pathology. Placenta 31(11): 958-962.
-
Soares MJ, Varberg KM, Iqbal K (2018) Hemochorial placentation: development, function and adaptations. Biol Reprod 99(1): 196-211.
-
Barker DJ, Thornburg KL (2013) Placental programming of chorionic diseases, cancer and lifespan: A review. Placenta 34(10): 841-845.
-
Roth LG (1957) Central placenta previa due to succenturiate lobe. Am J Obstet Gynecol 74(2): 447-449.
-
Kumari S, Biswas AK, Giri G (2015) Succenturiate placenta: An incidental finding. J Case Rep Images Gynecol Obstet 1: 1-4.
-
Jeanty P, Kirpatrick C, Verhoogen C, Struyven J (1983) The succenturiate placenta. J Ultrasound Med 2: 9-12.
-
Hata K, Hata T, Aoki S, Takamori H, Takamiya O, et al. (1988) Succenturiate placenta dignosed by ultrasound. Gynecol Obstet Invest 25(4): 273-276.
-
Hamilton WJ, Boyd JD, Mossman HW (1972) the placenta and decidua. In: Hamilton WJ, Mossman HW (Eds.), Human embryology. 4th (Edn.), William &Wilkins Co, Baltimore, pp: 129.
-
Godyn JJ, Hazra A, Gulli VM (2005) Subperitoneal placenta accreta succenturiate in the case of successful near-term extrauterine abdominal pregnancy. Human Pathol 36(8): 922-926.
-
Hess OW (1952) Placenta previa of the succenturiate lobe. American Journal of Obstetrics and Gynecology 64(1): 213-215.
-
Ma JS, Mei X, Niu YX, Li QG, Jiang XF (2016) Risks factors and adverse pregnancy outcomes of succenturiate placenta: A case- control study. J Reprod Med 61(3-4): 139-144.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer