A Case of Palmoplantar Pustulosis and its Clinical Course under the Administration of Two Biological Products
A case of pustulosis palmaris et plantaris or palmoplantar pustulosis (PPP) accompanied by generalized skin eruption is presented. Extra-palmoplantar skin lesions similar to those in psoriasis were observed. After the initiation of apremilast administration and phototherapy, most skin lesions were well controlled. After 1 month, chest pain of the sternocostal joint area occurred. Magnetic resonance imaging revealed bone marrow edema in the sternum body and manubrium. This finding was considered pustulotic arthro-osteitis, observed in a patient with PPP. After the administration of secukinumab, the patient’s chest pain diminished. However, after 20 weeks, palmoplantar skin eruption flared up, making walking difficult. Then, secukinumab was switched to guselkumab. The therapy worked gradually; however, after 16 weeks, a sudden aggravation occurred. The patient experienced severe chest pain and nail deformities. Approximately 1 month later, these symptoms improved under the continuous administration of guselkumab. This abrupt exacerbation was considered a paradoxical reaction, affected by guselkumab. After the aggravation subsided, the patient has been kept in a satisfactory condition.
Introduction
Pustulosis palmaris et plantaris or palmoplantar pustulosis (PPP) is a chronic pustular dermatosis, characterized by palmoplantar intraepidermal vesicles filled with neutrophils [1]. Previously, PPP has not been clearly differentiated from palmoplantar pustular psoriasis or a subtype of psoriasis vulgaris (PSO). It is now well recognized that PSO and PPP are separate entities [2].
The most basic diagnostic point of PPP is the small palmar and/or plantar vesicles, usually observed at a very early stage. Then, these vesicles turn to hyperkeratotic pustules and eventually flake off. This cycle continues for a long time, accompanied by arthritis, nail deformities, and sometimes extra palmoplantar skin lesions. Plantar arch involvement is one of the diagnostic points. This report presents a case of PPP presenting with severe chest pain and discusses its clinical course under the administration of two biological products.
A 60-year-old male presented with palmoplantar hyperkeratotic erythema accompanied by generalized skin lesions, with the latter developed several months before.
On the trunk and extremities, partially hyperkeratotic erythematous plaques of various sizes were observed. Some plaques had well-defined annular figures, similar to psoriatic lesions. On the palms and soles, atrophic skin, supposed to be caused by the long-term application of topical steroid, was observed along with partly hyperkeratotic scales. Some flaky vesicles were also observed. The dorsal surface of some fingers was affected and one finger nail was deformed (Figure 1). At this moment, the patient had no obvious joint pain in his hand, foot, or anterior chest.
The patient was diagnosed with PPP at the age of 50 years and had been taking a topical steroid with 5-mg prednisolone for several years.
The patient had hypertension at approximately the same time and started taking the antihypertensive drugs, azilsartan and amlodipine besylate. The patient has no dental problems or otolaryngological diseases, such as chronic tonsillitis or sinusitis. He is a heavy smoker and cannot accept pieces of advice or warnings to quit smoking. He loves outdoor sports.

Pathological Findings
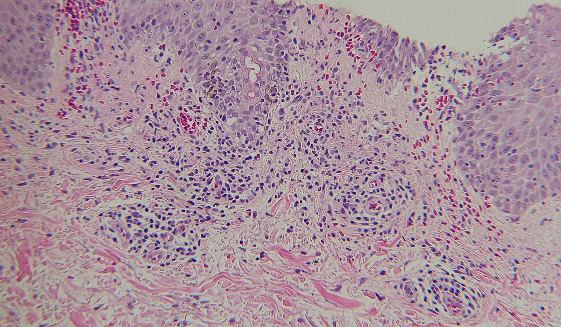
A biopsy specimen was taken from a hyperkeratotic erythematous plaque on his trunk. The epidermis was irregularly elongated and partially spongiotic. In the upper dermis, capillary dilatation and perivascular lymphocyte infiltration were observed. These findings suggest psoriasiform dermatitis with spongiosis (Figure 2).
Treatment and Clinical Course
Prednisolone was stopped, and the oral administration of apremilast along with targeted 308-nm excimer light irradiation was started. Most skin lashes disappeared promptly, leaving scaly erythema on the palms and soles.
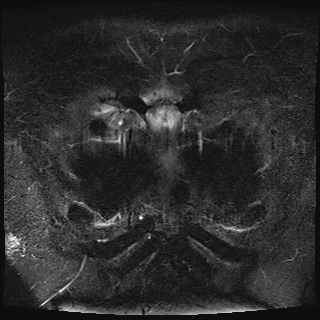
After 1 month, the patient complained of pain in his left clavicular area. The nail deformities also progressed. Magnetic resonance imaging (MRI) revealed bone marrow edema in the sternum body and manubrium, in contiguity with the sternoclavicular joint (Figure 3). No abnormality was observed on the sternoclavicular joint.
<Clinical changes after the initiation of secukinumab> After 4 weeks, chest pain and palmoplantar skin lesions improved; however, the nail deformities remained. After 12 weeks, palmoplantar scaly erythema recurred and gradually intensified.
After 20 weeks, the patient had walking difficulty caused by severe inflammation of the soles; then, treatment was switched to guselkumab, an anti-IL-23 monoclonal antibody. The dose started with 100 mg per week for 4 weeks, followed by the same dose every 8 weeks.
<Clinical changes after the initiation of guselkumab> After 4 weeks, plantar inflammation gradually improved. After 16 weeks, chest pain suddenly increased, and most nails were severely destroyed (Figure 4).
After 20 weeks, chest pain improved. After 28 weeks, the nail deformities were improved. After 60 weeks, mild chest pain rarely occurred and was well controlled with ordinary nonsteroidal anti-inflammatory drugs.

Discussion
In outpatient settings in Japan, PPP is not rare, and the estimated prevalence is 0.12%, which is higher than that in the Western population [3]. Based on the author’s experience, extra palmoplantar skin eruption of PPP is also not rare, and most cases are PSO-like eruption, as observed in this case. Usually, they can be well controlled using ordinary remedies.
MRI suggests synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome [4]. The pathophysiology of PPP and SAPHO syndrome are thought to overlap. The patient in this case report has an obvious clinical feature of PPP so that the patient’s chest pain was categorized to be pustulotic arthro-osteitis, a complication of PPP.
Secukinumab was reported to be effective in treating palmoplantar psoriasis [5], which bears similarities to PPP. In this case, it worked well for approximately 12 weeks; then, the palmoplantar skin eruption severely worsened.
After switching to guselkumab, a sudden exacerbation was noticed, which subsided after 4 weeks under the continuous administration of guselkumab. This abrupt change may fall into the category of paradoxical reaction.
Throughout the clinical course, in this patient, PPP was well controlled using guselkumab, as previously reported [6]. Now, the patient is on the regular administration of guselkumab for more than 2 years and has almost no medical problems related to PPP.
References
-
Uehara M, Ofuji S (1974) The morphogenesis of pustulosis palmaris et plantaris. Arch Dermatol 109(4): 518-520.
-
Murakami M, Ohtake T, Horibe Y, Ishida-Yamamoto A, Morhenn VB, et al. (2010) Acrosyringium is the main site of the vesicle/pustule formation in palmoplantar pustulosis. J Invest Dermatol 130(8): 2010-2016.
-
Kubota K, Kamijima Y, T, Ooba N, Koide D, Iizuka H, Nakagawa H (2015) Epidemiology of psoriasis and palmoplantar pustulosis: a nationwide study using the Japanese national claims database. BMJ Open 5(1): e006450.
-
Khan MM, Khan MA (2009) New insights into synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome. Current Rheumatology Reports 11: 329-333.
-
Gottlieb A, Sullivan J, van Doorn M, Kubanov A, You R, et al. (2017) Secukinumab shows significant efficacy in palmoplantar psoriasis: results from GESTURE, a randomized controlled trial. J Am Acad Dermatol 76(1): 70-80.
-
Terui T, Kobayashi S, Okubo Y, Murakami M, Hirose K, Kubo H (2018) Efficacy and safety of guselkumab, an anti- interleukin 23 monoclonal antibody, for palmoplantar pustulosis. JAMA Dermatol 153(3): 309-316.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling