Cancer And Anthropology: A Multidisciplinary Approach To Today’s Enigma
An accentuated systems approach has been considered in Medical Anthropology with respect to theoretical and institutional methodologies to health, illness and healing. Marked changes in distribution, incidence and prevalence of disease, are all related to changes in life expectancy and living patterns, though the latter is related to globalization mainly, significantly among all types of diseases, non-communicable ones are rising with cancer predominating of all. According to WHO, by 2020, there is expected to be some 20 million new cancer cases worldwide. Anthropology has a major role to play in many aspects of cancer, which includes aetiology and protection, epidemiology and prognosis. Human beings are bestowed with a finest gift named culture, which is a significant tool to influence peoples understanding and acceptance of preventive measures. Social and cultural factors needs to be planned in such a manner so that it can be implemented for cancer control programmes ensuring success. Unadventurously, anthropology has pursued to assimilate the biological and physiological with cultural and social parameters. paying attention to the continuous cultural conformations of cancer that exist ‘before cancer’ will increase understanding of how the public health construction of ‘cancer awareness’ relates to everyday health practices such as symptom experience and health care seeking. In today’s date when it is becoming more warning to fight cancer, anthropologists seek to answer to many questions pertaining to its growth and proliferation. The responsibility of a Medical Anthropologist lies in the fact to identify the causes and a better understanding of its prognosis, and if anthropologists come up with explanations, it can be a great measure for prognosis and thus the burden may be lowered and we can win over mortality. The present paper will seek to answer to all the above mentioned facts taking Breast Cancer research as model.
Introduction
In many aspects, cancer is still considered as an enigma, despite the growing advancements in scientific approach to treatment opportunities, a sacredness of a monstrous creature intimidating to rupture and modify life worlds and societies. In a Union address, the former President of United States mentioned, the untiring effort by America to find a cure for Cancer as a moon shot, that invoked Neil Armstrong’s famous words of “giant leap for mankind”. The ‘war on cancer’ representation and the oratory of a cancer cure unite across countries and cultures the many doubts and interrelations of the cancer composite into one single, almost mimicked, global mission of eliminating the disease. It is termed to be a coalescing hunt to understand and conquest cancer. Different social conditions are known to be favourable for Cancer manifestation. Carcinoma has become an increasingly multidimensional social arena where the emphasis is on lifestyle factors and how carcinogens interact in our environment with the understanding about genetic predispositions and contaminations. This complex field is invariably infested with the knowledge and notions of mortality and sense of fate.
Cancer is termed to be a cultural phenomenon that propagates into the society and into intimacies of every day’s life [1], thereby it is often termed as “total social fact”. Many scholars pointed about the presence of the disease in most aspects of social life [2, 3]. The ultimate dichotomy between life and death is carried through moral significance of cancer mythologies, its complexity lies between the endpoints of imagined futures and counterfactually questioned pasts [2]. There are number of research pointing on socio- historical situatedness of experience and regional variability of carcinoma [4]. Medical anthropology has pioneered a research that centres the expressions and performs of cancer, impacting on diverse populations affected by cancer [5].
Cancer is caused by both external factors (tobacco, infectious organisms, chemicals and radiation) and internal factors (inherited mutations, hormones, immune conditions and mutations that occur from metabolism). These causal factors may act together or in sequence to initiate or promote carcinogenesis [6]. Ten or more years often pass between exposure to external factors and detectable cancer. Knowledge about the causes of cancer, and interventions to prevent and manage the disease is extensive. Cancer can be reduced and controlled by implementing evidence based strategies for cancer prevention, early detection and management [7]. One third of cancers could be cured if detected early and treated adequately, based on the observation that treatment is more effective at early stages. In addition, more than 30% of cancers could be prevented simply by behavioral changes that include abstinence from using tobacco, use of healthy diet, maintaining a healthy weight, being physically active and preventing infections that may cause cancer death [8].
In all developed and developing countries, cancer is a major cause of morbidity and mortality [9]. In most of the countries with low socio-economy including India, majority of the population doesn’t have proper access to well regulated cancer care system. Despite numerous advances in treatment, the burden of cancer is increasing worldwide. With a decline in fertility level and increase in life expectancy, the demographic scenario of India is changing. Higher incidence of non-communicable diseases, namely cancer is positively associated with increase of aged population in a country. Both sexes are equally prone to be effected with cancer, with a chance that affects all living cells in the body across all ages. Carcinoma is known to be a multifactorial disease and the process of differentiation differs at different sites. The report from World Cancer documents that cancer rates are set to increase at an alarming rate globally. Approximately, one third to one half of cancer diagnosis is preventable by changes to lifestyle behaviors, amounting to at least 1.1 million avoidable cancer cases per [10].
Prevalence
Breast cancer is the most common cancer diagnosed in women worldwide with over 1.3 million new cases per year. There is a wide variation in the geographical burden of the disease with the highest incidences seen in the more developed regions of the world and the lowest incidences observed in the least developed regions [11, 12, 13]. More recently the incidence of breast cancer has been observed to be increasing in low income countries and data suggests that over the next twenty years the majority of the increase in the worldwide burden of the disease will be due to rising incidences in these countries.
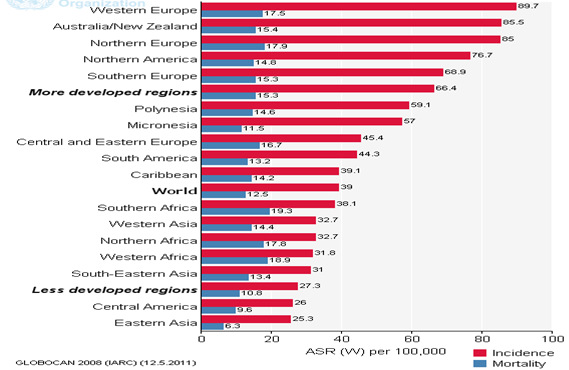
Breast cancer is the most frequent cause of cancer related death for women in both developed and developing countries. The estimated number of deaths globally due to breast cancer in 2008 was 458367. Mortality rates show less geographical variation compared to incidence rates because of the more favorable survival of breast cancer in high-incidence developed regions. The world standardized mortality rate for breast cancer is 12.5 per 100000 and ranges from 17.5 per 100000 in Western Europe to 6.3 per 100000 in Eastern Asia (Figure 1).
The incidence of breast cancer is rising in India and is now the second most commonly cancer diagnosed in women after cervical cancer. It is estimated that in 2008 there were 115251 new cases of breast cancer with an age standardized incidence rate of 22.9 per 100000. It is estimated that by 2030 the number of new cases of breast cancer in India will reach just fewer than 200000 per year [14].
Social Factors behind the Enigma
Over the decades, there are a number of well-established risk factors listed to have increased breast cancer risk. These included age, female reproductive factors, exogenous estrogen exposure, radiation exposure, and other non- genetic factors. The Surveillance Epidemiology and End Results (SEER) cancer statistics review from NCI have suggested that breast cancer rate is increasing with age.
A risk factor is defined as ranging from a lifestyle choice an inherent characteristic that influences a person’s chances of developing a disease (NBOCC, 2009). The definite cause for breast cancer development is far from being unraveled; some factors have been associated with increased risk of developing the disease.
Non-Modifiable Risk Factors
The non-modifiable risk factors constitute characteristics that cannot be changed, and are usually present independent of the individual’s actions.
Gender: breast cancer is predominantly a female disease, with only 1% of the cases occurring in male [15]. Women have an increased risk of developing the disease during their lifetimes compared to men. The reason women develop breast cancer more is not merely because of more breast cells than men, but lies in the fact that their cells are constantly exposed to the growth-promoting effects of the female hormones estrogen and progesterone [16].
Age: increasing age is the single strongest risk factor of breast cancer, apart from the female gender. It is a rare disease before the age of 30 years, after which the incidence rises steeply with increasing age upto about the age of 50 years. Thereafter incidence still increases with age, but at a slower rate. The strong dependence of breast cancer on age, apart from the accumulating genetic damage that occurs during the lifespan, has long been shown to correlate with the duration of hormonal exposure. The chance of getting breast cancer goes up as a woman gets older [17]. About 1 out of 8 invasive breast cancers are found in women younger than 45, while about 2 out of 3 invasive breast cancers are found in women at an 55 or older.
Family History: Family history of breast cancer is an established risk factor of the disease. A woman’s risk of developing breast cancer is higher if her mother, sister or daughter had breast cancer. The risk is higher if one of her family member got the disease before the age of 40 years. About 18% of breast cancers occur in women who have a history of the disease in a first degree relative such as daughters, mother or sisters. Genetic studies have shown that a greater proportion of the familial breast cancer is due to specific germ line mutations within a family pedigree. Depending on the probability of disease occurrence, the genes associated with increased breast cancer may be low penetrance or high penetrance genes. An example of high penetrance genes are the BRCA 1 and BRCA 2 genes whose mutation accounts for about 20% of the familial aggregation of breast cancer, and have been associated with inheritable susceptibility to breast and ovarian cancer. Heritable breast cancers account for 5-10 % of all breast cancers, half of which are related to BRCA 1/2 gene mutations [18].
Genetic Alterations: Inactivating germ line mutations in tumor suppressors and/or oncogenes are the best understood causal mechanism for Genetic susceptibility to cancer, which is triggered in several ways. The genetic events affecting oncogenes often result in increased stimulatory function, whereas those affecting tumor suppressor genes may cause loss of inhibitory function.
Menstrual History: Women who have had more menstrual cycles because they started menstruating at an early age (before age 12) and/or went through menopause at a later age (after age 55) have a slightly higher risk of breast cancer. This may be related to a higher lifetime exposure to the hormones like estrogen and progesterone. Women who are exposed to endogenous sex hormones over a longer period of their life time turn to have increased risk of developing breast cancer. The concept of hormonal carcinogenesis is consistent with epidemiological observations that late menarche and early menopause have a protective effect against breast cancer. This is consistent with the fact that late menarche (onset of menstruation) and/or early menopause (before age of 55 years) have fewer numbers of menstrual cycles and therefore shorter exposure to ovarian hormones during the reproductive years compared to women who have early menarche and/or late menopause [19].
Modifiable Risk Factors
Parity, Reproductive History and Breast Feeding: Parity and an early first full-term pregnancy (FFTP) both have been shown to decrease the long-term breast cancer risk. Nulliparous women are also at increased risk of acquiring breast cancer. Before pregnancy, mammary gland cells are in a vulnerable undifferentiated state but differentiate to functioning milk-producing structures during pregnancy which are refractory to carcinogenesis. It is thought that pregnancies and FFTP in particular, consecutively decrease the pool of vulnerable breast cells. The undifferentiated cells found in the breast of nulliparous women never undergoes through the process of differentiation, retaining a high concentration of epithelial cells that are targets for carcinogens and are therefore susceptible to undergo neoplastic transformation. Breast feeding also reduces BC risk and is thought to exert its effects through hormonal mechanisms.
Post-Menopausal Hormone Therapy (PHT): This therapy also known as hormone replacement therapy (HRT) and menopausal hormone therapy (MHT), is used by many older women to relieve the symptoms of menopause and to help prevent osteoporosis (thinning of the bones). The long-term (more than five years) use of postmenopausal estrogen therapy (ERT) or combined estrogen/progestin hormone replacement therapy (HRT) may be associated with an increase in breast cancer risk [20].
Abortion/Miscarriage History: Some studies have reported an increased risk of breast cancer among women who have had induced abortions. In incomplete pregnancy, the breast is exposed only to the high estrogen levels of early pregnancy and thus may be responsible for the increased risk seen in these women. However, some other studies have found no association between abortions and increased risk of breast cancer.
Physical Activity: Studies have consistently shown that the risk of breast cancer is lower among physically active premenopausal women than among sedentary women. Physical activity during adolescence may be especially protective, and the effect of physical activity may be strongest among women who have at least one full-term pregnancy. A woman’s exposure to estrogen is lowered by exercise, which affects the menstrual cycle and can inhibit ovulation. Research suggests that the less a woman ovulates (that is, the fewer ovulation cycles she has), the lower her risk of breast cancer. So exercise - with its apparent ability to affect estrogen and, likewise, ovulation - may indirectly lower the risk of breast cancer [21]. The preventive effect of physical activity may be due to the non-specific immune stimulation and decreased estrogen levels during recovery as well as delayed onset of menarche.
Obesity: Obesity has been consistently associated with an increased risk of breast cancer among postmenopausal women. This relationship may be mediated again by estrogen production. Fat cells produce some estrogen and obese postmenopausal women, therefore, tend to have higher blood estrogen levels than lean women.
In post-menopausal women obesity has little effect on the serum concentration of estrogen probably due to reduced ovarian estrogen by a negative feedback, hence contributes little changes to the risk of breast cancer. Interestingly, obesity in this group of women has been associated with a decrease of breast cancer risk before menopause, yet the mechanism remains unclear. On the other hand, large studies have recorded that obesity and weight gain increase breast cancer risk in postmenopausal women. The risk is evident among obese women who don’t use hormone replacement (HRT) with the relative risk up to 2. Every 5kg of weight gain since the lowest adult weight increase the breast cancer risk by 8% [22].
In another study, women older than 55 with an increase in body mass of 10kg have been associated with 7% increase in breast cancer risk. The mechanism by which post- menopausal obesity increases the risk for developing breast cancer may due to the unregulated estrogen level by negative feedback, and obesity instigates an increase in the serum concentration of bio available estradiol. Also, sex hormone binding globulin decreases with increase in body mass index (BMI) and might contribute to the increased breast cancer risk.
Alcohol Use and Smoking: The risk of breast cancer is increased among women who consume alcohol or smoke. Studies have shown that consumption of more than two drinks a day leads to an increased level of estrogen in the blood leading to increased risk of breast cancer.
Materials and Methods
Study participants included cases and controls ranging in age from 30-72 years. The cases included subjects visiting the main cancer referral centers of West Bengal; Cancer Center Welfare Home and Research Institute, Kolkata, National Medical College and Hospital, Kolkata. The controls were such selected that none of them had any personal or family history of breast cancer [23].
Data on socio-demography and reproductive performances included parity, age at first child, menarche, menopause, duration of breast feeding, physical activity and diet with detailed information regarding OCP use and abortion incidents. History of breast cancer and oncologic data was retrieved from the medical records after consent from the patients. Demographic data were also collected for all participants.
Data collected were analyzed using SPSS 20.0. Binary logistic regression was used to assess the correlation of any other possible risk factors and the degree of their contribution to breast cancer.
Oral contraceptive use has been defined as use of Oral Contraceptive pills for a total or more than 6 months. Women who never used oral contraceptives or who never used them for less than 6 months were classified as non-users [24].
Results
Stepwise logistic regression (backward conditional) analysis revealed that there are some lifestyle and reproductive variables, which can significantly predict a person’s risk of developing the disease. A person in service as means of occupation is 0.3 times less likely to have breast cancer (OR-0.30, 95% CI=0.129 – 0.682, p<0.001), likewise having no family history of breast cancer reduces the risk of developing the disease by 0.028 times (OR-0.028, 95% CI=0.0009 – 0.092, p<0.0001) [25]. Irregular menstrual periods are seen to increase the risk of breast cancer by 9.40 times (OR-9.40, 95% CI= 2.092 – 42.22, p<0.0001). Prolonged used of oral contraceptives is likely to elevate the breast cancer risk by 2.59 times (OR-2.578, 95% CI= 1.0 – 6.65, p<0.0001). A women’s risk of having breast cancer gets 17.02 times increased if she has history of abortions (OR- 17.02, 95% CI= 2.3 – 143.15, p<0.0001). The potential risk of breast cancer gets increased to 0.26 times if a woman feed her breast for less than 3 months (OR- 0.26, 95% CI= 0.09 – 0.69, p<0.001). Likewise, the risk is modified to 0.19 times (OR- 0.19, 95% CI=0.034 +– 1.07, p<0.01) if a woman undergoes post-menopausal hormone therapy and 6.03 times if she has been operated with hysterectomy (OR-6.03, 95% CI=1.43 – 25.48, p<0.001) [26]. Consumption of alcohol and smoking increases the risk of developing breast cancer by 0.31 times (OR-0.31, 95% CI=0.141 – 0.669, p<0.01) (Table 1).
| Status (Patients) | |
|---|---|
| Education (Graduate) | NS |
| Occupation (Service) | 0.30** (0.129 – 0.682) |
| Marital Status (Unmarried) | NS |
| Family History (No) | 0.028*** (0.0009 – 0.092) |
| Age at Menarche (Below 12 years) | NS |
| Regularity of Menstrual Periods (Irregular) | 9.40*** (2.092 – 42.22) |
| Use of Oral Contraceptive Pills (Yes) | 2.578*** (1.00 – 6.65) |
| Abortion (Yes) | 17.02*** (2.03 – 143.15) |
| Parity (Nulliparity) | NS |
| Number of Issues (Only One) | NS |
| Breast Feeding Duration (>3months) | 0.261** (0.09 – 0.690) |
| Which Breast Fed (Only one) | NS |
| Menopausal Status (Post-menopause) | NS |
| Age at Menopause (Below 50 years) | NS |
| Post-Menopausal Therapy (No) | 0.191* (0.034 – 1.07) |
| Hysterectomy (Yes) | 6.03** (1.426 – 25.48) |
| Smoking/Alcohol (No) | 0.31* (0.141 – 0.669) |
Table 1: Binary Logistic Regression analysis among the various lifestyle, reproductive variables and the patients and controls.
Discussion
Carcinoma of the breast is a threat to a woman, because, it affects the perception of body image and sexuality to a degree greater than any other carcinomas. It not only damages the tissues to the household. Studies from different parts of India has shown that breast cancer has become the number one cancer and the incidence rate of the disease has been faster in younger women, however the causes remain unknown [27]. One of the commonest causes of death in middle-aged women in many developed countries is breast cancer and it is becoming frequent in developing countries as well. Mortality rates from breast cancer have increased during past 60 years in every country [28].
Breast cancer is not just a physical disease; it compels the clients and the health care professionals to face the meaning of their lives. As there is significant role of the breast in a woman’s beauty and sexuality, the responses may include fear of disfigurement, loss of attractiveness, abandonment and death. These fears too may cause some women to delay seeking health care [29].
According to the study of International Agency for Cancer Research, a part of World Health Organization, there was 79,000 breast cancer patients in India in 2001 and the number crossed 80,000 in 2002. The age-standardized rate of breast cancer in India in 2001 and the number crossed 80,000 in 2002. The age standardized rate of the breast cancer in India in 1.75 per 1,00,00 and accounts for 60,600 new cases (19.3% of total female cancers). The estimated cases according to the states in India showed an excess over cervical cancer in 7 states in India [30].
Age and family history are commonly considered to have effect on prognosis and survival of breast cancer. The present study revealed substantial variation in breast cancer risk among the mutation carriers, particularly in terms of age variation and cancer type which basically envisaged that the concomitant effect of genetic variability and environmental factors which eventually modify the expression of the status.
Study of risk factors of breast cancer with marital status might have an impact on the incidence of breast cancer and it was observed that women who never married were at higher risk of breast cancer which has also been reported in Indian context. Since there is a strong interaction between marital status and parity, the increased breast cancer risk associated with single women possibly might be due to nulliparity [31]. The present study also revealed significant association (p<0.0015) with breast cancer and unmarried females in comparison to the controls with an increased risk of 0.19 times (OR-0.192; 95% CI= 0.0527 – 0.6995; p<0.01).
Breast feeding as a protective factor for breast cancer does have a sound biological plausibility. Various pathophysiological mechanisms which are been proposed such as decreased frequency and intensity of ovulation thus maintaining the consistent lower level of estrogen; mobilization of endogenous carcinogens from the ductal and lobular epithelial cell environment, and facilitating the excretion of organochlorides (xenoestrogens) having the same potentials as estrogen [32]. From the population of Delhi it was reported that the mean duration of the sum total breastfeeding for all children as 6.58 years in patients and 7.4 years in controls (OR=1.91; 95% CI, 1.17–3.13) [33]. Similarly, another study from South India has come out that lack of breastfeeding is positively associated with breast cancer [34]. Multicentric trial observed that prolong breastfeeding is associated with reduction in breast cancer risk among reproductive age females [35].
The study executed logistic regression analysis which revealed occupation (housewife), positive family history, irregularity of menstrual periods, use of oral contraceptives, abortions, breast feeding for less than 3 months, post- menopausal hormone therapy, hysterectomy and smoking/ alcohol consumption has been analyzed to be significant predictor variables for breast cancer risk.
Both personal and family histories influence a woman’s risk of developing breast cancer. In other word, woman with first degree relative with breast cancer will have twice the risk than those who do not possesses family history [36]. On the other hand, twin studies indicated that up to 30% of breast cancer cases may be due to genetic factors [37, 38]. This study also emphasized the importance of a positive family history and other lifestyle factors for the breast cancer predisposition. Therefore, the present study envisaged that appropriate genetic counseling and modification of lifestyle factors, symptomatic mutation carriers would be able to minimize the risk for disease susceptibility among the Bengalee Hindu Caste Females of West Bengal, India.
Acknowledgement
The authors are thankful to Indian Council of Social Science Research for providing Travel Grant to support presentation at the conference and for all other support.
References
-
Stacey J (1997) Teratologies: A Cultural Study of Cancer. London, Routledge.
-
Jain R, Strickler HD, Fine E, Sparano JA (2013) Clinical studies examining the impact of obesity on breast cancer risk and prognosis. J Mammary Gland Biol Neoplasia 18(3-4): 257‐266.
-
McMullin J (2016) Comics and cancer: graphic narratives and biolegitimate lives. Med Anthropol Q 30(2): 149- 167.
-
Burke AR, Singh RN, Carroll DL, James CSW, Agostino RBD, et al. (2012) The resistance of breast cancer stem cells to conventional hyperthermia and their sensitivity to nanoparticle-mediated photothermal therapy. Biomaterials 33(10): 2961‐2970.
-
Kumar BV, Lakhotia S, Ankathil R, Madhavan J, Jayaprakash PG, et al. (2002) Germline BRCA1 mutation analysis in Indian Breast/Ovarian cancer families. Cancer Biol Ther 1(1): 18-21.
-
Rajkumar T, Soumittra N, Nancy NK, Swaminathan R, Sridevi V, et al. (2003) BRCA1, BRCA2 and CHEK2 (1100 del C) germline mutations in hereditary breast and ovarian cancer families in South India. Asian Pac J Cancer Prev 4(3): 203-208.
-
Levy-Lahad E, Catane R, Eisenberg S, Kaufman B, Hornreich G, et al. (1997) Founder BRCA1 and BRCA2 mutations in Ashkenazi Jews in Israel: frequency and differential penetrance in ovarian cancer and in breast– ovarian cancer families. Am J Hum Genet 60(5): 1059- 1067.
-
Friedenreich C, Bryant HE, Courneya KS (2001) Case- control study of lifetime physical activity and breast cancer risk. Am J Epidemiol 154(4): 336-347.
-
Yuan JM, Yu MC, Ross RK, Gao YT, Henderson BE (1988) Risk factors for breast cancer in Chinese women in Shanghai. Cancer Res 48(7): 1949-1953.
-
Jemal A, Siegel R, Ward E, Xu, J (2010) Cancer Statistics. CA Cancer Journal for Clinicians. 60(5): 277-300.
-
Kotnis A, Sarin R, Mulherkar R (2005) Genotype, phenotype and cancer: Role of low penetrance genes and environment in tumor susceptibility. J Biosci 30(1): 93-102.
-
Toh GT, Kang P, Lee SSW, Lee DSC, Lee SY, et al. (2008) BRCA1 and BRCA2 Germline Mutations in Malaysian Women with Early-Onset Breast Cancer without a Family History. PLoS One 3(4): 2024.
-
Yip CH (2009) Breast cancer in Asia. Methods Mol Biol 471: 51-64.
-
Ferlay J, Héry C, Autier P, Sankaranarayanan R (2010) Global Burden of Breast Cancer in Breast Cancer. Epidemiology 1: 1-19.
-
Government of India, Ministry of Home Affairs, Office of the Registrar General and Census Commissioner, India.
-
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, et al. (2003) Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 72(5): 1117- 1130.
-
Antoniou AC, Sinilnikova OM, Simard J, Léoné M, Dumont M, et al. (2007). RAD51 135G-->C modifies breast cancer risk among BRCA2 mutation carriers: results from a combined analysis of 19 studies. Am J hum Genet 81(6): 1186-1200.
-
Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, et al. (2000) Environmental and Heritable Factors in the Causation of Cancer--Analyses of Cohorts of Twins from Sweden, Denmark, and Finland. N Engl J Med 343(2): 78-85.
-
Antoniou AC, Wang X, Fredericksen ZS, McGuffog L, Tarrell R, et al. (2010) A locus on 19p13 modifies risk of breast cancer in BRCA1 mutation carriers and is associated with hormone receptor-negative breast cancer in the general population. Nat Genet 42(10): 885- 892.
-
Antoniou AC, Shenton A, Maher ER, Watson E, Woodward E, et al. (2006) Parity and breast cancer risk among BRCA1 and BRCA2 mutation carriers. Breast Cancer Res 8(6): 72.
-
Cox A, Dunning AM, Closas MG, Balasubramanian S, Reed MWR, et al. (2007) A common coding variant in CASP8 is associated with breast cancer risk. Nat Genet 39(3): 352-358.
-
Engel C, Versmold B, Wappenschmidt B, Simard J, Easton DF, et al. (2010) Association of the variants CASP8 D302H and CASP10 V410I with breast and ovarian cancer risk in BRCA1 and BRCA2 mutation carriers. Cancer Epidemiol Biomarkers Prev 19(11): 2859-2868.
-
Metcalfe K, Lynch HT, Ghadirian P, Tung N, Olivotto I, et al. (2004) Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J Clin Oncol 22(12): 2328-2335.
-
Rice JC, Ozcelik H, Maxeiner P, Andrulis I, Futscher BW (2000) Methylation of the BRCA1 promoter is associated with decreased BRCA1 mRNA levels in clinical breast cancer specimens. Carcinogenesis 21(9): 1761-1765.
-
Kelsey JL, Gammon KJ, John EM (1993) Reproductive factors and breast cancer. Epidemiologic Reviews 15(1): 36-47.
-
Kelsey JL, Horn-Ross PL (1993) Breast Cancer: magnitude of the problem and descriptive epidemiology. Epidemiol Rev 15(1): 7-16.
-
Key TJA, Beral V (1992) Sex hormones and cancer. In: Vainio H, et al. (Eds.), Mechanisms of Carcinogenesis in Risk Identification. IARC Scientific Publications, Lyon, pp: 116-255.
-
Harvey AM (1974) Early contributions to the surgery of cancer: William S. Halsted, Hugh H. Young and John G. Clark. Johns Hopkins Med J 135(6): 399-417.
-
Healey CS, Dunning AM, Teare MD, Chase D, Parker L, et al. (2000) A common variant in BRCA2 is associated with both breast cancer risk and prenatal viability. Nature Genetics 26: 362-364.
-
(2011) American Cancer Society. Global Cancer Facts & Figures 2nd (Edn).
-
Hadjisavvas A, Charalambous E, Adamou A, Neuhausen SL, Christodoulou CG, et al. (2004) Hereditary breast and ovarian cancer in Cyprus: identification of a founder BRCA2 mutation. Cancer Genet Cytogenet 151(2): 152- 156.
-
Helewa M, Levesque P, Provencher D, Lea RH, Rosolowich V, et al. (2002) Breast Disease Committee and Executive Committeee and Council, Society of Obstetricians and Gynaecologists of Canada. J Obstet Gynaecol Can 24(2): 164-80.
-
Pakseresht S, Ingle GK, Bahadur AK, Ramteke VK, Singh MM, et al. (2009) Risk factors with breast cancer among women in Delhi. Indian Journal of Cancer 46(2): 132- 138.
-
Meshram II, Hiwarkar PA, Kulkarni PN (2009) Reproductive risk factors for breast cancer: a case control study online. J Hlth Allied Scs 8: 5
-
Gajalakshmi V, Mathew A, Brennan P, Rajan B, Kanimozhi VC, et al. (2009) Breastfeeding and Breast Cancer Risk in India: A Multicenter Case-Control Study. Int J Cancer 125(3): 662-665.
-
Lawrence HK, Marilyn LK, Marion ML, Christine BA (2007) Lifestyle Factors and Survival in Women with Breast Cancer. J Nutr 137(1S): 236S-242S.
-
Sunderam S, Jeseena KJ, Kashyap V, Singh SB, Kumar M (2016) Study on Quality Of Life of Cancer Patients In Relation To Treatment Modality in a Tertiary Health Institute of Jharkhand. IOSR Journal of Dental and Medical Sciences 15(5): 16-20.
-
Mallath MK, Taylor DG, Badwe RA, Rath GA, Shanta V, et al. (2014) The growing burden of cancer in India: epidemiology and social context. The Lancet 15(6): 205- 212.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer