Women's Eruptive Genital Syringoma: A Case Observed at the Dermatology-Venerology Department of the National Hospital University Center of Bangui, Central African Republic
Syringoma is often localized to the face. The aim of this work is to describe the first case of female genital syringoma observed in Bangui. Miss B, aged 19 years old, living in Bangui, consulted on September 13, 2019 for a genital pruritis. There is a history of carcinoma in her older sister. The physical examination shows a general good condition, elastic vulvar edema with a rash of small papules. The hypotheses of early condyloma and syringoma have been raised. The histology result is in favor of a syringoma. The patient was proposed for medical evacuation to a country with Laser. This case, which is the first in Bangui, should lead clinicians to think of syringoma when faced with a papular genital rash.
Introduction
Syringomas are benign skin tumors of the ecrin or apocrine sweat glands [1]. It is a developmental abnormality of the sweat glands favored by genetics and mycotic infections [2, 3]. It reaches 1% of the population and predominates in phototypes 4 to 6 [4]. Syringoma appears in flare-ups in young subjects, most often of the female sex [5]. There are family forms [6]. The disease presents as firm, smooth papules, pink in color or discreetly yellow or pigmented [5]. It affects more the face around the eyelids (Figure 1), but the rest of the body may be affected [5]. There are several clinical forms including the solitary form, the eruptive form, the plaque form, the miliary form. Solitary genital syringoma is rare and the vulvar rash is exceptional [5, 6, 7, 8, 9]. The aim of this work is to describe the first case of female genital eruptive syringoma observed in Bangui.
Observation
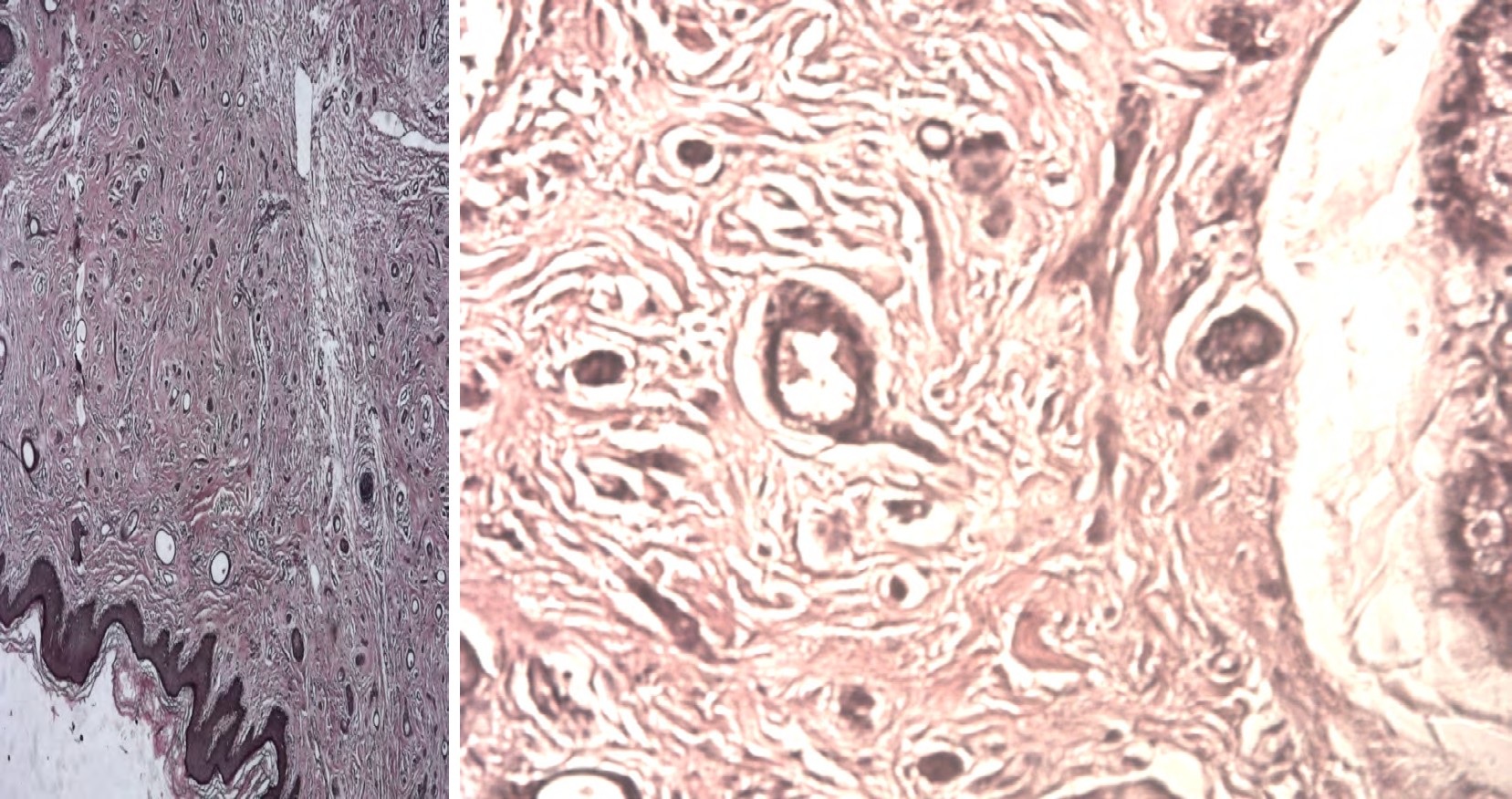
Miss BP, aged 19, living in Bangui, consulted on September 13, 2019 for genital pruritus. There is a history of fatal carcinoma in her older sister constituting psychosis in her mother. Physical examination shows general condition, elastic vulvar edema with a rash of small, smooth papules (Figure 2). Hypotheses of early condyloma and syringoma have been raised. The histology result showed a tumor proliferation located in the dermis. The tumor grows at the expense of dilated or narrow ducts making a comet- like appearance and lined with a double layer of epithelial cells without cytonuclear atypia or mitosis. The stroma is fibrous with vessels and a very discreet infiltrate (Figure 3).
The conclusion is in favor of a syringoma. The patient was proposed for medical evacuation to a country with Laser.
Comment: this case is the first observed in Bangui. The patient is young and female as described in the literature [5, 8, 9]. The disease may be associated with certain pathologies or be an integral part of certain syndromes such as Nicolau Balus syndrome (the other elements of which have not been found), mongolism, Marfan disease and Ehlers-Danlos disease [5, 10]. Etiopathogenically, there was no familial notion of syringoma or mycotic infection [11]; the hormones were not measured in our patient, in particular the progesterone observed by Yorganci, et al [12]. Carcinophobia was observed in her mother as reported by Kopéra, et al [13]. Clinically, the disease was revealed by pruritus as reported by Tay, et al [14] and Kopéra [13]. Treatment of syringoma is discussed on a case-by-case basis with respect to the location and number of lesions between cryotherapy, electrocautery, curettage, endolesional dissection, cryosurgery or laser surgery [1, 15]. Electrocoagulation seems to give better results according to Grosshans [5]. All these more or less aggressive methods can lead to scars and residual pigmentations. Some authors have used drug treatments alone or in combination with Laser such as trichloroacetic acid by Kang, et al [16]. Recently Christine [17] reported a personal experience of successful medical treatment by application of alovera gel combined with biopepin vegetable oil of sea buckthorn for almost a month. The profuse eruption and the vulvar localization of our case led us to consider evacuation to a center with a laser.


Conclusion
This first case described in Bangui should lead clinicians to think about syringoma when faced with a papular genital rash and decision-makers to equip the services with various therapeutic means, in particular the laser.
References
-
Agharbi Falimata Z (2019) Les syringomes. Pan Afr Medic Journal 32: 194.
-
Sand FL, Thomsen SF (2017) Clinician’s update of the benign, premalignant and malignant skin tumours of the vulva : the dermatologist’s view. Int Sch Res Notices 2017: 2414569.
-
Christopher R Shea, Dir M Elston, Eugene J Van Scott (2021) Syringoma Differential Diagnoses. Medscape.
-
Soler Carrillo JJ, Estrach T, Mascaró JM (2001) Eruptive syringoma: 27 new cases and review of the literature. Journal of the European Academy of Dermatology and Venereology 15(3): 242-246.
-
Jean Hilaire Saurat, Edouard Grosshans, Paul Laugier, Jean Marie Lachapelle (2004) Dermatologie et infections sexuellement transmissibles. 4th (Edn.), Masson, Paris, pp: 623.
-
Yesudian P, Thambiah A (1975) Familial syringoma. Dermatologica 150(1): 32-35.
-
Young AW, Herman EW, Tovell HM (1980) Syringoma of the vulva: incidence, diagnosis, and cause of pruritus. Obstetrics and gynecology 55(4): 515-518.
-
Panizzon R, Mitsuhashi Y, Schnyder UW (1987) Syringoma of the vulva. Hautarzt 38(10): 607-609.
-
Blazejak T, Plewig G (1989) Localized syringoma of the vulva. Geburtshilfe Frauenheilkd 49(12): 1083-1084.
-
Dupre A, Bonafe JL (1977) Syringomas, mongolism, Marfan’s disease and Ehlers-Danlos’ disease. Ann Dermatol Venereol 104(3): 224-230.
-
Miranda JJ, Shahabi S, Salih S, Bahtiyar OM (2002) Vulvar syringoma, report of a case and review of the literature. Yale J Biol Med 75(4): 207-210.
-
Yorganci A, Kale A, Dunder I, Ensari A, Sertcelik A (2000) Vulvar syringoma showing Progesterone receptor posi- tivity supports hormonal control of syringomas. Int Journal of Obstétrics and gynecology 107(2): 292-294.
-
Kopera D, Soyer HP, L Cerroni (1999) Vulvar syringoma causing pruritus and carcinophobia: treatment by argon laser. J Cutan Laser Ther 1(3): 181-183.
-
Tay YK, Tham SN, Teo R (1996) Localized vulvar syringomas-an unusual cause of pruritus. Dermatology 192(1): 62-63.
-
Wang JI, Roenigk HH (1999) Treatment of Multiple Facial Syringomas with the Carbon Dioxide (CO2) Laser. Dermatol Surg 25(2): 136-139.
-
Won Hyoung Kang, Nam Soo Kim, Jeune Bae Kim MT, Woo Chul Shim (1998) Un nouveau traitement pour le syringome : Combinaison de laser au dioxyde de carbone et d’acide trichloroacétique. Dermatol Surg 24(12): 1370-1374.
-
Christine (2021) Comment faire disparaitre le syringome des paupières de façon naturelle.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling