A Prospective Prescription Audit of Topical Corticosteroid usage at Skin OPD in a Tertiary Care Centre
Introduction: Topical corticosteroids are used for various conditions in dermatology like vitiligo, eczema and psoriasis. They should be used rationally to minimize the side effects. The present study is done to document and improve the pattern of prescribing topical steroids among patients attending Skin OPD at tertiary care centre. Material & Methods: The study was a prospective audit of 100 prescriptions issued to the patients in skin OPD. The data was collected for age and sex of patients, dermatosis for which it is prescribed, number and molecule of drugs, with its dose, site, duration, strength, quantity and frequency of administration. Descriptive statistics was used for analysis. Results: Present study is an audit of 100 prescriptions. Sixty two patients were males and 49% were in 13-40 years of age group. Most common skin condition for which topical steroid prescribed was eczema in 34%. Average 3-6 drugs were prescribed in majority (82%) of prescriptions. The potent corticosteroids was the most frequently prescribed group in 46% prescriptions and most common molecule prescribed was betamethasone valerate in 27%. In 73% prescriptions twice daily application was advised. Maximum 50% prescriptions of TCS were for 7-15 days and site of application was mentioned in 70%. Generic and brand names were mentioned in all prescriptions with quantity of drug. Fingertip unit application was mentioned in 3% of prescriptions. Conclusion: The most common indication for prescribing topical steroids was eczema and the most common molecule prescribed was betamethasone valerate. Generic and brand names for drugs were used in all prescription, but advice about Finger tip method application was not a routine practice.
Introduction
Corticosteroid (CS) therapy comprises the mainstay of treatment for many dermatologic conditions since they were first introduced in early 1950s [1]. The various indications for which topical corticosteroids (TCS) are used include psoriasis, vitiligo, eczema, atopic dermatitis, acute radiation dermatitis and lichen sclerosus. Steroids, though are highly effective drugs, may produce deleterious effects when used irrationally [2].
Intermittent monitoring of drug use is one of the measures undertaken in order to analyze the rationality of drug usage and to offer feedback/ suggestions to the prescribers [3]. The rational use of topical steroids should include careful consideration of the patient’s age, total area of application, quantity to be applied, efficacy of the selected corticosteroid, and frequency of application [4]. It is to minimize adverse cutaneous and systemic reactions, especially with prolonged use. The purpose of this study was to document and improve the pattern of prescribing TCS among patients attending Skin OPD at a tertiary care center, thus effective modifications can be suggested if necessary.
Material & Methods
This prospective prescription audit was carried out in Skin OPD of tertiary care center for a duration of two months. A total 100 prescriptions issued to the patients were studied. The data collected included age and sex of patients, dermatosis for which TCS was prescribed, number, molecule and potency of the corticosteroid prescribed. The documentation regarding the mention of the dose, site, duration, strength, quantity to be applied, and frequency of administration of TCS was done. Descriptive statistics was used for analysis.
Results
The present study audited 100 prescriptions with majority of patients in age group 13-40 years (49%) and from urban population (69%) (Table 1).
| Frequency (%) | ||
|---|---|---|
| Age group | 1-12 years | 7 |
| 13-40 years | 49 | |
| 41-60 years | 28 | |
| >60 years | 16 | |
| Sex | Male | 62 |
| Female | 38 | |
| Address | Urban | 69 |
| Rural | 31 |
Table 3: Demographic data.
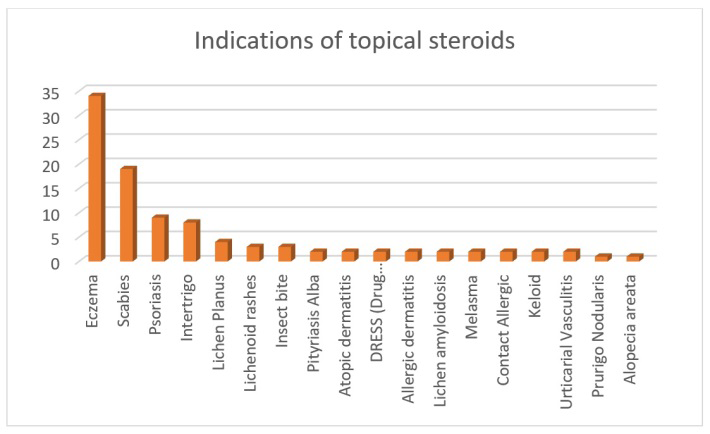
The most common skin condition for which TCS prescribed was eczema (34%) followed by scabies (19%) (Figure 1).
In a prescription, average 3-6 drugs were prescribed to majority of patients (82%) (Table 2).
| Frequency (%) | |
|---|---|
| <3 | 4 |
| 6-Mar | 82 |
| >6 | 14 |
| Total | 100 |
Table 1: Total number of drugs prescribed to a patient.
Of all the systemic agents prescribed, antihistaminic agents (94%) were the most commonly prescribed drugs while among topical agents, topical steroid was prescribed in all 100% cases followed by scabicides (19%) (Table 3).
| Drug Group | Frequency (%) | ||
|---|---|---|---|
| Systemic Drugs | Antihistaminic | 94 | |
| Systemic Drugs | Vitamins | 15 | |
| Systemic Drugs | Scabicide | 12 | |
| Systemic Drugs | Antifungals | 7 | |
| Systemic Drugs | Antibacterial | 5 | |
| Systemic Drugs | Others | 3 | |
| Systemic Drugs | Topical Drugs | Antivirals | 0 |
| Steroids | Topical Drugs | 100 | |
| Topical Drugs | Scabicide | 19 | |
| Topical Drugs | Antibacterial | 22 | |
| Topical Drugs | Antifungals | 14 | |
| Topical Drugs | Analgesic | 0 | |
| Topical Drugs | Others | 5 |
Table 2: Systemic Drugs.
Both brand and generic name were mentioned in all 100 prescriptions. The potent corticosteroids was most frequently prescribed in 46% prescriptions. Mid potent and mild potent corticosteroids were prescribed in 19% and 26% prescriptions respectively while super potent agents in only 4%. The most common molecule of topical steroid prescribed was betamethasone valerate in 27% prescriptions, followed by betamethasone diproprionate and hydrocortisone butyrate in 19% prescriptions (Table 4).
| Molecule of the drug | Frequency (%) | |
|---|---|---|
| Super potent | Clobetasol proprionate (0.05%) | 4 |
| Potent | Betamethasone valerate (0.1%) | 27 |
| Betamethasone diproprionate (0.05%) | 19 | |
| Mid Potent | Mometasone furoate (0.1%) | 14 |
| Beclomethasone (0.025%) | 5 | |
| Mild Potent | Clobetasone proprionate (0.025%) | 6 |
| Fluticasone propionate (0.05%) | 1 | |
| Hydrocortisone butyrate (0.1%) | 19 | |
| Low Potent | Hydrocortisone (1%) | 2 |
| Desonide (0.05%) | 3 |
Table 4: Molecule of the drug.
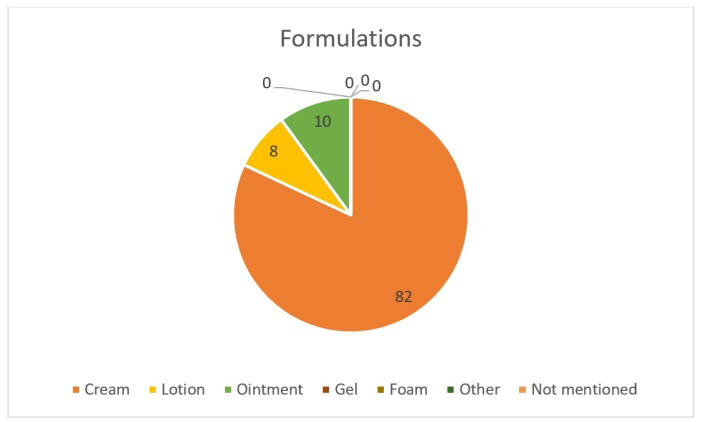
Out of all 100 prescriptions 73% were advised to apply topical corticosteroids twice a day, 25% for once a day and 2% for once a week. Most common formulation of topical steroids prescribed was creams in 82% (Figure 2).
Maximum 50% prescriptions for TCS were for 7-15 days followed by 24% for 16 days- 1 month duration (Table 5).
| Frequency (%) | |
|---|---|
| <7 days | 14 |
| 7-15 days | 50 |
| 16 days-1month | 24 |
| >1 month | 12 |
Table 5: Duration of application of topical steroids.
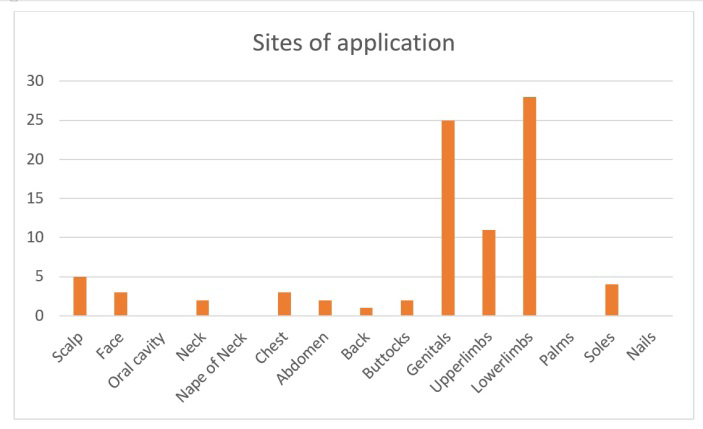
The site of application was mentioned in 70% prescriptions among which lower limbs (28%) were the most common site followed by genitals (25%) and upper limbs (11%) (Figure 3). Quantity of drug was mentioned in all prescriptions (100%).
Fingertip unit was explained and documented in only 3 prescriptions (3%). Fixed drug combination was prescribed in 3% among all. Emollients were prescribed in 78% with explanation about the method of application.
Discussion
The term ‘Audit’ means a methodical examination or review of a condition or situation with the intent of verification. It is an exercise which tries to find out input versus output based on available resources. Periodic or regular ‘prescription auditing’ may minimize overuse and misuse of drugs, plan essential drug selection and estimate the drug need for the community. It also will have a great value to health administrators, policy makers, manufacturers, distributors, health professionals and various consumer groups for decision making.
Since corticosteroids are one of the commonest group of drugs used in dermatological practice, an assessment of their usage pattern is recommended. It will encourage the proper and rational utilization to optimize their benefits and limit adverse effects like skin atrophy, contact dermatitis, tachyphylaxis, striae, telangiectasia and acneiform dermatitis. Systemic reactions may occur in the form of hypothalamic pituitary-adrenal suppression, Cushing’s disease, and femoral head osteonecrosis, when topical steroids are used over large surface area for long period of time [5]. The abuse of corticosteroids is worsened when it is used by general practitioners for any type of skin rashes without a confirm diagnosis and for protracted periods [6]. Potency of TCS used for various indications in dermatology should be individualized based on the severity of the dermatitis, location and surface area of the affected skin, and the age of the patient. Analysis of the prescriptions in present audit revealed that eczema was the most common diagnosis, explaining the greater use of TCS, as they are the first line of anti-inflammatory treatment for eczema and other inflammatory conditions [7].
It has been recommended that the limit of number of drugs per prescription should be two otherwise there will be increased risk of drug interactions. But in the current study, the average number of drugs per prescription was found to be 3-6 in 82% prescriptions. This number is higher than that recommended by Narwane, et al. [8] and Singh, et al. [9] but somewhat similar with studies conducted in western Nepal and different parts of India [10, 11, 12, 13].
In contrast to some other studies on corticosteroid prescriptions where medications were prescribed only by their brand names and generic names were never preferred in Oshikoya [14], our study mentioned both generic and brand names in all our prescriptions. In Jaiswal MK, et al. [15] and Singh, et al. studies [9], TCS were prescribed using their generic names in 88.98% and 85.8% prescriptions respectively. In Sharma, et al. [16] study generic names were mentioned in only 63% prescriptions. Use of generic names usually provides flexibility to the dispensing pharmacist and they are less expensive and increases the prescription compliance than brand-name drugs. Using brand names for prescribing may sometimes create dispensing errors. Drugs with similar brand names but different ingredients might mistakenly be switched over [13]. Use of the drugs mostly by generic name is a welcome initiative towards the rationality, which was reflected in our study.
The potent corticosteroids was the most frequently prescribed in 46% prescriptions, followed by mild and mid potent steroids in 26% and 19% respectively. The most common molecule prescribed was betamethasone valerate in 27% prescriptions, followed by betamethasone diproprionate and hydrocortisone butyrate in 19% each. In a study carried out in India, potent TCS were commonly used in 43% patients [17]. Another study showed 94.36% of all topical steroids prescribed belong to very potent groups [18]. According to study by Jaiswal MK, et al. high potency corticosteroids were prescribed most frequently (55.34%) followed by moderate potency (33.48%) and very high potency drugs in 8.63% prescriptions [15]. In contrast to this, the majority of the topical corticosteroids prescribed were of low potency (47%) while ultra-high and high potent drugs being 20% and 33% respectively in Sharma S, et al. [16]. This pattern of prescription may be influenced by the availability of the preparation in the hospital pharmacy and the choice of the dermatologist.
In a study by Uppal R, et al. quantity of topical steroid was mentioned in only 4%, frequency of administration in 77%, the site of administration in 69%, and duration of treatment in 55% of the total prescriptions [19]. In Sharma et al, the site of administration in 25%, and frequency of administration and duration of treatment in 100% of the total prescriptions [16]. In Jaiswal MK, et al. duration of application was not mentioned in 62.95% [15]. Not specifying the quantity can result in under or over usage of the drug. Under usage of the preparation may cause sub-therapeutic outcome, at the same time excessive usage can result in unwanted effects [4, 20]. In our study quantity, frequency, site and duration was mentioned in all prescription of which 73% were advised twice daily application followed by 25% once daily application and 2% for once a week application. Maximum 50% prescriptions of TCS were for 7-15 days followed by 24% for 16 days- 1 month duration. The site of application was mentioned in 70% prescriptions among which lower limbs (28%) were the most common site followed by genitals in 25% and upper limbs in 11%.
Fixed drug combination was prescribed in 3% prescriptions among all in our study. Similar to which very less corticosteroids were given as combination products in Jaiswal M, et al. study [15] and less than one-third of the steroids were given as combination products in Rathod SS, et al. study [18]. This was in contrast to the study by Mirshad PV, et al. where FDCs consisted of 47.5% of the formulations [13]. Use of combination drugs with TCS do not have any added benefit to that of plain TCS so irrational use of FDCs should be avoided.
Physicians and dermatologists must be aware of giving proper advice to the patients about the amount of topical steroid to be applied on different parts of the body. Use of the fingertip unit (FTU) method is a simple tool to help doctors and patients obtain a better understanding of the amount of topical steroid to be used. The risk of side-effects increases with steroid potency and the amount used [7]. In our study finger tip unit was explained and documented in only 3% prescriptions which should be promoted to reduce the variations in the use of TCS and to encourage adherence to therapy. Emollients were prescribed in 78% with explanation about the method of application as they have ‘steroid sparing effect’ which reduces the amount of TCS used.
Conclusion
The most common indication for prescribing topical steroids was eczema in our study. Prescribing practice of high potent and moderate potent topical corticosteroids was found to be high. The most common molecule of topical steroid prescribed was betamethasone valerate. Use of the drugs mostly by generic names is a welcome initiative towards the rationality, seen in current study. Advice about finger tip method application was not a routine practice.
Future plans
- To do reaudit to evaluate improvement after creating awareness about the rational prescription of topical corticosteroids.
- Revise hospital formulary where low-potency steroids can also be made available.
- Continuing medical education for not only residents but also for undergraduates and general practitioners by giving them awareness about the use of combinations and importance of fingertip unit.
References
-
Saravanakumar RT, Prasad GS, Ragul G, Mohanta GP, Manna PK, et al. (2012) Study of prescribing pattern of topical corticosteroids in the department of dermatology of a multispecialty tertiary care teaching hospital in south India. Int J Res Pharm Sci 3(4): 685-687.
-
Schoepe S, Schacke H, May E, Asadullah K (2006) Glucocorticoid therapy-induced skin Atrophy. Exp Dermatol 15(6): 406-420.
-
Kumar MA, Noushad PP, Shailaja K, Jayasutha J, Ramasamy C (2011) A Study on drug prescribing pattern and use of corticosteroids in dermatological conditions at a tertiary care teaching hospital. International Journal of Pharmaceutical Sciences Review and Research 9(2): 132-135.
-
Sweileh WM (2006) Audit of prescribing practices of topical corticosteroids in outpatient dermatology clinics in north Palestine. East Mediterr Health J 12(1-2): 161- 169.
-
Fisher DA (1995) Adverse effects of topical corticosteroid use. West J Med 162(2): 123-126.
-
Noruka E, Okoye O (2006) Topical Steroid Abuse: It’s Use as a Depigmenting Agent. J Natl Med Assoc 98(6): 934- 938.
-
Darsow U, Wollenberg A, Simon D, Taieb A, Werfel T, et al. (2013) Difficult to control atopic dermatitis. World Allergy Organ J 6(1): 1-6.
-
Narwane SP, Patel TC, Shetty YC, Chikhalkar SB (2011) Drug Utilization and Cost Analysis for Common Skin Diseases in Dermatology OPD of an Indian Tertiary Care Hospital - A Prescription Survey. BJPR 1(1): 9-18.
-
Singh T, Banerjee B, Garg S, Sharma S (2019) A prescription audit using the World Health Organization- recommended core drug use indicators in a rural hospital of Delhi. J Educ Health Promot 8: 37.
-
Sarkar C, Das B, Sripathi H (2001) Drug Prescribing Pattern in Dermatology in a Teaching Hospital in Western Nepal. J Nepal Med Assoc 41: 241-246.
-
Saleem TKM, Dilip C, Nishad VK (2012) Assessment of Drug Prescribing Patterns in Dermatology Outpatient Department in a Tertiary Care Hospital, Malabar, Kerala. Indian Journal of Pharmacy Practice 5(3): 62-68.
-
Tikoo D, Chopra SC, Kaushal S, Dogra A (2011) Evaluation of Drug Use Pattern in Dermatology as a Tool to Promote Rational Prescribing. JK Science 13(3): 128-131.
-
Mirshad PV, Khan AKA, Fasalu ROM, Muneersha TKM (2013) Prescription audit of corticosteroid usage in the department of dermatology at a tertiary care teaching hospital. Int J Basic Clin Pharmacol 2(4): 411-413.
-
Oshikoya KA, Bello JA, Ayorinde EO (2008) Prescribing knowledge and skills of final year medical students in Nigeria. Indian J Pharmacol 40(6): 251-255.
-
Jaiswal M, Chakrawarty R, Sharma S, Sachdev D, Sharma R, et al. (2017) Prescription audit of Corticosteroids in Dermatology OPD of a tertiary care teaching hospital of tribal region of central-south India. IJBR 8(1): 20-25.
-
Sharma S, Shashidhar CV (2018) An Analysis of Prescription Patterns of Topical Corticosteroids in Dermatology OPD. Natl J Integr Res Med 9(2): 59-63.
-
The National Prescribing Centre (1999) Using topical corticosteroids in general practice. MeReC Bulletin 10(6): 21-24.
-
Rathod SS, Motghare VM, Deshmukh VS, Deshpande RP, Bhamare CG (2013) Prescribing practices of topical corticosteroids in the outpatient dermatology department of a rural tertiary care teaching hospital. Indian J Dermatol 58(5): 342-345.
-
Uppal R, Sharma SC, Bhowmik SR, Sharma PL, Kaur S (1991) Topical corticosteroids usage in dermatology. Int J Clin Pharmacol Toxicol 29(2): 48-50.
-
Ference JD, Last AR (2009) Choosing Topical Corticosteroids. Am Fam Physician 79(2): 135-140.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling