Reviewing Practical Administration of Oral Propranolol for Infantile Haemangiomas
In the era where every national government promotes the quality of public health through family empowerment and national health insurance along with all its terms and arrangements, doctors as part of the public health service program are expected not mono-dimensional; dealing only the therapeutic elements of the health service, Doctors are expected to comprehend other factors, such as the availability and preparation form of the drug in the hospital formulary, and the efficacy of the patient's health costs. Propranolol is long known to be effective as a therapy for infantile haemangioma, and there are various propranolol therapy regimens for it. In theory, the oral administration of propranolol for infantile haemangioma ideally corresponds to the dose proposed by Léauté-Labréze which is 2 milligrams per kilogram body weight daily, in 6-hour intervals or 4 times of drug administration, and the patients are to have weekly evaluation for dose adjustment and assessment of side effects. In practice, modification to existing regimens to twice daily of 10 milligrams in order to accommodate adaptation to hospital formulary factors and the patient's socio-economic factors are proven to be practical, effective, yet still safe.
Introduction
Infantile haemangioma is a benign tumor lesion arising from the abnormal proliferation of blood vessels that are often found in babies/infants. Usually infantile haemangiomas undergo rapid development until the age of 1 year, remain static until a certain time point, then go through spontaneous regression. Infantile haemangiomas are often located in the area of the face and neck, occur in young women three times more often than boys [1, 2, 3, 4].
Infantile haemangiomas are generally treated conservatively, by careful monitoring of the spontaneous regression. However in some occasion this lesion may require more proactive management, especially with consideration of specific area locations it resides such as at the airway structure, around the periorbital area where it is prone to trauma and rubbing, or in the midline part of face where it may cause aesthetic and psychologic disturbance [4, 5].
One of the first-line therapies for infantile haemangioma is oral prednisolone with doses of 2 to 5 milligrams per kilogram of body weight daily [6]. Conversely, as response to the systemic corticosteroid therapy may vary, its side effects for a long usage is not favorable. Other medications are also reported to be an alternative therapy for infantile haemangioma, such as interferon-α, vincristine, and cyclophosphamide, but all of them are also reported to risk serious side effects [7, 8].
In June 2008, Christine Léauté-Labréze and colleagues from The Children’s Hospital of Bordeaux wrote in his column “Letter to the Editor” of The New England Journal of Medicine regarding their preliminary experience with oral propranolol therapy to manage severe infantile haemangiomas [9]. They reported 11 children with capillary haemangiomas: 10 with lesions on the face and 1 with lesion in the forearm; among whom four children were unresponsive to previous oral prednisolone therapy. The average age of the children receiving the initial therapy of oral propranolol was 3.2 month old, with the age range of 2 month-old to 6 month-old. The first patient received oral propranolol with doses of 3 milligrams per kilogram of body weight daily, while subsequent patients got a dose of 2 milligrams per kilogram of body weight daily. All children in their study showed improvements in terms of reduced size and improved color of the lesions, four of whom were also confirmed by ultrasonogram for having reduced lesion size. The mean period of treatment was 9.8 months. During follow-up observation, 7 out of 10 children already after therapeutic regimens still continues experiencing color and thickness regression of the lesion, while 3 other enduring stable.
The effectiveness of oral propranolol –with its mechanism of action, therapeutic effects or side effects already widely known-- as therapy for infantile haemangiomas gives leeway for the doctors to replace risky drugs such as corticosteroids, interferon-α, cyclophosphamide and vincristine. Although oral corticosteroids remains an option, oral propranolol therapy immediately became a first-line therapy for infantile haemangioma management.
Mechanism of Action Propranolol
Within a few hours after oral propranolol was given, it will trigger vasoconstriction, so redness in lesions gradually fading. The main effect of oral propranolol was preventing the rate of angiogenesis on the haemangioma. Léauté-Labréze and colleagues theorized oral propranolol would lower basic fibroblastic growth factor, (BFGF) and performance factor in growing endothelial blood vessel (vascular endothelial growth factor, VEGF) [9]. Truong and others theorized that β-blocker disturbeb catecholamine receptors, lowers cyclic-AMP and lowering the levels of VEGF. Propranolol also triggers the involution of haemangioma by triggering endothelial apoptosis [9, 10].
Side Effects
There were no reports suggesting serious side effects related to oral propranolol therapy for infantile haemangioma. The side effects ever been reported, among others, are somnolence, bradycardia, hypotension and hypoglycemia [11, 12]. All symptoms returned to normal when the dose was lowered, so it is unnecessary to stop the teraphy should we find the side effects.
Lawley and his friends once reported symptoms of lethargy, bradycardia and hypotension in infants aged 6-weeks with eyelid haemangioma, and hypoglycemia in infants aged 36-days with multiple haemangioma. The second baby was in oral propranolol therapy doses of 2 milligrams per kilogram of body weight daily.
Bonifazi and coauthors reported there was once hypoglycemia and seizure in infants with diffuse haemangiomatosis treated with oral propranolol of 2 milligrams per kilogram of body weight daily for 5 months [13]. Patient was carefully treated and monitored, as soon as there were no symptoms of hypoglycemia patient returned to a lowered dose of oral propranolol with dose of 1.5 milligrams per kilogram of body weight daily. During the next 5 months patient had no complaints.
The Dose and Monitoring Recommendations
Answer Léauté-Labréze and coauthors, Siegfried, Keenan, and Al-Jurcidini made the first formula oral propranolol therapy protocol for infantile haemangioma [13]. Since that time, many of the management guidelines published on the basis of a reference from their writings [5, 9, 10, 13].
Before initiating oral propranolol therapy, doctors are to check the possibility of family history with heart problems. Doctors need to collect data of basic vital signs, frequency of heart rate, blood pressure, and blood chemistry examination. The therapy begins with a dose 0,5 to 1 milligrams per kilogram body weight/day (divided in 3 times a day). If the dose is well tolerated, the dose was increased 2 to 3 milligrams per kilogram body weight daily, and was carried out for 6 to 12 months, each month a dose tailored to weight fluctuation, propranolol should undergo gradual decline (tapering off) with a reduction of 50% of previous dose for 1 to 2 weeks before quitting [14].
Evaluation of cardiovascular condition and blood sugar levels to be evaluated thoroughly after the initial dose, and at any time when there is any dose adjustment. Manunza and his friends monitor the frequency of patient’s heart rate and blood pressure every 30 minutes during the first 4 hours post initial dose, the same thing is performed during every dose adjustment [15]. Maturo and Hartnick also did similar monitoring protocol, such as periodic blood pressure measurements every one hour and heart rate every 4 hours [16].
Cases
Case 1
In April 2021, we had a 4 month-old baby girl with body weight of 6 kilograms, referred from a dermatologist with diagnosis of infantile haemangioma. She had single lesion in the midline of forehead, reddish in color, with a dimension of 3 centimeters x 2 centimeters, arose 1 millimeter above the surrounding skin, soft during palpation, distinct margin and mobile from its base and the surrounding tissue. This patient was referred to our plastic surgery clinic with the intention for excision. Later she was treated with oral propranolol therapy of 10 milligrams given twice daily for 12 months’ time, with further plan of excisional therapy should the lesion not regressing after 12 months.
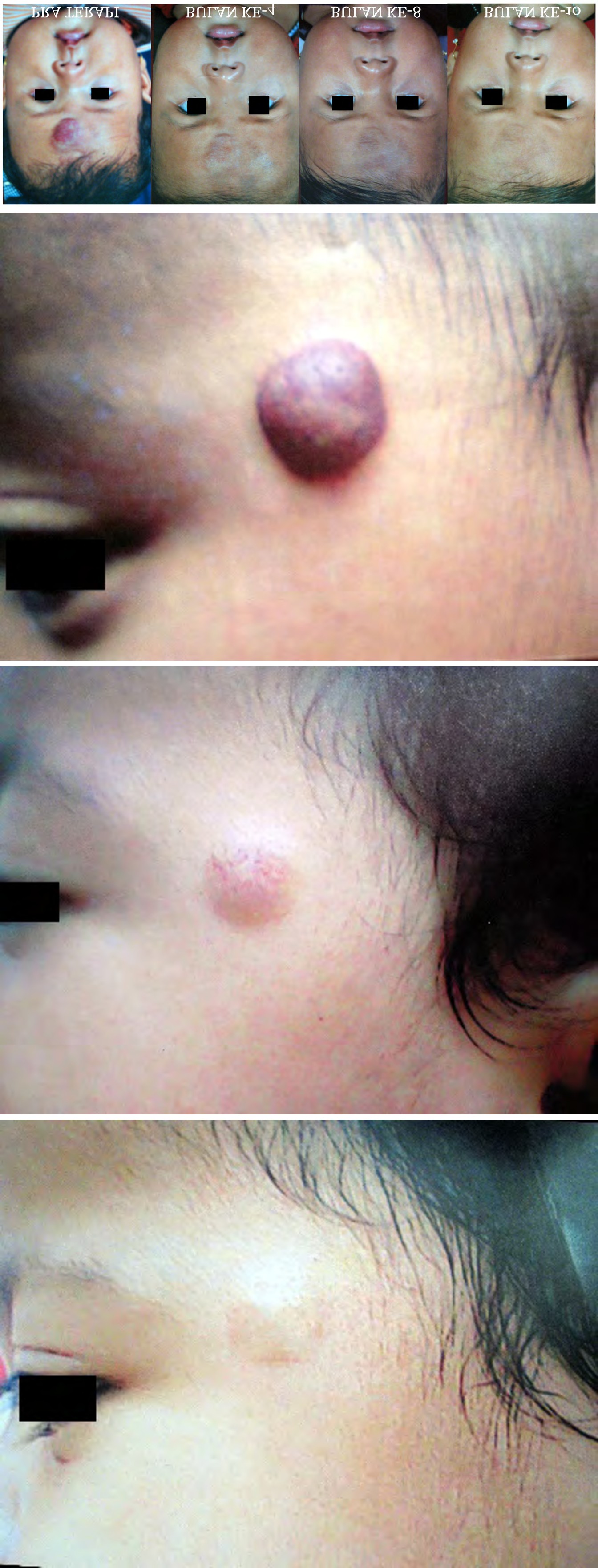
Figure 1 (left to right): Before oral propranolol therapy, on the 4th month after initial therapy, on the 8th month after initial therapy, and on the 10th month after initial therapy.
Each month she visited our plastic surgery clinic for vital sign and pulse rate monitoring, while blood sugar check was conducted every 2 months. In August 2021, the 4th month after initial therapy, the redness was already faded, but darker shade of skin was still visible, and the bulging still remained. In December 2021, the 8th month after initial therapy, haemangioma lesion was already level with the surface, the darker shade if skin increasingly faded. In February 2022, 10 months after initial therapy, regression of the lesions completed, the appearance of the forehead showed no more haemangioma lesion. Her pulse rate and blood sugar level was within normal limit during the therapeutic regimen.
Case 2
In June 2021, we had a 14 month-old female patient with body weight of 10 kilograms, referred from a
dermatologist with diagnosis of infantile haemangioma. She had one infantile haemangioma lesion from her left upper eyelid area expnding to her left frontotemporal area. The lesion was scattered, bright red in color, with a dimension approximately 5 centimeters x 5 centimeters, arose 1 millimeter above the surrounding skin, soft during palpation, distinct margin and mobile from its base and the surrounding tissue. This patient was referred to our plastic surgery clinic with the intention for excision. Later she was treated with oral propranolol therapy of 10 milligrams given twice daily for 12 months’ time, with further plan of excisional therapy should the lesion not regressing after 12 months.
Figure 2 (left to right): Before oral propranolol therapy, on the 4th month after initial therapy, and on the 8th month after initial therapy.
Each month she visited our plastic surgery clinic for vital sign and pulse rate monitoring, while blood sugar check was conducted every 2 months. In October 2021, the 4th month after initial therapy, the entire lesion was already level with the surrounding skin, redness in her left upper eyelid diminished, leaving only a little area of redness on the left frontotemporal area. In February 2022, 8 months in therapy, regression of the lesions completed. Monitoring the pulse count as well as blood sugar while checks for the therapeutic regimen shows values in the normal range.
Case 3
In June 2021, we received a visit from a girl patient aged

6 months and 7 kilograms of weight with skin lesions in temporal forehead, round, reddish lesions color with midline lesions the size of 2 centimeters, 2 millimeters protrudes from the surrounding skin, rubbery in palpation, firm and clearly bordered and not fixed with the base and the surrounding tissue. The patient was diagnosed haemangioma and initially sent to our plastic surgeon for excision with consideration of aesthetically favorable resulting scar. Her parent asked if there was an option for a non-surgical pharmacotherapy, so we programmed her with oral propranolol therapy of 10 milligrams given twice daily for 12 months’ time, with further plan of excisional therapy should the lesion not regressing after 12 months.
Figure 3 (left to right): Before oral propranolol therapy, on the 5th month after initial therapy, and on the 9th month after initial therapy.
Each month the patient visited our clinic to evaluate her lesion as well as her vital signs and pulse count. Her blood sugar was evaluated bimonthly. In November 2021, 5 months in therapy, the entire lesion was already flat to the surface level of the skin, reddish lesions are a lot fading, and the dimension already shrinking to 1 centimeter in width. In March 2022, 9 months in therapy, the lesion regression. Pulse count as well as blood sugar level during the therapeutic duration shows values within the normal range.
Case 4
In July 2021, we received a visit from a girl patient aged 11 months and 9 kilograms weight with reddish skin lesions in the midline of forehead, its colors was bright red, round size diameter 5 millimeters lesion, lesions are more prominent in central part approximately 1 millimeter from the surrounding skin, rubbery in palpation, firm and clearly bordered and not fixed with the base and the surrounding tissue. The patient was diagnosed haemangioma and initially sent to our plastic surgeon for excision with consideration of aesthetically favorable resulting scar. Her parent asked if there was an option for a non-surgical pharmacotherapy, so we programmed her with oral propranolol therapy of 10 milligrams given twice daily for 12 months’ time, with further plan of excisional therapy should the lesion not regressing after 12 months.
Each month the patient visited our clinic to evaluate her lesion as well as her vital signs and pulse count. Her blood sugar was evaluated bimonthly. In November 2021, 4 months in therapy, the entire lesion was already flat to the surface of the skin, redness of the lesions are already shrinking to 3 millimeters x 2 millimeters, and the color a lot more faded. In March 2022, 8 months in therapy, regression of the lesions, the appearance of the forehead already leave no scars. Monitoring the pulse count as well as blood sugar while checks for the therapeutic regimen shows values in the normal range.

Figure 4 (left to right): Before oral propranolol therapy, on the 4th month after initial therapy, and on the 8th month after initial therapy.
Discussion
Although propranolol has been used for decades for management of hypertension, ischemic heart disease, cardiac arrhythmia disease, nerve related diseases, endocrine disorders, eye diseases, its level of safety and effectiveness for the therapy on pediatric patients are not to be agreed yet. The same applies in the use of oral propranolol for infantile haemangioma.
Protocol for oral propranolol therapy for infantile haemangioma may vary. This is common on generic drugs which need tailored adjustment from adult doses to pediatric doses; On the other hand, prospective studies to find proper doses of certain drugs for children very rarely can be conducted. There are many guidelines, but there are similarities between those protocols, for example: gradual adjustment for the sake of patient safety issue.
In the aspects of interval and frequency of daily medication, many variants have been published. Propranolol has optimal interval of 6 hours, but for the sake of practicality may be given in the 8 to12 hour interval [17, 18, 19].
One reference recommended that in the first week of propranolol therapy is given with doses of 0.5 to 1 milligram per kilogram of body weight daily divided into 2 doses, then in the second week if first week’s dose can be tolerated without any problems patients the dose is raised 1 to 1.5 milligrams per kilogram of body weight daily divided into 2 doses, and the third week if the second week’s dose tolerable raised 2 to 3 milligrams per kilogram of body weight daily (like the first dose introduced by Léauté-Labréze) and the dose is maintained until the lesion regressing. In many references, oral propranolol therapy for infantile hemanigioma adopt the formula coined by Léauté-Labréze i.e., 2 milligrams per kilogram of body weight daily, where it is commonly divided into 2 to 3 times. The maximum dose of propranolol for infantile haemangioma has not yet been clearly established, however there is research stating a maximum dose of propranolol for arrhythmia therapy for pediatric patients of 5 milligrams per kilogram of body weight daily. After the regression of the lesions, there is a therapeutic regimen that recommends gradual dose reduction (tapering off) and some others are simply stopping the therapy without gradual adjustment.
Outside the medical aspect of the discussion, in an era where the Government encourages the quality of public health through the empowerment of families and the provision of national health coverage along with all of the terms and tatanannya, the doctor of Ministry program as part of public health is no longer sufficient to manage in mono- dimensional only consider the medical element only. Doctors must also be able to holistically consider other factors, such as the availability of drugs in formularium hospital, the patient’s health, cost efficiency and others.
Preparations of the drug propranolol in hospital formularies was accordingly governed by national formularies. In our country Indonesia it is regulated in Health Minister document (KEPMENKES no 89/MENKES/ SK/II/2013), namely in the form of 10-milligrams and 40-milligrams tablets, and those preparation provide difficult and impractical for patients or parents to apply into their therapeutic regimens because of the potential inaccuracy of the divided dose. Therefore, we suggest a simpler regimen of therapy with a tablet of 10 milligrams propranolol --we teach the parents to dissolve it into milk, sweetened tea or water syrup; given twice a day immediately after lunch and dinner to avoid hypoglycemic effects.
Patients undergoing therapy with regimens are getting prescription drugs to every 30 days, all of the patients is a participant of Indonesian national health coverage (JKN) so that the entire drug free insured JKN. Into consideration the option cycle is 30 days for the sake of the efficiency of travel financing introduction when patients and controls to plastic surgery clinic of the hospital. This is certainly going to be troublesome if the therapy regimens are in a form that every week should be adapted. Every 30 days the patient control for evaluation of vital signs and pulse count, blood sugar checks during every 2 months.
Reviewing a dose of propranolol on the patients case 1, if appropriate therapy regimens used in the first week then consensus patients should have got 3 to 6 milligrams per day (2 x 1.5 milligrams to 2 milligrams 3 x) then in the second week of 6 to 9 milligrams per day (2 x 3 milligrams to 2 x 4.5 milligrams) then the third week and so on 12 to 18 milligrams per day (2 x 6 milligrams to 2 x 9 milligrams). A dose of 2 x 10 milligrams for patients accepted therapeutic regimens are a matter of theory is indeed much bigger even above value dosage of maintenance, but during that time also no complaints, symptoms, or signs that indicate the presence of adverse effects.
Reviewing a dose of propranolol on the patients case 2, if appropriate therapeutic regimens used in the first week then consensus patients should get 5 to 10 milligrams a day (2 x 2.5 milligrams to 2 x 5 milligrams) and then on the second week of 10 to 15 milligrams per day (2 x 5 milligrams to 2 x 7.5 milligrams) then the third week and so on 20 to 30 milligrams per day (2 x 10 milligrams to 2 x 15 milligrams). A dose of 2 x 10 milligrams for patients accepted therapeutic regimens are a matter of theory is indeed much greater during the first 2 weeks of treatment was even almost equals the value of the over-dosage of maintenance dose, but during that time also no complaints, symptoms, or signs that indicate the presence of adverse effects.
Reviewing a dose of propranolol on the patients case 3, if the therapeutic regimens used appropriate consensus then on first week patients should have got 3.5 to 7 milligrams per day (2 x 1.75 milligrams to 2 x 3.5 milligrams) and then on the second week 7 to 10.5 milligrams per day (2 x 3.5 milligrams to 2 x 5.25 milligrams) then the third week and so on 14 to 21 milligrams per day (2 x 7 milligrams to 2 milligrams x 10.5). A dose of 2 to 10 milligrams for patients accepted therapeutic regimens are a matter of theory is indeed much greater during the first 2 weeks of treatment, but also during that time no complaints, symptoms, or signs that indicate the presence of adverse effects.
Reviewing a dose of propranolol on the patients case 4 therapeutic regimens are used, if the appropriate consensus then on first week patients should get 4.5 to 9 milligrams per day (2 x 2.25 milligrams or 2 x 4.5 milligrams) and then on the second week 9 to 13.5 milligrams per day (2 x 4.5 milligrams or 2 x 6.75 milligrams) then the third week and so on 18 to 27 milligrams per day (2 x 9 milligrams or 2 x 13.5 milligrams). A dose of 2 x 10 milligrams for patients accepted therapeutic regimens are a matter of theory is indeed much greater during the first 2 weeks of treatment was even slightly bigger than the value of lower doses of maintenance dose, but during that time also no complaints, symptoms, or signs that indicate the presence of adverse effects.
Conclusion
In theory, the giving of oral propranolol for infantile haemangioma ideally correspond to doses expressed by Léauté-Labréze i.e., 2 milligrams per kilogram body weight/ day [9], is divided in intervals of 4 hours or 4 times the giving of drugs, and every week the control patients to see a doctor for evaluation and dose adjustment of side effects. In the four cases presented in this case report, the selection of material of a given drug formularies hospital as well as socio- economic factors of the patient makes doctor doing a simple modification of 10 milligrams propranolol given twice daily, which applied into therapeutic regimens are practical, effective, but still safe.
Report this case obviously have limitations in the amount of data. Authors are aware of the need to research a prospective with the number of much more data to monitor the effectiveness and safety of propranolol appropriate regimen at the giving of the long term. However, we hope this case report results can be adequate reference and give more insights to colleagues who involve in infantile haemangioma management at the level of primary health care services.
References
-
Kilcline C, Frieden IJ (2008) Infantile haemangiomas: how common are they? A systematic review of the medical literature. Pediatr Dermatol 25(2): 168-173.
-
Boye E, Jinnin M, Olsen BR (2009) Infantile haemangioma: challenges, new insights, and therapeutic promise. J Craniofac Surg 20: 678-684.
-
Haggstrom, Drolet BA, Baselga E, Chamlin SL, Garzon MC, et al. (2006) Prospective study of infantile haemangiomas: clinical characteristics predicting complications and treatment. Pediatrics 118(3): 882- 887.
-
Galiano RD, Gurtner GC (2007) Vascular anomalies. In: Kryger ZB, Sisco M (Eds.), Practical plastic surgery. 1st (Edn.), Austin: Landes Bioscience, pp: 138-141.
-
Lawley LP, Siegfried E, Todd Jl (2009) Propranolol treatment for haemangioma of infancy: risks and recommendations. Pediatr Dermatol 26(5): 610-614.
-
Pope E, Krafchik BR, Macarthur C, Stempak D, Stephens D, et al. (2007) Oral versus high-dose pulsecorticosteroids for infantile haemangiomas problematic: a randomized, controlled trial. Pediatrics 119(6): e1239-47.
-
Bruckner AL, Frieden IJ (2003) Haemangiomas in infancy. J Am Acad Dermatol 48(4): 477-493.
-
Michaud AP, Bauman NM, Burke DK, Manaligod JM, Smith RJ (2004) Spastic diplegia and other motor disturbances in infants receiving interferon-alpha. Laryngoscope 114(7): 1231-1236.
-
Léauté-Labréze C, Dumas de la Roque E, Hubiche T, Boralevi F, Thambo JB, et al. (2008) Propranolol for severe haemangiomas in infancy. N Engl J Med 358(24): 2649-2651.
-
Truong MT, Chang KW, Berk DR, Heerema-McKenney A, Bruckner AL (2010) Propranolol for the treatment of a life-threatening mediastinal infantile haemangioma and subglottic. J Pediatr 156: 335-338.
-
Hoffmann BB (2007) Adrenoreceptor antagonist drugs. In: Katzung BG (Ed.), Basic and clinical general. 10th (Edn.), New York: McGraw-Hill, pp: 147-158.
-
Zimmermann AP, Wiegand’s, Werner JA, Eivazi B (2010) Propranolol therapy for infantile haemangiomas: review of the literature. Int J Pediatr Otorhinolargyngol 74(4): 338-342.
-
Bonifazi E, Acquafredda A, Milano A, Montagna O, Laforgia N (2010) Severe hypoglycemia during successful treatment of diffuse haemangiomatosis with propranolol. Pediatr Dermatol 27(2): 195-196.
-
Siegfried EC, Keenan WJ, Al--Jureidini S (2008) More on propranolol for haemangiomas of infants [letter]. N Engl J Med 359: 2846.
-
Manunza F, Syed S, Laguda B, Linward J, Kennedy H, et al. (2010) Propranolol for infantile haemangiomas complicated: a case series of 30 infants [letter]. BR J Dermatol 162(2): 466-468.
-
Maturo S, Harnick C (2010) Initial experience using propranolol as the sole treatment for infantile haemangiomas airway. Int J Pediatr Otorhinolargyngol 74(3): 323-325.
-
(2010) Propranolol. Drug Facts and Comparisons 4.0. Efacts [online]. Wolters Kluwer Health, Inc.
-
(2008) Propranolol hydrochloride oral solution prescribing information. Roxane Laboratories, Inc.
-
(2009) Lexi-Comp ONLINE. Propranolol Hydrochloride. Hudson, OH: Lexi-Comp; c1978.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling