Vaginal Atrophy Vectors Technique – A Technique for Safe, Simple and Effective Vaginal Injection of Hyaluronic Acid
The injectable use of hyaluronic acid in the vaginal walls has demonstrated encouraging results in improving the symptoms of vaginal atrophy. The therapy has not yet settled, however, due to reports of associated non-thrombotic pulmonar embolism, in which an overdose of hyaluronic acid was injected into the deep layer of the anterior vaginal wall, an area of high vascular risk, by non-physicians. We have used a simple and safer technique since 2019, whereby only 1ml of hyaluronic acid is injected superficially, in the submucosal plane, through a blunt-tipped cannula, in the posterior wall, with excellent results and fewer complications.
Introduction
Vaginal atrophy (VA) is characterized by the variable association of flaccidity and genital dryness, burning, pain spontaneously or during sexual intercourse and urinary symptoms. It affects more than 90% of postmenopausal women and up to 20% of premenopausal women in conditions of hypoestrogenism, such as chronic users of anovulatory drugs, postpartum and postophorectomy [1].
The topical use of hyaluronic acid (HA) for the treatment of VA is well established [2, 3, 4, 5]. Injectable use however, alone [6, 7] or combined with other substances such as nanofat, plasma rich in platelets and peptides [8, 9, 10, 11], despite the excellent results described, has not yet been unequivocally established [12, 13] by reports of associated non-thrombotic pulmonary embolism [14, 15, 16, 17]. We have developed an injection technique, which we call the VA Vectors Technique, through which we have been performing the procedure in a simple and safer way, with excellent results, since 2019.
Methods
Since 2019, 22 women, aged between 35 and 66 years, with complaints of dryness and pain during intercourse received an injection of 1ml of HA, at a concentration of 20mg/ml, in posterior wall of vagina.
For analysis of results, in addition to obtaining images before and after the injection, we advise patients to answer the Sabbatsberg sexual self-assessment scale (SS) [11] (Table 1).
Sabbatsberg Sexual Self-Rating Scale
Please tick the appropriate answer (only one) for cach section. Please do not respond to any question that does not currently apply to you. Just mark such questions cicarly NA. Sexual activity includes intercourse, masturbation, oral sex, and anal sex.
1. a. My sexual interest during the past month has been: very great ( ) moderate ( ) little ( ) very little or nonexistent ( ) b. In comparison to previous years, my sexual interest is now: much greater ( ) greater ( ) unchanged ( ) less ( ) much less ( )
2. a. My sexual activity during the last month has been: very great ( ) great ( ) moderate ( ) little ( ) very little or nonexistent ( ) b. In comparison to previous years, my sexual activity is now: much greater ( ) greater ( ) unchanged ( ) less ( ) much less ( )
3. a. My sexual life during the last month has been: very satisfying ( ) satisfying ( ) rather satisfying ( ) less satisfying ( ) not satisfying ( ) b. In comparison to previous years, my sexual life is now: much more satistying ( ) more satisfying ( ) unchanged ( ) less satisfying ( ) much less satisfying ( )
4. a. Sex during the last month has given me: very great pleasure ( ) great pleasure ( ) moderate pleasure ( ) little pleasure ( ) no pleasure ( ) b. In comparison to previous years, sex now has given me: much greater pleasure ( ) greater pleasure ( ) the same pleasure ( ) less pleasure ( ) much less pleasure ( ) Table 1: Sabbatsberg Sexual Self-Rating Scale.
For the procedure, the passage of the speculum and vaginal asepsis with an aqueous solution of chlorhexidine were performed. Next, 1% lidocaine was injected into the vaginal furcula and a puncture was made in this location with a 21G needle. A 22G/5cm blunt-tipped cannula was introduced through this entry port for HA injection (Figure 1).

The cannula was positioned superficially, in the submucosa, and the injection of HA was performed in retroinjection, in 3 vectors, 1 central, which received about 0.4ml of HA and 2 lateral to the described one, which received 0.3ml each. The injection was performed only on the posterior wall, trying to distribute the HA only in the distal 5 cm of the vagina (Figure 2).
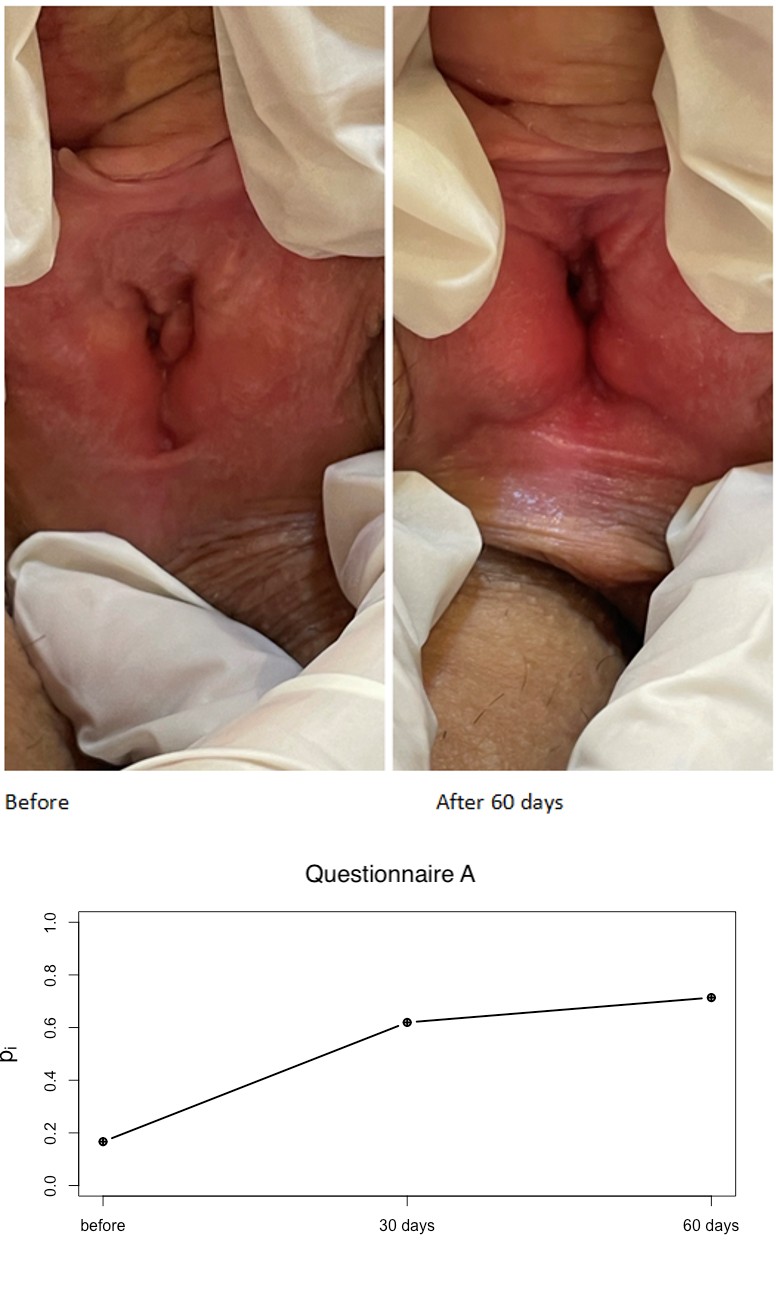
After injection, the product was accommodated with digital massage and we could note the mucosa quite hyperemic (Figure 3).
Vaginitis, active genital herpes, urinary infection, bleeding or vaginal discharge to be clarified, autoimmune diseases or any alteration in the specular evaluation contraindicated the procedure. Patients should not manipulate the vagina and remain sexually abstinent for 07 days. No local or systemic medication was prescribed. After this inicial treatment, biannual maintenance sessions can be carried out.
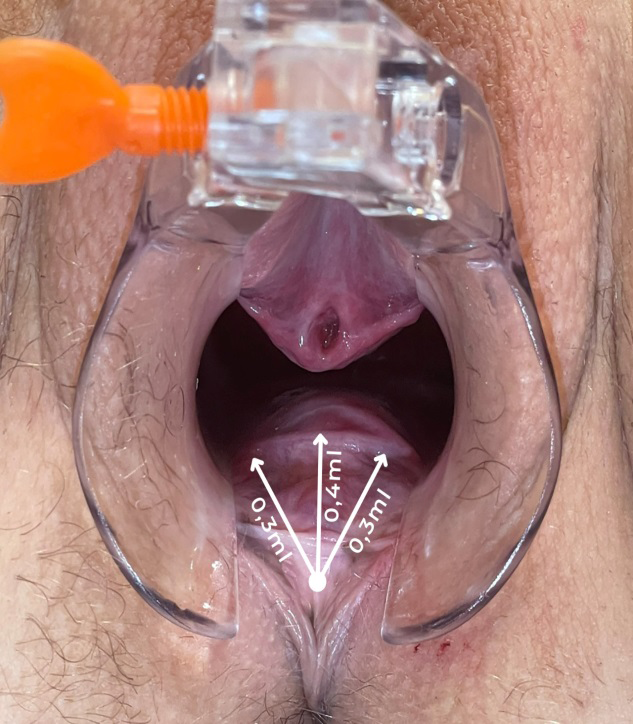
Figure 2: The injection of HA was performed in retroinjection, in 3 vectors, 1 central, which received about 0.4ml of HA and 2 lateral to the described one, which received 0.3ml each. The injection was performed only on the posterior wall, trying to distribute the HA only in the distal 5 cm of the vagina, where women have major complaints of dryness.

Results
Images were obtained before and after HA injection, showing that the mucosa was less pale and more hydrated after the treatment (Figure 4). The functional sexual improvement however, evaluated by the SS, were more expressive than the images (Table 2, Graph 1, Graph 2 and Table 3).
| Questionnaire A | Questionnaire B | |||||
|---|---|---|---|---|---|---|
| I-J | t Tukey | p | I-J | t Tukey | p | |
| Before – 30 days | -28,204 | -23,345 | < 0,001 | -30,182 | -22,336 | < 0,001 |
| After – 60 days | -34,250 | -18,989 | < 0,001 | -35,818 | -26,507 | < 0,001 |
| 30 days-60 days | -6,045 | 2,592 | 0,022 | -5,636 | -2,086 | 0,037 |
Table 1: Paired comparisons between groups.
Graph 1: Differences in measurement times considering the participants’ responses to the scale’s type A questionnaire.
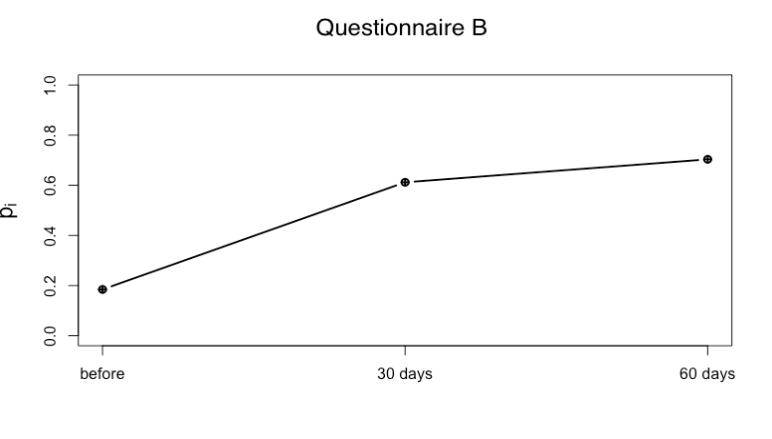
Graph 2: Differences in measurement times considering the participants’ answers to the scale’s type B questionnaire.
| Questionnaire A | Questionnaire B | |||||
|---|---|---|---|---|---|---|
| Rank Means | M | SD | Rank Means | M | SD | |
| Before | 12,681 | 2,049 | 0,756 | 11,500 | 2,034 | 0,729 |
| 30 days | 40,886 | 3,867 | 0,695 | 41,681 | 4,310 | 0,485 |
| 60 days | 46,931 | 4,136 | 0,521 | 47,318 | 4,504 | 0,428 |
Table 2: Descriptive statistics of the experiment.
All treated patients reported, to varying degrees, an increase in sexual interest, activity, and pleasure. We asked patients to consider not only intercourse but also masturbation, oral sex, and anal sex as sex. In the immediate post procedure period, the most common complaint was burning sensation when urinating, with spontaneous resolution within 24 hours.
We had three spontaneous extrusion of the injected HA. We believe that this occurred because we used HA with a higher G` in very atrophic mucous membranes, therefore we suggested HA with a lower cross link for vaginal injection. Indeed, when HA with less elasticity was injected, we did not have any complication.
Statistical Data Analysis
Initially, the results of the multivariate model indicated statistically significant differences between the measurement moments [Wald (2)= 592.732, p < 0.001], indicating that the effect of the intervention was significant. Therefore, univariate models were tested for each type of question (A; B).
The univariate model considering questions A of the Sabbatsberg Scale of Sexual Self-Assessment showed significant differences between measurements [Wald (2)= 504.796, p < 0.001], corroborating the findings of the multivariate model. From this, non-parametric paired comparison tests were performed, based on Tukey’s test, which can be seen in Table 2.
The results of the comparative tests indicated significant differences between all measurement periods, with a significant increase in the responses of the research participants to questions A of the scale used. It can also be inferred that the increase was greater when analyzing the periods before and 30 days, in addition to before and 60 days, marking the effectiveness of the intervention. In addition, the differences between the periods 30 days and 60 days after the intervention indicate that this effect was maintained, even if with less strength, during the 60 days of the intervention. The aforementioned effects can be seen in graph 01.
Similarly, when considering the responses to questionnaire B of the scale used, it was possible to observe significant differences in the repeated measures [Wald (2)= 528.348, p < 0.001], thus paired comparisons were performed. Tukey’s test showed results very similar to those of questionnaire A, in which it was possible to observe significant differences for all measurement times, with a significant increase between the three measured times, with an increase in the moment before and 30 days, in addition to before the intervention and 60 days higher than the increase observed between 30 days and 60 days. Such results confirm the previous findings, that the intervention had a significant effect during the 60 days, with significant differences between the moment before the intervention and the later moments. The effects can be seen from Graph 2.
Below, the descriptive statistics of the sample are presented, in order to contribute to the interpretation of the significant differences between the measurement moments (Table 3). The results point to a significant increase in the moment before the intervention when compared to the moment 30 days after the intervention. Similarly, it is possible to notice a slight increase in the results when comparing the moments after 30 days with after 60 days from the beginning of the experiment. However, it is important to emphasize that the comparison statistic of the test is the average of the ranks (Rank Means), as it is a non-parametric statistical test.
Discussion
Currently, alternatives for the treatment of VA are based on hormone replacement, the local use of vaginal lubricants and moisturizers and the application of vaginal technologies such as lasers and radiofrequency. However, hormone therapy is contraindicated in a considerable number of women, such as those with breast or endometrial carcinoma, unexplained vaginal bleeding, thrombotic and cardiovascular disease, porphyria, hepatobiliary disease, and systemic lupus erythematosus. Creams for vaginal use are considered uncomfortable for most women, which reduces adherence to treatment.
The devices, despite the promising results, are not approved by the FDA for the treatment of VA, and their use has been associated with serious adverse events, such as chronic vaginal pain [18]. HA is an essential polysaccharide in the maintenance of water balance, in the regulation of inflammation, in the immune response, in wound healing and in angiogenesis of skin and mucous membranes [19]. Histological analyzes demonstrated that the mucosa in VA, in addition to reduced vascularization and thickness, presents quiescent fibroblasts, reduced and dehydrated extracellular matrix and inversion of the proportion of collagen I-III, with altered trabecular architecture and elasticity [20].
The injection of HA into the vaginal mucosa is associated with the expression of the CoL1A1 and CoL3A1 genes, suggesting the stimulation of local collagen formation [6]. Studies have shown that vaginal injection of HA considerably improves the symptoms of mucosal atrophy [6]. Pulmonary complications of non-thrombotic embolism due to HA are uncommon, with only six reported cases of isolated injection of HA leading to such a complication. Of these, only two cases were associated with vaginal injection [14, 15, 16, 17].
It is believed that in these cases the embolism occurred due to the injection of HA in the anterior wall of the vagina [11], where there is an extensive venous plexus [21]. In addition, injections were performed with high amounts of HA, by non-medical professionals [14]. In the VA technique, we suggest the injection of only 1 ml of HA, to be injected superficially, gently, with a 22G cannula with a blunt tip and only in the posterior wall of the vagina, an area of lower vascular risk and where most patients report greater discomfort in relation to pain, dryness and fissures.
Conclusion
Injection of HA into the vaginal walls using the VA vectors technique is an outpatient, simple, low-cost, and reproducible procedure. The use of blunt-tipped cannulas, exclusive application to the posterior wall and use of small aliquots per session made the procedure safer and extremely effective in improving symptoms associated with VA.
References
-
Bride MBM, Rhodes DJ, Shuster LT (2010) Vulvovaginal atrophy. Mayo Clin Proc 85(1): 87-94.
-
Buzzaccarini G, Marin L, Noventa M, Vitagliano A, Riva A, et al. (2021) Hyaluronic acid in vulvar and vaginal administration: evidence from a literature systematic review. Climacteric 24(6): 560-571.
-
Santos CCMD, Uggioni MLR, Colonetti T, Colonetti L, Grande AJ, et al. (2021) Hyaluronic Acid in Postmenopause Vaginal Atrophy: A Systematic Review. J Sex Med 18(1): 156-166.
-
Origoni M, Cimmino C, Carminati G, Iachini E, Stefani C, et al. (2016) Postmenopausal vulvovaginal atrophy (VVA) is positively improved by topical hyaluronic acid application. A prospective, observational study. Eur Rev Med Pharmacol Sci 20(20): 4190-4195.
-
Chen J, Geng L, Song X, Li H, Giordan N, et al. (2013) Evaluation of the efficacy and safety of hyaluronic acid vaginal gel to ease vaginal dryness: a multicenter, randomized, controlled, open-label, parallel-group, clinical trial. J Sex Med 10(6): 1575-1584.
-
Berreni N, Salerno J, Chevalier T, Alonso S, Mares P (2021) Evaluation of the effect of multipoint intra-mucosal vaginal injection of a specific cross-linked hyaluronic acid for vulvovaginal atrophy: a prospective bi-centric pilot study. BMC Womens Health 21(1): 322.
-
Garavaglia E, Sala C, Busato M, Bellia G, Tamburlin N, et al. (2020) First Use of Thermal Stabilized Hyaluronic Acid Injection in One-Year Follow-Up Patients with Genitourinary Syndrome. Med Devices (Auckl) 13: 399- 410.
-
Angelucci M, Frascani F, Franceschelli A, Lusi A, Garo ML (2022) Efficacy of intradermal hyaluronic acid plus polynucleotides in vulvovaginal atrophy: a pilot study. Climacteric 7: 1-7.
-
Cohen PR, Riahi RR (2019) Platelet-Rich Plasma and Genital Rejuvenation. Skinmed 17(4): 272-274.
-
Hersant B, SidAhmed-Mezi M, Belkacemi Y, Darmon F, Bastuji-Garin S, et al. (2018) Efficacy of injecting platelet concentrate combined with hyaluronic acid for the treatment of vulvovaginal atrophy in postmenopausal women with history of breast cancer: a phase 2 pilot study. Menopause 25(10): 1124-1130.
-
Aguilar P, Hersant B, SidAhmed-Mezi M, Bosc R, Vidal L, et al. (2016) Novel technique of vulvo-vaginal rejuvenation by lipofilling and injection of combined platelet-rich- plasma and hyaluronic acid: a case-report. Springerplus 5(1): 1184.
-
Le C, Murgia RD, Noell C, Weiss M, Weiss R (2022) Female genitourinary treatments in aesthetics. Clin Dermatol 40(3): 259-264.
-
Zheng Z, Yin J, Cheng B, Huang W (2021) Materials Selection for the Injection into Vaginal Wall for Treatment of Vaginal Atrophy. Aesthetic Plast Surg 45(3): 1231- 1241.
-
Yang Y, Sheng H, Gu Q, Su L, Tong H, et al. (2020) Death Caused by Vaginal Injection of Hyaluronic Acid and Collagen: A Case Report. Aesthet Surg J 40(5): NP263- NP268.
-
Han SW, Park MJ, Lee SH (2019) Hyaluronic acid-induced diffuse alveolar hemorrhage: unknown complication induced by a well-known injectable agent. Ann Transl Med 7(1): 13.
-
Park HJ, Jung KH, Kim SY, Lee JH, Jeong JY, et al. (2010) Hyaluronic acid pulmonary embolism: a critical consequence of an illegal cosmetic vaginal procedure. Thorax 65(4): 360-361.
-
Kong J, Yang T, Yang X, Zhang F, Liao X, et al. (2023) Death from Pulmonary Embolism Caused by Vaginal Injection of Hyaluronic Acid: a Case Report and a Literature Review. Aesthetic Plast Surg 47(4): 1535-1541.
-
Smith J (2018) FDA warning shines light on vaginal rejuvenation. ObGynNews pp: 1-5.
-
Nusgens BV (2010) Acide hyaluronique et matrice extracellulaire: une molécule primitive ? Ann Dermatol Venereol 137: S3-8.
-
Fadare O (2011) Vaginal stromal sclerosis: a distinctive stromal change associated with vaginal atrophy. Int J Gynecol Path 30: 295-300.
-
Cunningham FG, Leveno KJ, Dashe JS, Hoffman BL, Spong CY, et al. (2010) Maternal anatomy. In: Williams obstetrics. New York: McGraw-Hill (26thEdition) pp: 17- 8.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling