Scedosporium Apiospermum-Mediated Deep Cutaneous Mold Infection in an Immunosuppressed Patient
Scedosporium apiospermum is a ubiquitous environmental mold increasingly implicated in opportunistic fungal infections among solid organ transplant recipients. We report the unusual case of a 65-year old woman on triple immunosuppression with a deep cutaneous mold infection caused by S. apiospermum four years after renal transplant.
Case Report
A 65-year-old African American woman with a past medical history of type-2 diabetes mellitus, hypertension, hyperlipidemia, and renal transplantation presented to a local dermatologist’s office with an enlarging ulcerated lesion on her left lower extremity for several weeks. The lesion began as a collection of small ulcerations on the medial aspect of her left leg. Skin biopsy at that time reportedly demonstrated suppurative granulomatous dermatitis with associated ruptured follicular epithelium. Special stains for fungus and acid-fast bacilli were negative, prompting management as an inflammatory process with topical steroids. With repeated application of topical clobetasol, the patient noted increased friability, bleeding, and growth of the lesion over time.
Nine months later, the patient was referred to our dermatology clinic due to worsening of her left leg lesion and increased pain. The patient also reported a twenty-pound weight loss over the past year, but denied any fevers, chills or other signs of systemic infection. Since her kidney transplant in 2015, the patient remained on prednisone, tacrolimus, and mycophenolate mofetil for immunosuppression. Physical examination revealed numerous, painful, verrucous, hyperpigmented papules coalescing into larger plaques with multiple superficial ulcerations on the anterior and medial aspect of the patient’s lower left leg (Figure 1). No grains were noted. Given the prior biopsy results, our differential diagnosis included infection and a neutrophilic dermatosis such as verrucous pyoderma gangrenosum.
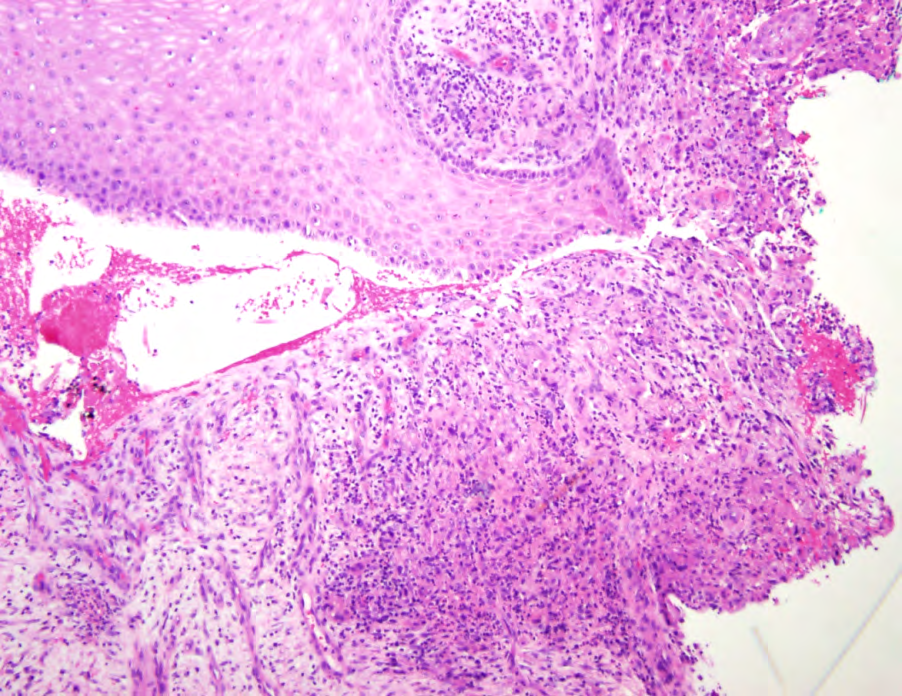
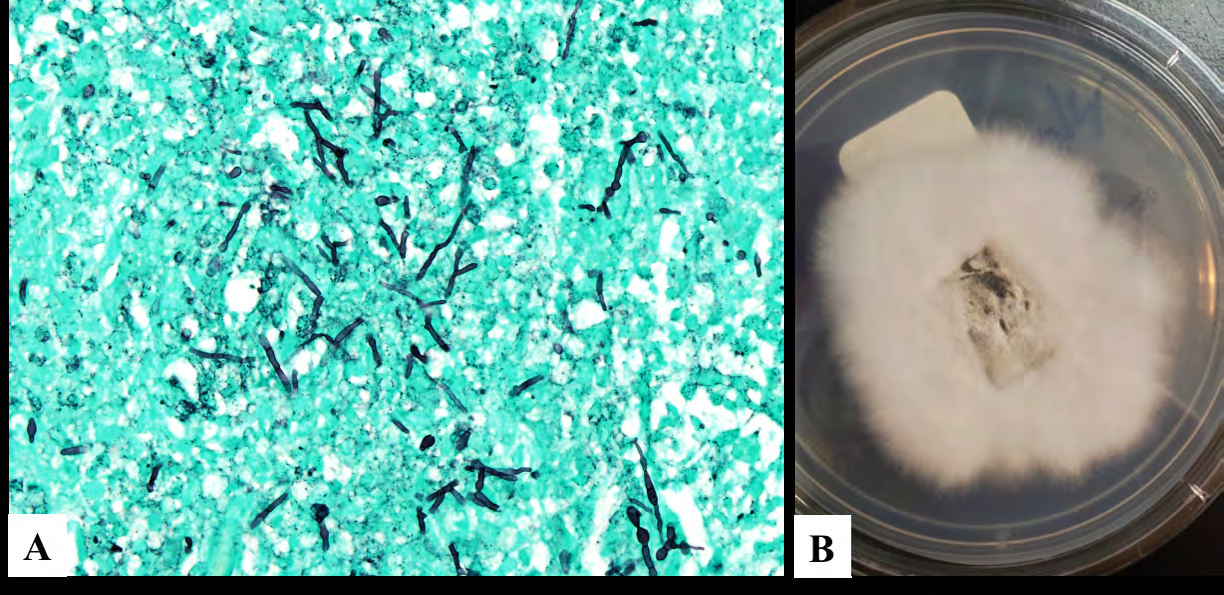
Purulent drainage and friable tissue was evident with the punch biopsy procedure. Skin biopsy demonstrated irregular epidermal hyperplasia with variable invaginations suggesting possible early sinus tract formation and a dermal suppurative and granulomatous dermatitis (Figure 2). Numerous hyphal elements and yeast forms were identified on Gomori methenamine silver (GMS) stain, consistent with a deep cutaneous fungal infection (Figure 3A). Tissue fungal culture grew white rabbit-fur-like mold that later turned into a house-mouse gray color with acute-angle branching septate hyphae seen under microscopy, which speciated as S. apiospermum (Figure 3B). Susceptibility testing confirmed sensitivity to voriconazole. The patient was referred to our infectious disease colleagues who initiated treatment with a six-month course of voriconazole 200 mg twice daily. Marked improvement was noted within one-month of initiating treatment, and no surgical debridement was required, distinguishing this deep Scedosporium cutaneous infection from Scedosporium eumycetoma. Therapeutic voriconazole levels were carefully monitored during this period, given the known drug interaction between tacrolimus and voriconazole. After five months of therapy, the infection resolved with scarring and dyspigmentation (Figure 1).

Figure 1: Deep cutaneous Scedosporium infection at presentation to our clinic, 9-months after initial local dermatologist visit. Verrucous hyperpigmented papules coalescing into fluctuant plaques overlying the left lower extremity. Patient’s left lower extremity before treatment (left inset) and five months after treatment with voriconazole (right inset).
Discussion
S. apiospermum is a ubiquitous opportunistic saprophytic mold most frequently associated with eumycetoma in temperate climates; however, it can also cause deep localized erosive infection and life-threatening disseminated disease in immunosuppressed patients [1, 2]. Indeed, a recent single- center, retrospective study of transplant recipients between 2000 and 2010 found that two-thirds of their patients were infected with S. apiospermum, consistent with prior reports of this mold’s predilection for this patient population [3]. Notably, S. apiospermum is inherently resistant to traditional antifungals such as amphotericin B, allowing it thrive despite conventional antifungal prophylaxis regimens targeting Aspergillus and Candida [4]. Consequently, the mortality of S. apiospermum infection in immunocompromised patients ranges from 60 to 100% [5]. It is therefore paramount to always have a high index of suspicion for possible infection with opportunistic saprophytic molds in susceptible patients, with attention to S. apiospermum infection, in particular, and to not disregard these culture results as contaminants.
This case highlights the importance of accurate identification and appropriate therapeutic intervention required for S. apiospermum mediated deep cutaneous mold infection in high-risk patients. Given the overlap in clinical presentation of deep cutaneous mold infection with non- infectious entities such as verrucous pyoderma gangrenosum or granulomatous disease such as sarcoidosis or necrobiosis lipoidica, one could easily misdiagnose the early stages of infection, where targeted antifungal intervention would be of highest yield. Left untreated, S. apiospermum infection can progress to brain abscess secondary to systemic dissemination; treated in late stage, the affected area of localized infection may heal with substantial scarring, as was seen in our case [6].
Microbiological diagnosis of Scedosporium infection is still largely dependent upon culture and morphological characterization, followed by susceptibility testing to guide antifungal selection. Emerging reports suggest that voriconazole is usually the drug of choice for S. apiospermum infections, but close therapeutic drug monitoring is required in organ transplant patients given the risk of drug-drug interactions with concurrent immunosuppressants [7]. Although the paucity of data regarding treatment response strategies precludes the formation of uniform management guidelines, adjunctive surgical debridement and drainage of lesions may be indicated in some cases.
As the diagnosis of deep cutaneous mold infection grows in recognition, so does the list of implicated fungal etiologies. Consideration of S. apiospermum as a causative agent is of particular importance given the challenges associated with its management and the potentially dire consequences of misdiagnosis. As the prevalence of acquired immunosuppression is rising, increased vigilance is required for the accurate diagnosis and prompt treatment of S. apiospermum mediated deep cutaneous mold infection in immunocompromised patients.
References
-
Goldman C, Akiyama MJ, Torres J, Louie E , Meehan SA (2016) Scedosporium apiospermum infections and the role of combination antifungal therapy and GM- CSF: A case report and review of the literature. Medical mycology case reports 11: 40-43.
-
Cortez KJ, Roilides E, Quiroz-Telles F, Meletiadis J, Antachopoulos C, et al. (2008) Infections Caused by Scedosporium spp. Clinical microbiology reviews 21: 157-197.
-
Johnson LS, Shields RK, Clancy CJ (2014) Epidemiology, clinical manifestations, and outcomes of Scedosporium infections among solid organ transplant recipients. Transpl Infect Dis 16: 578-587.
-
Lamaris GA, Chamilos G, Lewis RE, Safdar A, Raad, II , Kontoyiannis DP (2006) Scedosporium infection in a tertiary care cancer center: a review of 25 cases from 1989-2006. Clin Infect Dis 2006;43(12): 1580-1584.
-
Farina C, Gotti E, Suter F, Goglio A (2006) Scedosporium apiospermum soft-tissue infection: a case report and review of kidney transplant literature. Transplant Proc 38(5): 1333-1335.
-
Sharma RB, O’Donnell AC, Stamateris RE, Ha B, McCloskey KM, et al. (2015) Insulin demand regulates beta cell number via the unfolded protein response. J Clin Invest 125(10): 3831-3846.
-
Troke P, Aguirrebengoa K, Arteaga C, Ellis D, Heath CH, et al. (2008) Treatment of scedosporiosis with voriconazole: clinical experience with 107 patients. Antimicrobial agents and chemotherapy 52: 1743-1750.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling