Hailey-Hailey Disease with Nail Changes Preceding the Skin Changes- A Case Report
Hailey-Hailey disease is an uncommon genodermatoses characterised by recurrent vesicular and erosive lesions that favour the intertriginous areas, especially axilla and groin. Longitudinal leukonychia in multiple finger nails may appear concurrently, prior to or may follow the skin lesions in this disease (two-third patients). Here we are presenting a case of Hailey-Hailey disease in a 40 years old male with nail changes preceding the skin manifestations.
Introduction
Hailey-Hailey disease is a rare genodermatoses characterised by recurrent vesicular and erosive lesions that favour the intertriginous areas, especially axilla and groin. The disease was first described by Hailey brothers in 1939 as “familial benign chronic pemphigus” [1]. Here we report a case of Hailey-Hailey disease in a 40 years old male with nail changes preceding the skin manifestations.
Case Report
A 40 years old male presented with itchy vesiculobullous eruptions over both axilla and groins for last 4 years and asymptomatic longitudinal white bands in multiple finger nails for last 5 years which was of gradual onset. The vesicles ruptured spontaneously leading to formation of erosions. Recurrent exacerbation was reported during summer. There was no period of remission throughout the entire course of the disease. There was history of using local indigenous ointments over the lesions on and off with healing of few lesions leaving hyperpigmented spots. There was no history of similar complaints in any other family member.
On cutaneous examination, few intact vesicles containing clear fluid on erythematous base, few erosions and multiple hyperpigmented macules and patches were present over bilateral groins and axilla (Figure 1a). Asymptomatic longitudinal white bands (longitudinal leukonychia) were observed in multiple finger nails (Figure 1b). There was no involvement of neck folds, antecubital fossae, popliteal fossae, palms, soles and mucous membranes.
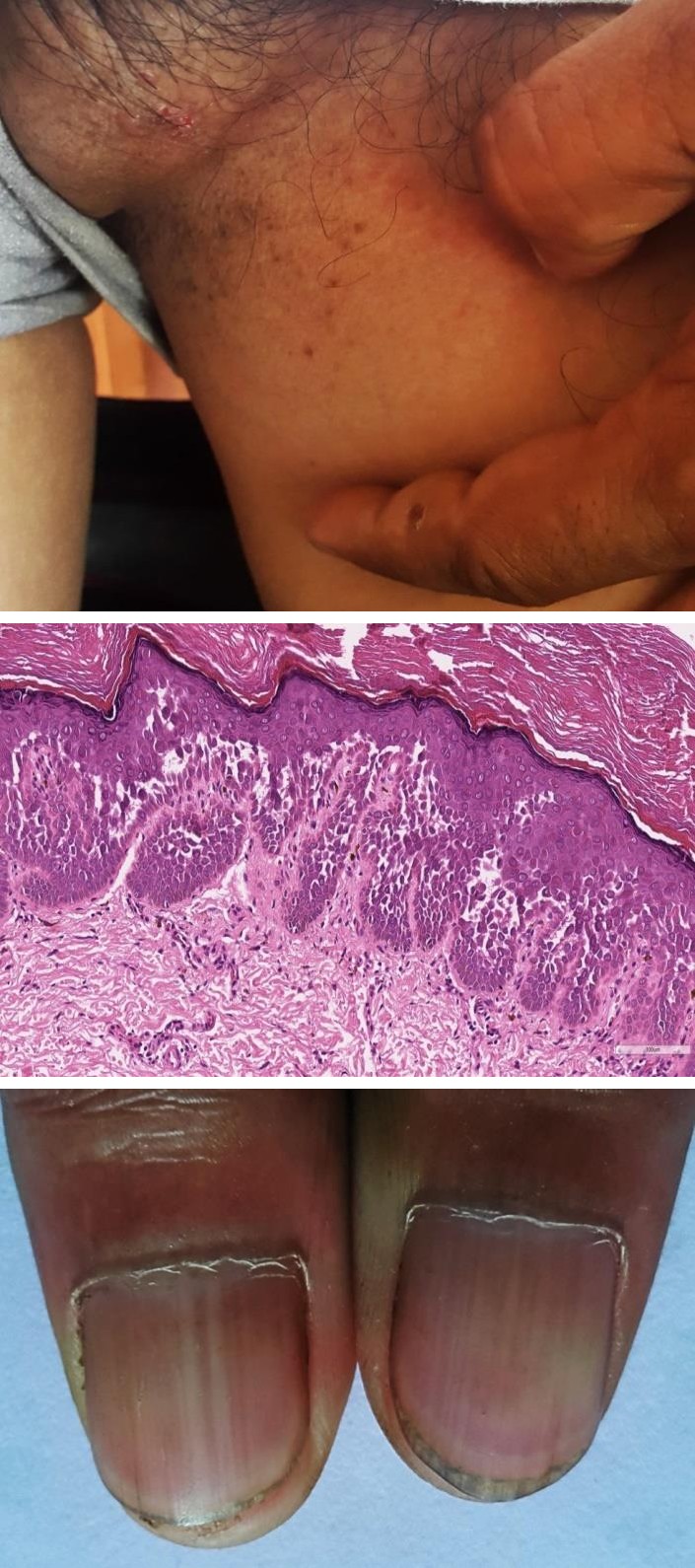
Figure 1(a): Showing few intact vesicles containing clear fluid on erythematous base, few erosions and multiple hyperpigmented macules and patches over left groin.
Figure 1(b): Showing longitudinal white bands in bilateral thumbnails.
All routine haematological and biochemical investigations were normal. A potassium hydroxide wet mount preparation from the axillary eruption did not show any fungal hyphae. Tzanck smear showed a few acantholytic cells. Histopathological examination (H.P.E) of a punch biopsy specimen from groin demonstrated intraepidermal bullae containing many acantholytic cells imparting a dilapidated brick wall appearance (Figure 2). Direct immunofluorescence was negative. On the basis of clinical and histological findings, a diagnosis of Hailey- Hailey disease was made. He was prescribed oral and topical antibiotics. The patient was lost to follow up.
Discussion
Hailey-Hailey disease is a rare autosomal dominant disorder with incomplete penetrance. Family history is obtained in about two-third of the patients [2]. However in our case, no positive family history was reported. The lesions usually develop during second and third decade of life and affect both sexes equally [2]. Our patient was a 45 years old male. The disease is caused by mutation of the ATP2C1 gene on chromosome 3q21-q24 which encodes a calcium channel that is localized to the Golgi apparatus of keratinocytes. It sequesters calcium within Golgi apparatus. There is a major role of cytosolic calcium concentration in keratinocyte differentiation [3]. Increased intracellular calcium concentration leads to expression of involucrin, a protein which envelops keratinocytes and responsible for keratinocyte adhesion. Alberg, et al. found decreased level of involucrin in Hailey- Hailey disease [4]. In affected individuals, there is a loss of cohesion between keratinocytes (acantholysis) and development of vesicles.
Recurrent, fragile vesicles and erosions over the intertriginous areas (axilla, groin, lateral aspect of neck, inframammary area and perianal region) is the characteristic clinical finding [2]. Scalp, antecubital fossae, popliteal fossaeare less frequently involved and involvement of oral, vulvar and conjunctival mucosa is rare [5]. However, in our patient, bilateral groin and axillary lesions were seen. The cutaneous lesions can be pruritic, painful and malodorous. Healing occurs without scarring leaving post inflammatory hyperpigmentation [2]. Painful intertriginous erosions, malodorous discharge and pruritus may interfere with physical and professional activities and give rise to psychosocial distress of the patients. Itching was the major complaint in our patient and few lesions healed with hyperpigmented macules and patches following application of indigenous ointments. Longitudinal white bands (longitudinal leukonychia) in the fingernails may serve as a diagnostic clue which was seen in 71% cases in a study by Burge SM, et al. [2]. In our case, longitudinal white bands in multiple finger nails appeared prior to the onset of cutaneous lesions. The disease has a chronic course with periods of exacerbation and remission [2]. In our patient, the lesions were continuously present throughout the course of the disease, without any period of remission. The disease can be triggered by friction, heat, sweating, infection and stress.
Differential diagnosis includes intertrigo, eczema, Darier disease and pemphigus vegetans. The treatment of Hailey-Hailey disease is challenging. Avoidance of potential is aggravating factors, such as friction and sweating, maintaining weight at appropriate levels, comfortable loose clothing to minimize frictionare the conservative mode of treatments. Various treatment modalities include topical corticosteroids, antimicrobials, calcipotriol, tacrolimus and retinoids, systemic antimicrobials, retinoids, dapsone, immunosuppressants like methotrexate and cyclosporine, botulinum toxin, dermabrasion, carbon dioxide laser, photodynamic therapy with variable efficacies [6, 7, 8, 9, 10]. Wide excision of the involved area with replacement by split graft is indicated in recalcitrant cases [11].
Conclusion
Asymptomatic white bands in finger nails (longitudinal leukonychia) may appear concurrently, prior to or may follow the skin lesions in Hailey- Hailey disease (two-third patients). In our case, nail changes preceded the appearance of skin lesions by 1 year. Hence, nail changes may serve as a diagnostic window for the early diagnosis of this rare genodermatoses.
References
-
Hailey H, Hailey H (1939) Familial benign chronic pemphigus. Arch Dermatol 39: 679-685.
-
Burge SM (1992) Hailey-Hailey disease: the clinical features, response to treatment prognosis. Br J Dermatol 126(3): 275-282.
-
Hakuno M, Shimizu H, Akiyama M, Amagai M, Wahl JK, et al. (2000) Dissociation of intra- and extracellular domains of desmosomalcadherins and E-cadherin in Hailey-Hailey disease and Darier's disease. Br J Dermatol 142(4): 702-711.
-
Aberg KM, Racz E, Behne MJ, Mauro TM (2007) Involucrin expression is decreased in Hailey-Hailey keratinocytes owing to increased involucrin mRNA degradation. J Invest Dermatol 127(8): 1973-1979.
-
Vaclavinkova V, Neumann E (1982) Vaginal involvement in familial benign chronic pemphigus (Morbus Hailey-Hailey). Acta Derm Venereol 62(1): 80-81.
-
Bianchi L, Chimenti MS, Giunta A (2004) Treatment of Hailey-Hailey disease with topical calcitriol. J Am Acad Dermatol 51(3): 475-476.
-
Rabeni EJ, Cunningham NM (2002) Effective treatment of Hailey-Hailey disease with topical tacrolimus. J Am Acad Dermatol 47(5): 797-798.
-
Berger EM, Galadari HI, Gottlieb AB (2007) Successful treatment of Hailey-Hailey disease with acitretin. J Drugs Dermatol 6(7): 734-736.
-
Berth-Jones J, Smith SG, Graham-Brown RA (1995) Benign familial chronic pemphigus (Hailey-Hailey disease) responds to cyclosporin. Clin Exp Dermatol 20(1): 70-72.
-
Don PC, Carney PS, Lynch WS, Zaim MT, Hassan MO (1987) Carbon dioxide laser abrasion: a new approach to management of familial benign chronic pemphigus (Hailey-Hailey disease). J Derm Surg Oncol 13(11): 1187-1194.
-
Menz P, Jackson IT, Connolly S (1987) Surgical control of Hailey -Hailey disease. Br J Plast Surg 40: 557-561.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling