Intramural and Metamorphosed-Seminoma Testis
Editorial
Seminoma is a frequently discerned, primary testicular germ cell tumour which may configure as a component of mixed germ cell tumour. Primary mediastina seminoma may also be discerned. Extra-gonadal neoplasms simulating seminoma may be delineated in diverse sites as pineal gland and are designated as germinoma. Seminoma commences from transformed gonocytes engendering germ cell neoplasia in situ (GCNIS). Cells configuring germ cell neoplasia in situ are posited to arise from delayed maturation of primordial germ cells or gonocytes along with accrual of additional set of chromosomes with emergence of polyploid, transformed germ cells [1, 2]. Subsequently, seminoma is engendered post puberty wherein a germ cell neoplasm in situ evolves into an intra-tubular seminoma followed by invasive seminoma [1, 2].
Factors contributing to emergence of seminoma are distinctive family history of tumour emergence, preceding germ cell tumour, cryptorchidism, subfertility or disorders associated with immunodeficiency [1, 2]. Testicular seminoma exhibits genomic mutations of KIT gene and iso- chromosome from short arm of chromosome 12, i (12p) [1, 2]. Seminoma manifests as a unilateral, palpable tumefaction and emerges in young subjects, commonly between 30 years to 49 years. Neoplasm is exceptionally discerned in subjects >70 years or <20 years [1, 2].
Generally, seminoma represents with a distinct tumour mass [1, 2]. Occasionally, clinical symptoms may ensue due to distinct tumour metastasis. Symptoms associated with paraneoplastic manifestations as limbic encephalopathy, hypercalcemia, polycythemia or exophthalmos are exceptional [1, 2]. Tumour metastases initially emerge within retroperitoneal lymph nodes with subsequent incrimination of mediastinal and cervical lymph nodes. Visceral metastases are usually delayed [1, 2]. Upon gross examination, well defined, homogeneous, uniform, solid, grey/white or off white testicular mass is expounded. Superficial surface appears nodular and lobulated with the occurrence of multiple nodules. Focal necrosis or haemorrhage is minimal. Spontaneous tumour regression denominates a scar [1, 2]. Frozen section exhibits fibrous bands infiltrated with small lymphocytes and clear tumour cells [1, 2]. Intra-operative or touch prep smears exemplify enlarged tumour cells incorporated with abundant cytoplasm intermingled with numerous lymphocytes. Alternating dense and light, striped background or ‘tigroid pattern’ may be discerned in air dried smears stained with Romanowsky- based May-Grunwald -Giemsa or Diff-Quik stain [1, 2].
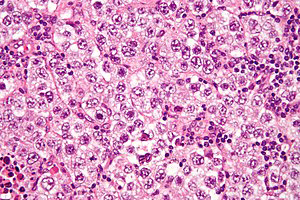
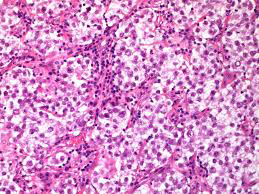
Cytological evaluation exhibits a dis-cohesive population of enlarged tumour cells incorporated with moderate cytoplasm, spherical, minimally irregular nuclei and singular or multiple, prominent nucleoli. Tumour cells appear admixed with miniature, mature lymphocytes [1, 2]. Hyper-cellular aspirates classically demonstrate “tigroid smears” composed of reticulated, granular substance intermingled with clear cells or tumour cells with enhanced intracytoplasmic glycogen [1, 2]. Upon microscopy, sheets of tumour cells appear segregated with fibrous tissue septa. A lobular configuration may be discerned [1, 2]. Characteristically, tumefaction exhibits a distinctive tumour perimeter. Typically, tumour cells are glycogen rich and appear pale.
Eosinophilic cells may be observed. Cellular membrane is well defined and cellular perimeter is distinct [1, 2]. Tumour cell nuclei are polygonal with flattened edges, configuring a ‘squared off’ appearance with singular or multiple, prominent, centric nucleoli. Nuclear overlapping is usually absent. Tumour cells are imbued with clear cytoplasm, spherical to polygonal nuclei and prominent, centric nucleoli [1, 2]. Tumour parenchyma is traversed with distinct fibrous tissue septa [1, 2]. Tumour parenchyma is infiltrated with a prominent, chronic inflammatory infiltrate composed of T lymphocytes and plasma cells. Germinal centres may be configured. Epithelioid cell granulomas may be discerned. Foci of intercellular oedema with configuration of micro- cystic spaces and coagulative necrosis can be exemplified [1, 2]. Multinucleated syncytiotrophoblastic cells can generate β-HCG [1, 2]. Foci of intra-tubular seminoma may concur with invasive seminoma. Infrequently, tumour configurations as inter-tubular, corded growth, micro-cystic, tubular or signet-ring appearance may be enunciated [1, 2]. ‘Anaplasia’ associated with enhanced mitotic activity or cellular and nuclear pleomorphic appears non concurrent with prognostic outcomes. ‘Regressed’ or burnt out seminoma is accompanied by fibrosis and sclerosis [1, 2]. Miniature seminomas <4 centimetres are uncommonly associated with lymphatic and vascular infiltration. Infiltration of rete testis can occur due to stromal invasion or pagetoid tumour spread wherein direct stromal invasion significantly impacts prognostic outcomes [1, 2] (Figures 1 & 2, Table 1).
| Node | Metastasis | |
|---|---|---|
| Tis: Tumour in situ confined to seminiferous tubules | ||
| TX: Tumour cannot be assessed | NX: Lymph nodes cannot be assessed | |
| T0:No evidence of primary tumour | N0:Lymph node metastasis absent | M0: Distant metastasis absent |
| T1:Tumour extends beyond seminiferous tubules, confined to testis •T1a: Tumour <3cm •T1b: Tumour>3cm | N1: Lymph node metastasis in up to 5 nodes <2cm | M1: Distant metastasis present •M1a: Metastasis in lungs or distant lymph nodes apart from retroperitoneal nodes •M1b: Metastasis in distant viscera as liver or bones, apart from distant nodes and lungs |
| T2: Tumour confined to testis, rete testis or infiltrates testicular blood vessels, lymphatics, epididymus, hilar soft tissue or tunica vaginalis | N2: Single lymph node metastasis or retroperitoneal nodal mass between 2cm to 5cm, peri-capsular infiltration or deposits in >5 nodes | |
| T3: Tumour extends to spermatic cord | N3:Single or matted lymph nodes or retroperitoneal nodal metastasis >5cm | |
| T4: Tumour extends to scrotum |
Table 1: TNM Classification of Testicular Germ Cell Tumours [1,2]. Serum tumour markers as LDH, AFP and β-HCG can be evaluated an
Table 1: TNM Classification of Testicular Germ Cell Tumours [1, 2]. Serum tumour markers as LDH, AFP and β-HCG can be evaluated and categorised as
- SX: Tumour markers remain un-assessed
- S0: Tumour markers within normal limits
- S1: Single tumour marker is mildly increased
- S2: Single tumour marker is significantly increased
- S3: Single tumour marker exhibits extremely elevated values [1, 2].
Seminoma is immune reactive to OCT3/4, CD117, D2- 40, PLAP, SALL4 or SOX17. Tumour cells can be stained with Periodic acid Schiff’s stain. Seminoma is immune non-reactive to CD30, AFP, glypican 3, HCG, EMA, AE1/AE3, CK7, inhibin, p63, PAX8 or GATA3 [3, 4]. Seminoma requires segregation from neoplasms such as embryonal carcinoma, spermatocytic tumour, solid variant of yolk sac tumour, Sertoli cell tumour, lymphoma or granulomatous orchitis [3, 4]. Seminoma can be appropriately discerned with ultrasonography. Plain radiography or computerized tomography of thoracic and abdominal cavity may be beneficial [3, 4].
Ultrasonography exhibits a uniform, well defined and hypo echoic tumefaction. Testicular micro-lithiasis may be discerned [3, 4]. Tumour markers such as serum LDH, AFP and β-HCG can be optimally evaluated. Serum LDH, PLAP and β-HCG may be elevated [3, 4]. Serum AFP appears elevated in hepatic disease or with accompanying non-seminomatous component [3, 4]. Stage I clinical disease is associated with superior prognosis. Incriminated subjects beyond > 40 years and advanced disease stage with accompanying non- pulmonary metastasis demonstrate inferior prognostic outcomes [3, 4]. Seminoma can be appropriately being managed with surgical extermination. Radical orchiectomy is optimal for treating primary testicular seminoma [3, 4]. Stage I disease can be subjected to cogent surveillance protocols. Seminoma is a radiosensitive neoplasm. Tumefaction of advanced grade can be treated with radiotherapy or platinum based chemotherapy [3, 4]. Residual disease following chemotherapy can be subjected to retroperitoneal lymph node dissection [3, 4].
References
-
Cedeno JD, Dawn EL, Stephen WL (2022) Testicular Seminoma. Stat Pearls International.
-
Berney DM, Ian C, Vishal R, Holger M, John RS, et al. (2022) an introduction to the WHO 5th edition 2022 classification of testicular tumours. Histopathology.
-
Tourne M, Radulescu C, Yves A (2019) Testicular germ cell tumours: Histopathological and molecular features. Bull Cancer 106(4): 328-341.
-
Nestler T, Baunacke M, Desiree D, Nicolas VL, Christer G et al. (2019) Testicular cancer guideline adherence and patterns of care in Germany: A nationwide survey. Eur J Cancer Care (Engl) 28(1): e12917.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer