Consider Zinc Deficiency in Infants with Periorificial Lesions
Background: Zinc is an essential trace element required for proper bodily function. Its deficiency can lead to various manifestations, including dermatological issues. There are two forms of zinc deficiency: hereditary and acquired. Case Report: We present two cases. The first case involved a child with a family history of two brothers who passed away at the age of 1 year, exhibiting a similar symptomatology. The second case involved a patient with hereditary epidermolysis bullosa and malnutrition. Both cases presented with erosive erythematous lesions around the mouth and extremities, which were unresponsive to symptomatic treatments. Additionally, they experienced diarrhea. A definitive diagnosis was made by measuring the levels of zinc in their blood, which were found to be low. Treatment with oral zinc sulfate was prescribed. The first patient showed rapid improvement with the treatment, but experienced recurrence when it was discontinued and subsequently improved again upon reinstatement. Unfortunately, the second infant passed away due to complications from an infection.
Introduction
Zinc is an essential trace element that plays a crucial role in the proper functioning of cells, as well as in the metabolism of proteins, carbohydrates, and vitamin A [1]. Deficiency of zinc can lead to a range of clinical manifestations, including gastrointestinal, cutaneous, and neurological symptoms [2]. There are two types of zinc deficiency: hereditary and acquired, with the latter being more common [3]. In this report, we present two new cases of zinc deficiency, one hereditary and the other acquired.
Observations
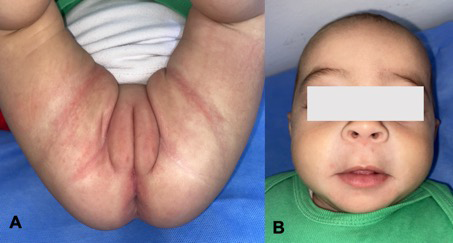
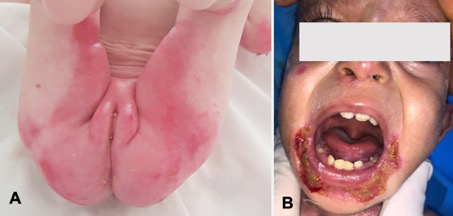
The first case involves a 5-month-old infant from a consanguineous marriage. The patient had a family history of two brothers who passed away at the age of one year with similar symptoms, and a low level of zinc in their blood tests. Since the age of 3 months, the infant developed erosive erythematous patches on the genital-crural, perioral, and occipital areas (Figures 1A and 1B), which did not respond to topical treatment with healing creams and antifungal medications. The patient also had chronic diarrhea. Acrodermatitis enteropathica was suspected based on consanguinity, family history, and skin manifestations. The diagnosis was confirmed by measuring the zinc level, which was found to be low at 0.47mg/ml, along with low alkaline phosphatase levels. Oral zinc sulfate supplementation was initiated at a dose of 3mg/kg/day, resulting in rapid improvement. However, there was a recurrence of symptoms when the parents discontinued the treatment. The supplementation was immediately reinstated, leading to significant improvement (Figures 2A and 2B). Genetic testing could not be performed due to financial limitations. The infant is currently receiving zinc therapy and undergoing regular check-ups. The second case involves a one-year-old infant from a consanguineous marriage, who was being followed for hereditary epidermolysis bullosa. The patient had been hospitalized multiple times in the pediatric emergency department due to malnutrition, dehydration, and delayed developmental milestones of unknown etiology. Since the age of 4 months, the infant presented with erosive crusty plaques with involvement of the extremities and alopecia (Figures 3A and 3B). A low level of zinc (0.4mg/ml) was detected, confirming the diagnosis of pseudoacrodermatitis enteropathica. Oral zinc supplementation was prescribed, but the treatment was not administered due to financial limitations. Unfortunately, the infant died due to infectious complications.

Discussion
The diagnosis of zinc deficiency should be considered when a triad of periorificial dermatitis, alopecia, and diarrhea is present [1, 2, 4]. The clinical manifestations are similar for both acquired and genetic zinc deficiencies [1]. These may include symmetrical erythematosquamous lesions, sometimes presenting as eczematous, psoriasiform, vesiculobullous, or erosive periorificial and acral lesions. Bacterial or candidal superinfections are common, which can sometimes lead to misdiagnosis [1, 4, 5, 6]. Other symptoms that may be observed include alopecia or thinning hair, diarrhea with anorexia, irritability, and delayed growth and development [2, 4, 5, 6]. However, this complete clinical presentation is only seen in about 20% of cases [6]. The hereditary form of zinc deficiency is known as acrodermatitis enteropathica, a rare genetic disease inherited in an autosomal recessive manner. It typically manifests in the first months of life and is caused by mutations in the SLC39A4 gene located on chromosome 8q24.3. This gene codes for a transmembrane protein called Zip4, which is required for zinc absorption. Its deficiency leads to impaired enteral zinc absorption, primarily in the duodenum and jejunum [1, 4, 5, 6].
Multiple acquired causes can contribute to zinc deficiency, leading to a profile resembling pseudoacrodermatitis enteropathica. These causes include excessive losses due to inflammatory gastrointestinal diseases, cystic fibrosis, severe infections, nephrotic syndrome, as well as inadequate intake resulting from exclusive breastfeeding, an imbalanced diet, or prematurity [5, 7].
The diagnosis is primarily based on clinical presentation, patient and family history, and confirmed by low zinc levels in the blood (zincemia) or by diagnostic tests showing the disappearance of clinical signs after zinc supplementation and their reappearance upon discontinuation. It is important to note that normal serum zinc levels can still be observed in around 30% of patients, so normal zinc levels do not rule out the possibility of zinc deficiency. Alkaline phosphatase levels can be useful, as they are often low due to the zinc-dependent nature of the enzyme, indicating the onset of deficiency and the need for zinc supplementation. Genetic studies can also aid in diagnosis when acrodermatitis enteropathica is suspected, although they are often not performed due to cost constraints [8].
Differential diagnoses for acrodermatitis enteropathica include seborrheic dermatitis, atopic dermatitis, contact dermatitis, psoriasis, and Langerhans cell histiocytosis. Other deficiencies, such as essential fatty acids, vitamin B12, or biotin deficiencies, can also present with similar clinical features [1, 5].
The treatment for acrodermatitis enteropathica involves lifelong supplementation with elemental zinc. Zinc sulfate is commonly used at a dose of 3 mg/kg/day and is well- tolerated [3, 8]. Dosages are typically adjusted based on the patient’s age, weight, and symptoms. The response to treatment is usually rapid, with clinical symptoms resolving within a few days [1, 5]. Regular monitoring of serum zinc levels is recommended, and genetic counseling should be offered [3]. With appropriate treatment, the prognosis for acrodermatitis enteropathica is excellent, with a survival rate of 100% [1]. In the case of pseudoacrodermatitis enteropathica, in addition to treating the underlying cause if possible, supplementation with elemental zinc at a dose of 0.5 to 1 mg/kg/day is necessary [3].
Conclusion
The presence of periorificial and extremity lesions should raise the suspicion of zinc deficiency in infants, especially in high-risk populations. Treatment is straightforward and involves the supplementation of elemental zinc. Without treatment, the hereditary form of zinc deficiency can be fatal, whereas the prognosis of the acquired form depends on the underlying cause.
References
-
Nistor N, Ciontu L, Frasinariu OE, Lupu VV, Ignat A, et al. (2016) Acrodermatitis Enteropathica: A Case Report. Medicine 95(20): e3553.
-
Glutsch V, Hamm H, Goebeler M (2019) Zinc and skin: an update. J Dtsch Dermatol Ges 17(6): 589-596.
-
Leung AKC, Barankin B (2016) Case in point: acrodermatitis enteropathica: an infant with skin lesions and diarrhea from zinc deficiency. Consultant for Pediatricians 15(8): 406-408.
-
Chue CD, Rajpar SF, Bhat J (2008) An acrodermatitis enteropathica-like eruption secondary to acquired zinc deficiency in an exclusively breast-fed premature infant. Int J Dermatol 47(4): 372-373.
-
Ouadi Z, Hocar O, Akhdari N, Amal S (2017) La carence en zinc chez l’enfant : du diagnostic au traitement. Journal de pédiatrie et de puériculture 30(3): 118-121.
-
Kharfi M, Zaraa I, Kury S, Moisan JP, Kamoun MR (2005) Acrodermatite entéropathique chez un nourrisson né à terme . Ann Dermatol Venereol 132(3): 246-248.
-
Zeriouh L, Hali F, Khadir K, Benchikhi H (2013) Pseudo- acrodermatite entéropathique chez un nourrisson né à terme, exclusivement nourri au sein. Archives de Pédiatrie 20(10): 1129-1132.
-
Ciampo IRLD, Sawamura R, Ciampo LAD, Fernandes MIM (2018) Acrodermatitis Enteropathica: Clinical Manifestations and Pediatric Diagnosis. Rev Paul Pediatr 36(2): 238-241.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling