Palmar Tinea nigra Non-Invasive Diagnosis with Dermoscopy, Reflectance Confocal Microscopy and Microbiology
Tinea nigra is an uncommon superficial mycosis caused by the darkly pigmented fungus Hortaea werneckii. which occurs mainly in tropical and subtropical regions. Clinically, it is characterized by a brown-to-black asymptomatic macule, with welldefined edges, most commonly affecting the palms and soles. We report a case of palmar Tinea nigra and the features found on dermoscopy, reflectance confocal microscopy and microbiology. It is important to recognize this disease early for proper treatment and to distinguish it from other melanocytic lesions with worse prognoses, such as melanoma
Introduction
Tinea nigra is a superficial mycotic infection, which is located especially on the palm of the hand or sole of the foot, and remains in other parts of the body. Its etiologic agent is Hortaea werneckii. Tinea nigra has been diagnosed in several parts of the world, but the highest frequency is in the tropical and subtropical regions of the American continent, especially in countries like Brazil. The great importance of Tinea nigra is that it can sometimes be confused with malignant melanoma.
Clinical Presentation
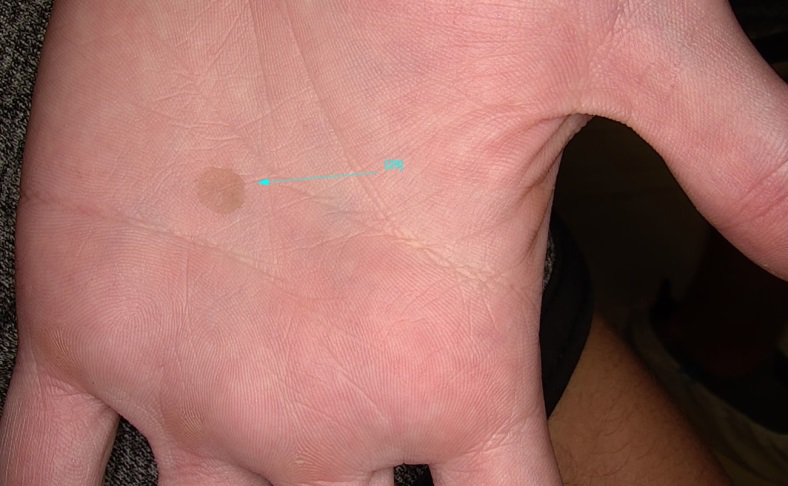
A 28-year-old man presented with an asymptomatic slow- growing patch in the palmar region, with 1-month history. Physical examination revealed a slightly scaly hyperchromic patch, with ill-defined borders, with a maximum diameter of 10mm, on the right palm (Figure 1).
Dermoscopic Appearance
Due to the hypothesis of Tinea nigra, dermoscopy examination was performed and showed a non-melanocytic pattern with speckled and superficial pigmentation (Figure 2).
Confocal Microscopy Appearance
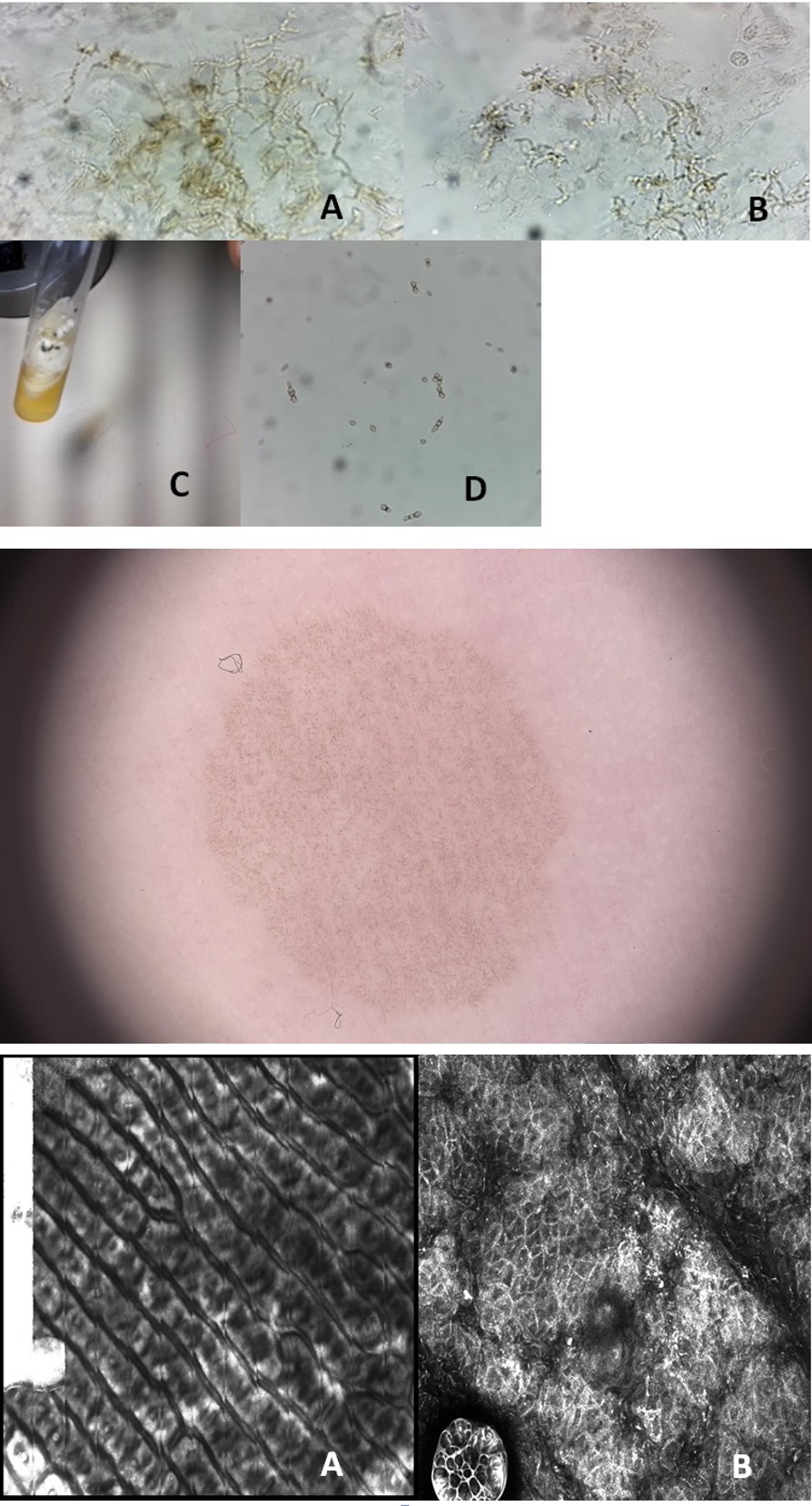
Reflective Confocal Microscopy (RCM) revealed high reflectivity of short and tortuous linear structures (Figures 3 A and B).
Figure 3A and B: Reflective Confocal Microscopy (RCM) reveals high reflectivity of short and tortuous linear structures.
Direct Mycological Examination and Culture
Direct mycological examination (DME) revealed septate, short and tortuous dematiaceous hyphae. The fungal microcultive presented demaceous fungus and culture isolated the agent Hortae werneckii confirming the diagnosis of Tinea nigra (Figures 4 A-D).
Figure 4A-D: A and B: Direct mycological examination (DME), fresh material blade mounted with 40% KOH revealed septate, short and tortuous dematiaceous hyphae; C: Tube with growth of etiologic agent Hortae werneckii; D: Crop slide mounted with cotton blue, culture isolated the agent confirming the diagnosis of Tinea nigra.
Treatment
The treatment was performed with the curettage itself for the mycological examination, followed by Isoconazol spray.
Discussion
Tinea nigra is a rare superficial keratophytosis caused by the dematiaceous fungus Hortae werneckii, which occurs mainly in tropical and subtropical regions. It is characterized by a brown-to-black asymptomatic macule, with well- defined edges, preferably affecting the stratum corneum of palms and soles [1, 2].
Clinically it may resemble a melanocytic palmoplantar lesion, including melanoma, which turns the immediate diagnosis important. Dermoscopy is very important to exclude diagnosis of melanocytic lesions, and is characterized by the presence of multiple, homogeneously arranged thin strands of brown dots or granules and short lines similar to spicules, which does not follow furrows or ridges pattern, also does not have another melanocytic pattern, as reticular or globular [2, 3].
Diagnosis is confirmed by direct mycological examination (DME), microculture e culture [4]. DME shows short, dark, septate, tortuous hyphae. Microculture is characterized by brownish septate hyphae and brownish bicellular conidia and culture reveals a greyish-white, wrinkled, membranous surface colony, and the reverse presented with black pigmentation [1, 2].
Reflectance Confocal Microscopy (RCM) is a non-invasive exam that increases the accuracy for diagnosis between melanocytic and non-melanocytic lesions. There are few cases in literature describing Tinea nigra aspects at RCM, though it is known that the exam allows observation of fungal structures, with high reflectivity of speckled appearance, similar to the ones observed on dermoscopy and to hyphae identified on DME. This correlation with microbiological findings of Tinea nigra, supports even more the clinical treatment, avoiding unnecessary excisions [2, 4].
It is important to recognize this disease early for proper treatment and to distinguish it from other melanocytic lesions with worse prognoses, such as melanoma.
References
-
Valentim FO, Lacerda PN, Haddad GR (2021) _Tinea nigra_: A series of three cases observed in Botucatu, São Paulo. Rev Soc Bras Med Trop 54: e0563-2020.
-
Verrinder JV, Avila RB, Ferreira MAMO, Lazzarini R (2017) Reflectance confocal microscopy of _Tinea nigra_: comparing images with dermoscopy and mycological examination results. An Bras Dermatol 92(4): 568-569.
-
Bakos RM, Leite LL, Reinehr C, Escobar GF (2021) Dermoscopy of skin infestations and infections (entomodermoscopy) - Part II: viral, fungal and other infections. An Bras de Dermatol 96(6): 746-758.
-
Uva L, Filipe PL, Almeida LS, Ferreira J (2018) Oliveira A. Reflectance confocal microscopy for the diagnosis of _Tinea nigra_. Clin Exp Dermatol 43(3): 332-334.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling