Giant Rhinophyma: About a New Case
The Rhinophyma is a benign skin condition which mostly affects Caucasian men between the ages of five and seven. It is characterized by progressively enlarging nasal skin, irregular thickening, and nodular deformation. This is the final stage of chronic acne rosacea. The main reasons patients seek medical attention are cosmetic and functional impairments, like nasal obstruction. In Rhinophyma, surgical removal of the hyperplastic tumor mass is recommended. We describe here the case of a giant Rhinophyma with respiratory and olfactory difficulties for 5 years.
Introduction
Giant Rhinophyma is a benign, progressive skin disorder characterized by a large, bulbous, and erythematous nose [1]. It is considered the final stage of acne rosacea. Several synonyms exist for this condition, from potato nose to rum blossom to pachydermatosis to pseudo-ephantiasis [2]. In rare cases, these lesions can be gigantic in size and difficult to treat [3]. Here we describe a case of giant Rhinophyma with respiratory and olfactory difficulties.
Case Report
This is a 75-year-old male with no significant pathologic history who consulted for a hypertrophic nose that had been developing for 5 years and gradually enlarged and underwent topical treatment with no improvement. Examination revealed a bulbous mass covering the entire nose, with dilated sebum-filled pores, deep nasal furrows surmounted by melica crusts (Figure 1).

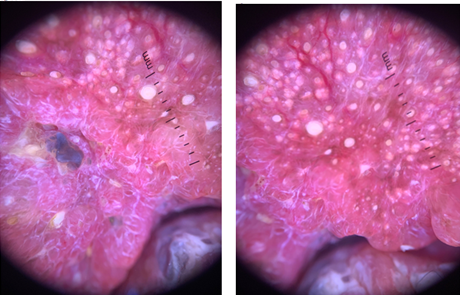
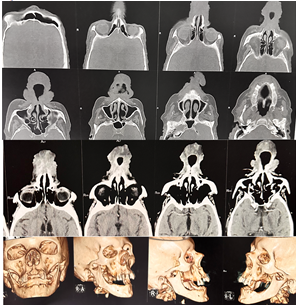
Nasal palpation was normal and showed no suspicious infiltration. Dermatoscopy revealed dilated and sebum-filled follicular openings, keratinized cones on an erythematous background, yellowish crusts, and scattered polygonal and branching vessels (Figure 2). The patient received local antibiotic therapy with local healing, eliminating signs of local superinfection (Figure 3). Preoperatively, a craniofacial CT scan was prescribed, which showed hypertrophy of the nasal mucosa and soft tissues with budding and hyper vascularization, occlusion of the nostrils, without concomitant bone involvement (Figure 4). The patient underwent plastic maxillofacial surgery for constructive surgery and subsequent treatment.

Discussion
Rhinophyma is a disfiguring disease of the nose and is considered the most severe form of end-stage rosacea, characterized by a gradual and painless overgrowth of the sebaceous glands and connective tissue in the nose [4]. Various theories have been proposed to explain this condition, such as: There is empirical evidence of exacerbation from alcohol or caffeine consumption and the presence of the mite Demodex folliculorum. It is a disfiguring and troublesome condition due to the unsightly appearance and nasal congestion. It is characterized by a painless, bulbous growth at the tip of the nose. Affects the skin and subcutaneous tissues of the nasal tip, sparing the underlying cartilage [4, 5, 6]. The diagnosis is clinical, in case of doubt histological [7]. Several surgical procedures have been used at this stage, including skin shaving or skin incision with re- epithelialization, full skin excision with flap or free skin graft, partial skin ablation, cryosurgery, electrocoagulation, and laser [8]. Carbon dioxide and Nd: YAG lasers have also proven their worth [9]. Postoperative skin color results are likely to be better if the wound is secondarily healed. Recent reports highlight the effect of combination therapy on minimizing the risk of side effects [1, 7].
Conclusion
Given the massive deformity of the nose that is responsible for nasal obstruction, patients with Rhinophyma suffer from serious psychosocial problems, often for years, which prompt them to seek effective help. Medical treatment was unsatisfactory. Interventional surgical measures remain the best pillar, convincing both the patient and the surgeon.
References
-
Marijic B, Braut T, Tudor F, Filipovic N, Hadzisejdic I, et al. (2021) Giant rhinophyma with olfactory and breathing dysfunction successfully treated by shave excision and electrocautery. Dermatol Ther 34(5): e15029.
-
Mangal M, Agarwal A, Jain H, Gupta A (2012) Giant Rhinophyma of the nose. J Oral Maxillofac Surg 70(2): 376-377.
-
Rordam OM, Guldbakke K (2011) Rhinophyma: Big problem, simple solution. Acta Derm Venereol 91(2): 188-189.
-
Chowdhary S, Alexander A (2021) Giant rhinophyma. BMJ Case Rep 14(1): e239860.
-
Dick MK, Patel BC (2020) Rhinophyma. In: StatPearls. Treasure Island (FL): StatPearls Publishing.
-
Laun J, Gopman J, Elston JB (2015) Rhinophyma. Eplasty 15: ic25.
-
Chauhan R, Loewenstein SN, Hassanein AH (2020) Rhinophyma: prevalence, severity, impact and management. Clin Cosmet Investig Dermatol 13: 537- 551.
-
Claros P, Sarr MC, Nyada FB (2018) Rhinophyma: our experience based on a series of 12 cases. Eur Ann Otorhinolaryngol Head Neck Dis 135: 17-20.
-
Borzecki A, Turska M, Strus RB, Wojtaluk AS (2019) Use of laser therapy in the treatment of severe rhinophyma: a report of two cases. J Cosmet Laser Ther 21(7-8): 390- 394.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling