Modified Isolation Method of Mesenchymal Stem Cells from Placental Tissue: Cheap and Effective
Mesenchymal stem cells (MSCs) originating from the human placenta (PMSCs) are promising for cell-based therapeutics. However, the growing demand for PMSCs in clinical trials necessitates high-quality cells in huge numbers. This study aims to create an effective and cheap procedure for PMSC isolation and culture. MSC was isolated from human placental tissue (3- 4mm) by three different methods: explant, collagenase (1 mg/ml), modified method (explant+ 0.1 mg/ml collagenase). PMSC cell morphologies were followed under an inverted microscope for 21 days. PMSCs characterizations were performed using CD44 and CD90 staining and the immunofluorescence method. PMSCs differentiation capacities were determined by alcian blue, oil red, and alizarin red staining. The modified method (explant+collagenase) is based on placenta tissue fragments put in the bottom of the dish and incubated with a culture medium containing %0,1 collagenase type 1. Compared to the traditional explant and enzymatic culture methods that used collagenase 1 mg/ml for incubation in terms of isolation efficiency, cell yield, and proliferative capability. Immunofluorescence staining demonstrated the characterization of mesenchymal stem cells for all isolation techniques. It was determined that the number of cells per area was the lowest in the explant method and the highest in the modified method. Morphological structures of PMSCs isolated using explant, collagenase, and modified method are fusiform and have a fibroblast-like appearance. PMSC isolated in the modified method has higher quality cells with high proliferation ability. It was observed that the modified method especially preserved the cell adhesion ability. It was observed that the isolated PMSCs using a modified method could differentiate into adipogenic, chondrogenic, and osteogenic cell lines in the stainings performed to evaluate their differentiation capacity. Our research identified an effective and high-yield method for producing high-quality PMSCs from the placenta tissue. According to general isolation protocols, the low amount of enzyme used makes it an ideal isolation technique for MSCs for therapeutic use.
Introduction
Mesenchymal stem cells (MSCs) are postnatal stem cells with a hierarchical structure that can self-renew and differentiate into multiple lineages [1]. Due to their biological significance and clinical applications, MSCs have emerged as a prominent issue in modern research. MSCs have distinct properties such as ease of isolation and cultivation, plasticity, and intrinsic tropism toward injured areas. They also have anti-inflammatory and anti-apoptotic activity in damaged tissue and immunomodulatory activity via paracrine function, antimicrobial activity, and bacterial clearance effect. In addition, they have the ability to stimulate neoangiogenesis and activate other resident stem cells [2]. MSCs are an excellent resource for the clinical treatment of certain diseases because of their exceptional properties.
MSCs derived from bone marrow, and adipose tissue has been extensively studied. MSCs derived from bone marrow can differentiate into bone, cartilage, tendon, muscle, adipose tissue, and hematopoietic cell-supporting stroma. As a result, they are candidates for treating patients suffering from bone disorders, heart failure, and other conditions. In addition, because MSCs can be isolated in significant numbers from adults, they have been thoroughly investigated for therapeutic utility. MSCs, for example, promote the ex vivo expansion of hematopoietic stem cells, act as immune modulators, release cytokines and growth factors, and migrate to sites of pathology [3].
Several studies have shown that cells derived from the placenta have MSC-like properties [4, 5, 6]. Unlike bone marrow and adipose-derived MSCs, PMSCs are isolated from the placenta after birth and collected after normal vaginal delivery or a cesarean section. In vitro, PMSCs are easily expandable and can be cryogenically stored, thawed, and reanimated. In addition, human PMSCs develop as plastic- adherent cells, have a surface phenotype similar to other MSCs [7], and can differentiate into multiple lineages [8].
Material and Method
PMSC Culture and growth by Explant Technique
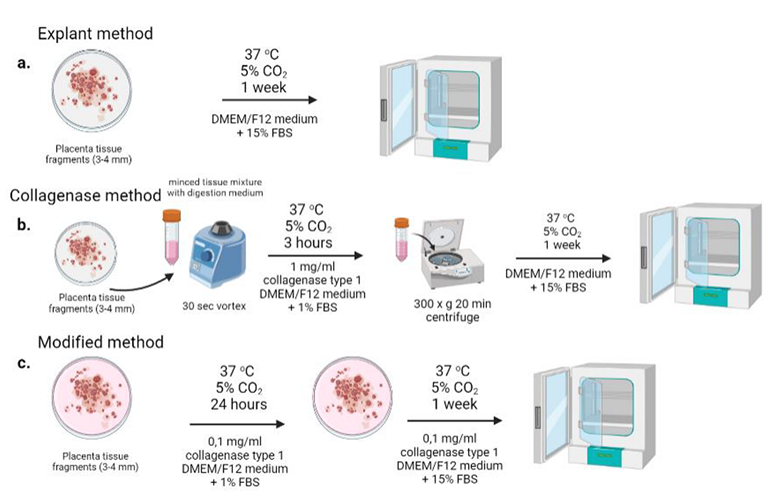
Placenta was obtained from the Obstetrical Department of the Aydin Adnan Menderes University, Turkey. The university’s Ethics Committee approved our study plan, and all donors provided informed consent. The placenta was gathered from healthy full-term women who had an elective cesarean section. In the explant group, the placenta was transferred to the laboratory immediately after it was collected, where it was disinfected and cut into 3-4 mm pieces were seeded onto the surface of a culture dish (Nest, 704004) with High Glucose-Modified Dulbecco’s Eagle MediumF12 (Sigma, D8437) supplemented with 15% (v/v) fetal bovine serum (FBS, Sigma, H1270) [9], 100 units/ml penicillin - 100 mg/ml streptomycin (Sigma, P0781), and amphotericin B (1 µg/ml) incubated at 37°C in a humidified atmosphere containing 5% CO2 for one week. During this time, half of the culture medium was replaced every three days until the cells migrated from the fragment borders and reached about 80% confluence. The experimental design is demonstrated in Figure 1.
PMSC Culture and Growth by Enzymatic Technique
The placenta was placed in a sterile transfer bag that was half full of 5% Penicilin-Streptomicin containing PBS. The cord was washed three times with a carrying solution under sterile conditions to remove blood. The cord was then disinfected in 70% ethanol for 30 seconds and thoroughly rinsed with normal 1% Penicilin-Streptomicin containing saline. The placenta was immersed in a 1 mg/ml collagenase type 1 (Merck, SCR103) digestion medium for 3 hours. After the incubation, digested tissue was centrifuged at 300 × g for 5 sec, and supernatant was collected. This step is repeated two times. Collected supernatants were centrifuged at 300 x g for 20 minutes [10]. The cell pellet was suspended in a culture medium containing DMEM/F12 %15 FBS, %1 Pen- Strep, 1 mg/ml Amphotericin B (Sigma, A2942), then seeded in 25 cm2 flasks (Corning, 430639).
To remove erythrocytes, cells were rinsed with PBS every two days, and the medium was changed. Then, the adherent cells were harvested with 0.25 percent trypsin- Ethylene Diamine Tetra Acetic acid (EDTA, Sigma, T4174) after the cells had reached 90% confluency (Figure 1).
PMSC Culture and Growth by Explant +Enzymatic Technique
As a modified method, 3-4 mm cut placenta tissue fragments were put in the bottom of 10 cm2 dishes and incubated for one week at 37°C with digesting culture medium containing 0.1% collagenase. After incubation, the medium was changed every three days until the 90% cell confluency (Figure 1).
Characterization of PMSC
Images of PMSCs isolated with three different techniques were taken on day 3, day 10, and day 21 under an inverted microscope (Zeiss, Axio Vert.A1, Germany). The images taken are given in Figure 2 in a 10x scale. Thoma slide was used in order to count MSCs. Percentage of MSC cell count was given in Figure 2.
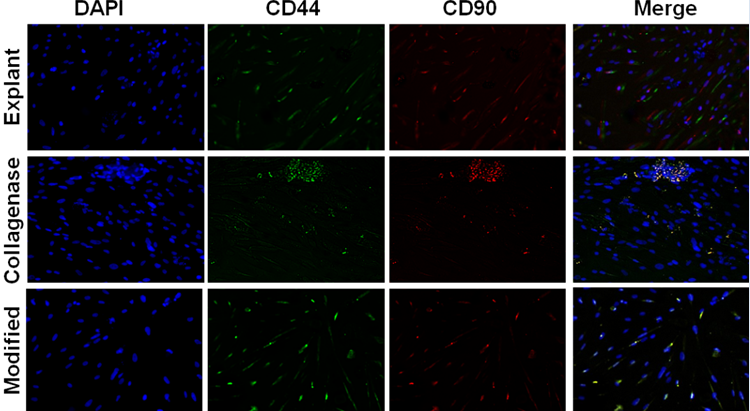
The amounts of cell surface receptors CD44 and CD90 will be evaluated using an immunofluorescence approach to characterize MSC cells [11]. When cells reach a specific size, they are seeded on unique polylysin-coated slides and fixed with 4% paraformaldehyde [12]. After fixation, blocking with PBS containing 1% BSA (Santa Cruz, sc-2323) - washing with PBS - overnight incubation with CD44 (BT Lab, BT-AP01505) and CD 90 (BT Lab, BT-AP01561) primary antibodies - washing with PBS - incubation with FITC (Santa Cruz, sc- 2012) and TR (Santa Cruz, sc-2780) fluorescently labeled secondary antibodies - washing with PBS, respectively, and fluorescence microscope images were obtained.
Alizarin Red, alcian blue, and oil red stainings were performed to observe the ability of the isolated mesenchymal stem cells to transform into different tissue cells [13]. Accordingly, after 24hours of incubation of PMSCs inoculated on 24 well plates (SPL, 30024), inverted microscope images were obtained after the cells were fixed and treated with the relevant dyes.
Results
Morphology of PMSCs
Cell morphologies of mesenchymal stem cells isolated from the placenta by different techniques were checked under an inverted microscope for up to 21 days. Under an inverted phase microscope, spindle-shaped placental MSCs were clearly visible (Figure 2).
![Figure 2: The amounts of cell surface receptors CD44 and CD90 will be evaluated using an immunofluorescence approach to characterize MSC cells [11]. When cells reach a specific size, they are seeded on unique polylysin-coated slides and fixed with 4% paraformaldehyde [12]. After fixation, blocking with PBS containing 1% BSA (Santa Cruz, sc-2323) - washing with PBS - overnight incubation with CD44 (BT Lab, BT-AP01505) and CD 90 (BT Lab, BT-AP01561) primary antibodies - washing with PBS - incubation with FITC (Santa Cruz, sc- 2012) and TR (Santa Cruz, sc-2780) fluorescently labeled secondary antibodies - washing with PBS, respectively, and fluorescence microscope images were obtained.](/fulltextimages/8759/fig_2.png)
Characterization of PMSCs
Immunofluorescence staining was used to examine the immunophenotypes of PMSCs. PMSCs were found to be positive for CD90 and CD44 in explant, collagenase, and modified method. In addition, DAPI staining was used for nuclear-specific dye and controlling to fixed cells (Figure 3).
Multilineage differentiation capability of PMSCs
The ability of MSCs isolated from different techniques to differentiate into three lineages (chondrogenic, adipogenic, and osteogenic) was demonstrated (Figure 4). Alcian blue staining, an essential marker in chondrogenic differentiation, was performed in PMSC cells. Alcian blue is blue in staining for mucopolysaccharides, and mucopolysaccharides are rich in chondrocytes. When the explant, collagenase, and modified methods are compared in Alcian blue staining, it is seen that it is more intense in the explant. Since the extracellular matrix structures are densely present in the explants, forming a connective tissue structure is high. The use of collagenase disrupts the extracellular matrix structure and facilitates the removal of cells from the tissue. It is crucial for reducing cell heterogeneity. Oil red staining is widely used to detect adipogenic structures. When explant, collagenase, and modified methods are compared, it was seen that the differentiation of adipose tissue in cells is more intense in the explant; however the modified method is more effective when looking at the number of cells. Alizarin red staining is widely used for the differentiation potential of stem cells in osteogenic differentiation. Alirazin-red staining, which is used to determine the bone tissue differentiation capacity, was similar to explant and collagenase. It is seen that the osteogenic differentiation capacity is more prominent in the modified method, and it provides cellular stem cell morphology. When explant, collagenase and modified method were evaluated together in terms of stem cell differentiation potential, it was observed microscopically that the modified method was more effective in terms of cell number and preservation of cell morphology.

Discussion
The use of mesenchymal stem cells in clinical practice has grown in popularity recently. As a result, there is a need to develop methods for obtaining MSC from tissues that are not used after surgery and using these cells in various clinical applications. The more affordable and effective these methods become, the more widely they will be used. MSC cells from placental tissue, discarded and not used during birth, were isolated in this study in a shorter time while preserving their properties. When MSC sources isolated from tissues discarded during the surgical procedure are examined in the literature, placenta, umbilical cord, and adipose tissue were discovered [14, 15, 16]. The advantage of the placenta is that it contains both maternal and fetal factors and is a large piece of tissue as a source of stem cells [17].
This study obtained higher-quality MSCs with desired purity and amount by employing several techniques and methods. Choosing an appropriate isolation method is essential in producing PMSCs with optimal quality and high yield to meet clinical demand. There are currently two main methods for isolating PMSCs: the enzymatic and the explant methods. However, there are some issues with both methods [4]. Enzymatic methods influenced MSC biological characteristics such as proliferative capacity [18, 19]. Furthermore, enzymatic methods are more complex, and the operation process will require more time and money.
On the other hand, no matter how much the placenta is washed with PBS in the explant method since it is a bloody tissue, many erythrocyte cells come with mesenchymal stem cells. It is a method based on waiting for the cells to adhere for a long time without medium change. It has been observed that situations that may cause contamination to occur [20]. In addition, it was determined that the number of cells falling from the tissue was less than the other two methods. It was observed in the microscopic images taken on the 3rd, 10th, and 21st days that these cells had less proliferation ability. Considering the enzymatic method [21], it was observed that the number of cells falling from the tissue was high, the proliferation ability of these cells was moderate, and some of the cells lost their adhesion ability due to degradation as a result of enzyme treatment [22].
The modified method of explant + collagenase resulted in the easier separation of MSCs. The critical point is that in the first step of separating, a millimeter-sized placenta was placed on the bottom of a dry flask, followed by enzymatic digestion medium.
When the modified method is used, the number of incoming cells is at an average level, and the proliferation abilities are quite high, supported by the microscopic images. Since the amount of enzyme-treated with the cells was 10 times lower, non-adherent cells due to lysis were not observed. Almost all of the spilled cells adhered effectively to the flask base. At the same time, the small amount of enzyme used makes this method cheaper and more clinically applicable.
Conclusion
Finally, our research discovered an efficient and high- yield method for producing high-quality MSCs from the placenta. Furthermore, our findings show that harvested PMSCs isolated by the modified explant collagenase technique have superior proliferative properties. Furthermore, it is a cheaper technique due to the use of fewer amounts of enzymes according to the classical procedures shows an ideal isolation method of MSCs for clinical applications.
Conflict of Interest
We have no conflict of interests to disclose and the manuscript has been read and approved by all named authors.
Acknowledgment
This work was supported by and Turkish Scientific and Technological Research Council (TUBITAK-120S682) and Aydin Adnan Menderes University Research Grant (ADU- TPF-20001).
References
-
Wei X, Yang X, Han Z, Qu F, Shao L, et al. (2013) Mesenchymal stem cells: a new trend for cell therapy. Acta Pharmacol Sin 34(6): 747-754.
-
Wannemuehler TJ, Manukyan MC, Brewster BD, Rouch J, Poynter JA, et al. (2012) Advances in Mesenchymal Stem Cell Research in Sepsis. J Surg Res 173(1): 113-126.
-
Seshareddy K, Troyer D, Weiss MLBT-M in CB (2008) Method to Isolate Mesenchymal‐Like Cells from Wharton’s Jelly of Umbilical Cord. In: Stem Cell Culture. Academic Press, pp: 101-119.
-
Huang Q, Yang Y, Luo C, Wen Y, Liu R, et al. (2019) An efficient protocol to generate placental chorionic plate-derived mesenchymal stem cells with superior proliferative and immunomodulatory properties. Stem Cell Res Ther 10(1): 301.
-
Pelekanos RA, Sardesai VS, Futrega K, Lott WB, Kuhn M, et al. (2016) Isolation and Expansion of Mesenchymal Stem/Stromal Cells Derived from Human Placenta Tissue. J Vis Exp 6(112): 54204.
-
Choi YS, Park YB, Ha CW, Kim JA, Heo JC, et al. (2017) Different characteristics of mesenchymal stem cells isolated from different layers of full term placenta. PloS one 12: e0172642.
-
Weiss ML, Medicetty S, Bledsoe AR, Rachakatla RS, Choi M, et al. (2006) Human Umbilical Cord Matrix Stem Cells: Preliminary Characterization and Effect of Transplantation in a Rodent Model of Parkinson’s Disease. Stem Cells 24(3): 781-792.
-
Wang HS, Hung SC, Peng ST, Huang CC, Wei HM, et al. (2004) Mesenchymal Stem Cells in the Wharton’s Jelly of the Human Umbilical Cord. Stem Cells 22(7): 1330- 1337.
-
Ranjbaran H, Abediankenari S, Mohammadi M, Jafari N, Khalilian A, et al. (2018) Wharton’s Jelly Derived- Mesenchymal Stem Cells: Isolation and Characterization. Acta Med Iran 56(1): 28-33.
-
Tsagias N, Koliakos I, Karagiannis V, Eleftheriadou M, Koliakos GG (2011) Isolation of mesenchymal stem cells using the total length of umbilical cord for transplantation purposes. Transfus Med 21(4): 253-261.
-
Schieker M, Pautke C, Haasters F, Schieker J, Docheva D, et al. (2007) Human mesenchymal stem cells at the single-cell level: simultaneous seven-colour immunofluorescence. J Anat 210(5): 592-599.
-
Parodi V, Jacchetti E, Bresci A, Talone B, Valensise CM, et al. (2020) Characterization of mesenchymal stem cell differentiation within miniaturized 3d scaffolds through advanced microscopy techniques. Int J Mol Sci 21(22): 1-21.
-
Ciuffreda MC, Malpasso G, Musaro P, Turco V, Gnecchi M (2016) Protocols for in vitro Differentiation of Human Mesenchymal Stem Cells into Osteogenic , Chondrogenic and Adipogenic Lineages. Methods Mol Biol 1416: 149- 158.
-
In ’t Anker PS, Scherjon SA, Kleijburg-van der Keur C, De Groot-Swings GMJS, Claas FHJ, et al. (2004) Isolation of Mesenchymal Stem Cells of Fetal or Maternal Origin from Human Placenta. Stem Cells. 22(7): 1338-1345.
-
Hassan G, Kasem I, Antaki R, Mohammad MB, AlKadry R, (2019) Isolation of umbilical cord mesenchymal stem cells using human blood derivatives accompanied with explant method. Stem cell Investig 6: 28.
-
Bunnell BA, Flaat M, Gagliardi C, Patel B, Ripoll C (2008) Adipose-derived stem cells: isolation, expansion and differentiation. Methods 45(2): 115-120.
-
Mathews S, Lakshmi Rao K, Suma Prasad K, Kanakavalli MK, Govardhana Reddy A, et al. (2015) Propagation of pure fetal and maternal mesenchymal stromal cells from terminal chorionic villi of human term placenta. Sci Rep 5(1): 10054.
-
Yoon JH, Roh EY, Shin S, Jung NH, Song EY, et al. (2013) Comparison of explant-derived and enzymatic digestion- derived MSCs and the growth factors from Wharton’s jelly. Biomed Res Int, pp: 428726.
-
Yi X, Chen F, Liu F, Peng Q, Li Y, et al. (2020) Comparative separation methods and biological characteristics of human placental and umbilical cord mesenchymal stem cells in serum-free culture conditions. Stem Cell Res Ther 11(1): 183.
-
Salehinejad P, Moshrefi M, Eslaminejad T (2020) An Overview on Mesenchymal Stem Cells Derived from Extraembryonic Tissues: Supplement Sources and Isolation Methods. Stem Cells Cloning 13: 57-65.
-
Han YF, Tao R, Sun TJ, Chai JK, Xu G, et al. (2013) Optimization of human umbilical cord mesenchymal stem cell isolation and culture methods. Cytotechnology 65(5): 819-827.
-
Gittel C, Brehm W, Burk J, Juelke H, Staszyk C, et al. (2013) Isolation of equine multipotent mesenchymal stromal cells by enzymatic tissue digestion or explant technique: comparison of cellular properties. BMC Vet Res 9(1): 221.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer