Exploring Treatment Options for Methicillin-Resistant Staphylococcus Aureus through a Mixed Methods Approach
Methicillin-resistant Staphylococcus aureus (MRSA) is a major public health concern, demanding multifaceted treatment strategies due to its complex nature. This study aimed to bridge the gap in understanding MRSA's clinical presentation, management, and outcomes by employing a mixed-methods approach. Through an extensive literature review and a singlecenter retrospective patient record review, the study offered insights into MRSA management, from diagnosis to treatment. The analysis included 44 patients, who presented to an outpatient dermatology practice. Results found a broad age range, revealing that 68.2% were treated with both topical and oral medications. Antibiotic susceptibility tests showed high resistance to Penicillin (84.1%) and high susceptibility to drugs like Linezolid (95.5%) and Moxifloxacin (97.7%). The literature review examined 22 relevant articles from the past decade. The study's findings emphasize the diversity of MRSA infections and the challenges in treatment, highlighting variations in antibiotic susceptibility and the urgent need for innovative approaches. It serves as a substantial contribution to the existing body of knowledge on MRSA and may inform future research and clinical practice.
Introduction
Methicillin-resistant Staphylococcus Aureus (MRSA) has emerged as a significant public health concern, leading to an array of infections that range from superficial skin infections to severe systemic illnesses. The complex nature of MRSA infections has prompted the necessity for varied treatment approaches, taking into consideration the location of the infection, culture sensitivities, and the unique clinical presentation of each case. While numerous research efforts have been directed toward understanding MRSA infections, there exists a gap in synthesizing contemporary management strategies and analyzing real-world patient data across diverse clinical settings. The rising prevalence of MRSA and the associated challenges in its management underscores the need for a comprehensive investigation into the current state of diagnosis, treatment, and outcomes.
The aim of this study is to fill this gap by exploring the clinical presentation, management, and outcomes of MRSA infections, with a particular emphasis on the differences in treatment strategies, locations of infection, and culture sensitivities. By employing a mixed-methods approach that combines an extensive literature review with a single-center, outpatient dermatology clinic, retrospective patient record review, and this study seeks to offer a multifaceted insight into MRSA management. This approach not only facilitates an understanding of the broader context through a review of existing literature but also offers a granular perspective through the analysis of real-world patient data from a specific healthcare center.
Methodology
The aim of this study was to explore the clinical presentation, management, and outcomes of MRSA infections, focusing on the differences in treatment strategies, locations of infection, and culture sensitivities. We adopted a mixed- methods approach, including a comprehensive literature review and a single-center retrospective patient record review. This methodology provided a broad perspective on MRSA management strategies and enabled the analysis of real-world patient data.
A comprehensive search was conducted on PubMed using specific keywords related to MRSA, including treatment, therapy, management, incision and drainage, topical treatment, antibiotics, antimicrobial therapy, culture sensitivities, and antibiotic susceptibility. Only articles published within the last 10 years that were available in full text and English language were considered. Additionally, the results were filtered for meta-analyses, randomized controlled trials (RCTs), and systematic reviews. For each article, relevant data were extracted, including study design, population characteristics, intervention details, and outcomes. A narrative synthesis of the findings was conducted.
A single-center retrospective chart review was conducted at Borealis Dermatology Clinic. The electronic health records (EHR) of patients diagnosed with MRSA were included from December 11, 2020, to July 31, 2023. We included adult patients (≥18 years old) with laboratory-confirmed MRSA infections. Patients with incomplete records or not treated at the center were excluded. For each eligible patient, the following data were extracted: demographics, including age and gender, treatment strategies, infection location, and culture sensitivities. Descriptive statistics were used to analyze the data. Continuous variables were presented as mean ± standard deviation (SD). Categorical variables were presented as frequencies and percentages. This study was approved by the Borealis Dermatology Clinic Institutional Review Board (IRB). Given the retrospective nature of the study, informed consent was waived. All data were anonymized to protect patient privacy.
Results
Single-Center Retrospective Chart Review
The study population consisted of 44 participants. The gender distribution was slightly skewed towards males, with 50% (n = 22) male and 45.5% (n = 20) female. The age of the participants ranges from 6 to 85 years. The mean age of the participants was approximately 34.88 years (SD = 15.71). This indicates a relatively wide dispersion in the study participants’ ages, with a spread of about 15.7 years above and below the mean.
In the context of treatments administered, 13.6% of participants (n = 6) received only topical treatment, and the same percentage received only oral medication treatment. However, 68.2% (n = 30) of participants received both topical and oral treatments. Approximately 42% were prescribed mupirocin, while 26% were treated with doxycycline, 38% sulfamethoxazole-trimethoprim, and 8% cephalexin.
Looking at the distribution of the affected body parts, it was found that 11.4% (n = 5) of the cases affected the arm/ hand, 34.1% (n = 15) affected the face/head, 4.5% (n = 2) involved the genital region, 13.6% (n = 6) pertained to the leg/foot, and 31.8% (n = 14) affected the torso. There was one case (2.3%) where multiple body parts were affected. Regarding the side of the body affected, the data show a slight leaning towards the right side, with 47.7% (n = 21) of the cases. 38.6% (n = 17) of the cases affected the left side, and 11.4% (n = 5) affected both sides. In the category of incision and drainage, slightly more than half of the participants, 52.3% (n = 23), did not have this procedure, while 45.5% (n = 20) did.
Antibiotic Susceptibility
For Ciprofloxacin, 27.3% of samples showed resistance, while 70.5% were susceptible. Clindamycin presented with 29.5% resistance, 65.9% susceptibility, and 2.3% inconclusive results. A significant resistance of 59.1% was observed in the Erythromycin samples, with 38.6% being susceptible. Gentamicin had a high susceptibility rate of 95.5%, with only 2.3% of inconclusive results. Levofloxacin results were 20.5% inconclusive, 4.5% resistant and 72.7% susceptible. Similarly, Linezolid had a high susceptibility rate of 95.5%, with only 2.3% of results inconclusive. Almost all the samples (97.7%) were susceptible to Moxifloxacin. Oxacillin revealed resistance in 34.1% of samples, with 63.6% showing susceptibility. Penicillin showed a high resistance rate of 84.1%, with only 11.4% being susceptible. Quinupristin/Dalfopristin had a very high susceptibility rate, with 97.7% of samples susceptible. Resistance was minimal at 2.3% for Rifampin, while 95.5% were susceptible.
Tetracycline displayed resistance in 6.8% of the samples, but the vast majority, 90.9%, were susceptible. Trimethoprim/ Sulfa showed 11.4% resistance and 86.4% susceptibility.
Lastly, almost all samples, 97.7%, were susceptible to Vancomycin (Figure 1).

Literature Review
The initial search yielded 44,473 results. Refining the search to include terms related to treatment, therapy, or management narrowed the results to 26,155 articles. Further specificity was added by integrating keywords associated with incision and drainage, topical treatment, oral antibiotics, or antimicrobial therapy, which brought the results to 15,093. Introducing the criteria of culture
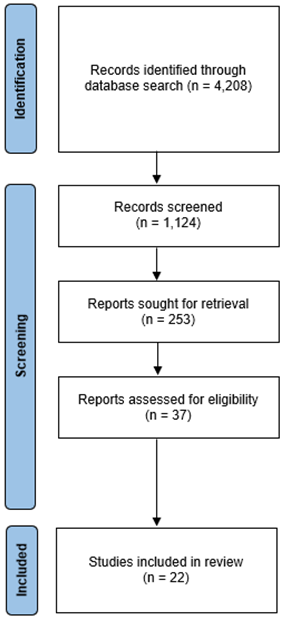
sensitivities or antibiotic susceptibility, the search yielded 4,208 articles. After applying filters to select articles from the past 10 years that were full text and in English, 1,124 articles remained. Subsequently, filtering for meta-analyses, randomized controlled trials (RCTs), and systematic reviews resulted in 37 articles. After thoroughly reviewing these articles, 22 were deemed relevant and retained for the study (Figure 2).
The Burden of MRSA
MRSA has emerged as a major nosocomial pathogen, leading to severe morbidity and mortality. Its grave impact has led to its classification as a high priority by the World Health Organization (WHO) and a serious threat by the Centers for Disease Control and Prevention (CDC), highlighting its global significance [1]. The economic burden of MRSA is substantial, with associated consequences including increased hospital costs, prolonged hospital stays, and higher mortality rates. Staphylococcus aureus, encompassing MRSA, continues to be a global health challenge, giving rise to serious infections and hefty economic burdens [2]. Mortality rates are alarming, with figures as high as 60%, and it causes 80,000 invasive infections and results in 11,000 deaths yearly. In the US alone, healthcare costs attributable to MRSA reach up to $3-4 billion annually [3].
The worldwide burden of MRSA infections underscores the imperative to identify optimal treatments to curb this threat [4]. Meanwhile, antibiotic resistance (ABR) is escalating at a global level, imperilling the health of populations around the world. Driven by factors such as overuse, misuse, slow changes in prescription behaviour, and natural evolution, ABR is expected to have severe consequences, including a potential loss of 1.1–3.8% of global GDP by 2050 and pushing 24 million people into poverty by 2030 [5]. The broader issue of antibiotic resistance is a significant public health concern. Overuse of antibiotics leads to increasingly resistant pathogens, resulting in an estimated extra cost of $22 billion annually in the US alone [6]. The problem extends to community-associated MRSA (CA-MRSA), which has become a common cause of purulent SSTIs worldwide [7]. Efforts to guide therapy through rapid molecular-based diagnostic tests and shifts in practice guidelines are part of the response to this challenge [4, 6].
The financial toll of ABR is immense, amounting to $20 billion in the US and €1.1–1.5 billion in the EU annually. While the World Health Organization (WHO) has laid down a global action plan for individual countries to battle ABR, the absence of comprehensive economic evaluations of ABR’s burden serves as an obstacle to its effective implementation. ABR in ESKAPE organisms is often linked with higher economic burdens, although some studies report no significant differences or even reduced costs in particular scenarios [5]. Differences in healthcare systems, medical pricing, insurance, treatment traditions, and study design account for varying costs across countries, further complicating the global fight against ABR.
MRSA infections are linked to increased morbidity, longer antibiotic therapy, higher healthcare costs, prolonged hospitalization, and an increased risk of death [8, 9]. Such infections can lead to various severe conditions, including bacteraemia, osteomyelitis, endocarditis, and sepsis [3]. Therapeutic options for MRSA are limited, and the resistance to conventional treatments such as vancomycin and linezolid is decreasing their effectiveness [10]. This has led to development and licensing of several new agents, like telavancin, dalbavancin, oritavancin, and tedizolid, characterized by enhanced properties [10]. However, more research is needed to support the effectiveness of these alternatives [10].
Some emerging solutions include the development of probiotics as low-cost alternatives for S. aureus decolonization and addressing the broader issue of drug-resistant infections that are increasingly hard to quantify [11, 12]. The World Health Organization (WHO) has identified a priority list of antibiotic-resistant (ABR) organisms, including ESKAPE organisms like Enterococcus spp. and Staphylococcus aureus, which consistently escape commonly used antibiotics [5].
Immune Response to S. aureus
The immune response to Staphylococcus aureus (S. aureus) represents a complex interaction that engages innate and adaptive immune cells. The role of immune tolerance has been an area of investigation, with the hypothesis that S. aureus colonization might lead to the immune system’s tolerance, thereby predisposing individuals to subsequent infections [13]. However, recent findings argue against these ideas, suggesting that colonization does not necessarily desensitize the immune response to the pathogen, nor does infection dampen immune responses [13].
Several critical components of the immune response to S. aureus have been identified, with implications for understanding and potentially intervening in these infections. In particular, S. aureus has been found to activate both innate and adaptive immune cells, thereby signaling immune cells and promoting inflammation [13]. The role of the cytokine IL-6 in anti-S. aureus immunity has been highlighted, and associations have been noted between anti-IL-6 antibodies and recurrent infection [13].
Emerging data also highlight the potential role of T cells in protection against S. aureus, particularly in skin and soft tissue infections (SSTIs). A link between T cell IL-17 and IL-22 and protection against SSTIs has been discovered, pointing to a complex interaction between various immune components in response to this pathogen [13]. These insights into the immune response to S. aureus provide a nuanced understanding of how the immune system engages with this organism, leading to potential implications for vaccine development and therapeutic interventions.
Resistance Rates
Resistance to antibiotics is a growing concern worldwide, with regions experiencing significant resistance rates to specific antibiotics. A study by Azzam A, et al. provided insight into the resistance rates for Vancomycin and Linezolid, reporting 9% (95% CI: 6–12) and 5% (95% CI: 2–8) resistance rates, respectively [1]. These figures are alarming as these antibiotics are commonly used to treat infections caused by MRSA. Furthermore, the rates of levofloxacin non susceptibility for MRSA have been observed to be staggeringly high, with figures reaching 58.8% in the U.S. and 84.9% in Europe [14]. Such high levels of resistance complicate the clinical management of these infections, potentially leading to treatment failures and increased morbidity and mortality.
The prevalence of resistance to Mupirocin varies across different regions. In the Americas, the highest pooled prevalence of mupirocin-resistant MRSA strains was reported at 10.5%, with Europe and Asia having resistance rates of 6.6% and 7.3%, respectively [2]. The prevalence of high- level mupirocin resistance is nearly the same for S. aureus and MRSA, with higher rates of resistance in Asia at 12.1% compared to Europe (8.0%) and the Americas (5.9%) [2]. Furthermore, an increasing trend in the overall prevalence of mupirocin-resistant MRSA strains was observed between 2011-2015 [2].
In a global context, high resistance rates are not isolated to specific antibiotics or regions. Reports indicate that more than 50% resistance to particular antibiotics exists in five out of six WHO regions for certain organisms [5]. These statistics paint a grim picture of the global landscape of antibiotic resistance, emphasizing the urgent need for concerted efforts to develop new antibiotics, implement stringent stewardship programs, and invest in research to understand resistance mechanisms better. The data collectively emphasize the serious public health threat posed by increasing antibiotic resistance rates and the importance of multidisciplinary strategies to combat this growing challenge.
For outpatient care, where the goal is to provide effective and convenient treatment regimens that minimize hospital visits and promote patient adherence, understanding these trends is crucial. The high resistance rates observed globally and nationally may prompt healthcare providers to favour certain oral antibiotics known for their lower resistance profiles or to consider alternative. This strategic shift aims to balance the effectiveness of treatment against the risk of contributing to further resistance. Consequently, in outpatient settings, the choice of antibiotic therapy increasingly relies on updated regional resistance data, the patient’s history of antibiotic response, and the practicalities of administering and monitoring the treatment, thereby ensuring that management strategies are both evidence- based and tailored to the specific needs of the community [2].
Treatment with Mupirocin
Mupirocin is a significant antibiotic in the fight against Staphylococcus aureus, including Methicillin-Resistant Staphylococcus aureus (MRSA) and Methicillin-Sensitive Staphylococcus aureus (MSSA). As the only approved antibiotic for decolonizing these strains, it functions by inhibiting protein synthesis, thereby demonstrating bacteriostatic activity [2, 15]. The antibiotic works by binding to isoleucyl-tRNA synthetase (IleS) and has become an essential tool in infection control [16].
Despite its crucial role, the emergence of mupirocin resistance is a growing concern. Two types of resistance, high- level and low-level, have developed after widespread use, with high-level resistance even found transferable between strains [2]. Disturbingly, the emergence of resistance in MRSA strains has been documented, and topical application does not eliminate strains with high or low-level mupirocin resistance [2]. These trends underscore the need for greater awareness and control measures, including education for reducing the prevalence of resistant strains and monitoring unrestricted use of mupirocin [2]. Despite the alarming trends, it is worth noting that the prevalence of mupirocin- resistant MRSA remains low in many settings [16].
In England, where mupirocin is widely used to prevent MRSA infection, even in the absence of specific guidelines, varying prevalence and transmission probabilities of mupirocin-sensitive (MupS) and mupirocin-resistant (MupR) strains have been identified in different hospital settings [16]. Interestingly, risk ratios suggest that MupS strains may have a higher probability of transmitting in certain environments [16].
Treatment with Beta-Lactam Medications
The shift towards using anti-Staphylococcal β-lactams represents an evolving strategy in treating MRSA infections, driven partly by emerging challenges with traditional therapies. Emonet, et al. have suggested that the switch to anti-Staphylococcal β-lactams is not only safer but also improves patient outcomes [17]. In dealing with complicated MRSA bacteremia, the Infectious Diseases Society of America (IDSA) recommends the use of high-dose daptomycin (DAP), with the Food and Drug Administration’s (FDA) recommended dosage for DAP being 6 mg/kg/day [3]. Retrospective studies have revealed the benefits of administering higher dosages of DAP, although this approach has also raised concerns about resistance [3]. Consequently, attention has turned towards alternatives such as β-lactams, particularly ceftaroline, which has shown promise In Vitro against MRSA strains resistant to vancomycin or DAP [3].
The potential benefits of β-lactams extend to combination treatments, which have been investigated in retrospective studies. These studies have revealed mixed results regarding the efficacy and safety of β-lactam combination treatment [3]. While some research has shown no significant difference in clinical outcomes with β-lactam combination treatments, other studies have found reduced 30-day mortality rates [3]. However, evidence also suggests an increased risk of acute kidney injury with β-lactam combination treatments, further highlighting the complexity of this therapeutic approach [3]. However, β-lactams have been noted for superiority over vancomycin, with current guidelines favoring drugs such as cefazolin and anti-Staphylococcal penicillins (ASPs) [18]. Specifically, the efficacy of cefazolin has been emphasized for its role in reducing death rates, clinical failure, hepatotoxicity, and nephrotoxicity, making it a favoured option for MSSA management [18].
Treatment with Azithromycin
Azithromycin, a widely-used antibiotic, has been the subject of attention due to the emergence of antimicrobial resistance, which resonates globally across various bacterial pathogens. This issue is highlighted in recent studies, which provide a nuanced perspective on azithromycin resistance [19]. Interestingly, the evidence surrounding azithromycin resistance is somewhat contradictory. While some studies have found no evidence of resistance emergence, others have detected signs of resistance, illustrating the complexity and variability of this phenomenon across different contexts and bacterial strains [19]. Specifically, the impact of azithromycin resistance has been noted in countries such as Burkina Faso and Mali, where the effect on pneumococcal resistance has been identified. These findings indicate that geographical variations and localized factors might play a significant role in the patterns of resistance to azithromycin [19].
Treatment with Tedizolid
Tedizolid phosphate represents an exciting advancement in the field of antibiotics, specifically for the treatment of acute bacterial skin and skin structure infections (ABSSSI), including those caused by the notoriously difficult-to-treat Methicillin-resistant Staphylococcus aureus (MRSA) [4]. Clinical findings have begun to shed light on Tedizolid’s promising therapeutic profile. Studies have demonstrated its superiority to vancomycin, a previously well-regarded treatment for similar infections, and have found Tedizolid to be equivalent in clinical response with other existing drugs used to treat these conditions [4]. This evidence marks Tedizolid as an efficacious option and a preferable one in certain scenarios.
The conclusion drawn from a network meta-analysis (NMA) has further bolstered Tedizolid’s standing as a valuable addition to the antibiotic armamentarium. This extensive analytical approach has showcased Tedizolid as a potential alternative option specifically for managing serious skin infections that are suspected or documented to be caused by MRSA [4]. The insights provided by the latest research, including NMA, will likely guide clinicians in making more informed decisions about the most appropriate and effective treatment strategies for their patients [4].
Treatment with Delafloxacin
Delafloxacin, a novel investigational anionic fluoroquinolone antibiotic, has begun to make significant strides in the medical field, showing promise as a potential treatment for various bacterial infections [14], [20]. One key feature of delafloxacin is its broad-spectrum In Vitro activity against an array of pathogens. It demonstrates effectiveness against Gram-positive and Gram-negative organisms, anaerobes, and atypical respiratory tract pathogens, expanding its potential applications [14]. Particularly noteworthy is its excellent In Vitro activity against Gram- positive pathogens, including Methicillin-resistant Staphylococcus aureus (MRSA), which is 32-fold more active against MRSA than levofloxacin [20].
Recent phase 3 studies have further solidified delafloxacin’s standing by demonstrating its non-inferiority to existing treatments, including the widely-used levofloxacin [14]. Moreover, when administered intravenously (IV) followed by an oral regimen, delafloxacin was found to be non-inferior to the combination therapy of IV vancomycin and aztreonam [20]. The potential of delafloxacin is further underscored by its stability against resistance. Studies have revealed no emergence of resistance and a low probability of selecting resistant mutants, indicating a reduced risk of contributing to the growing global problem of antibiotic resistance [20]. Additional attributes such as minimal potential for drug interactions and a well-tolerated profile comparable in clinical activity to vancomycin only add to the growing interest in this compound as a potential alternative in antimicrobial therapy [20].
Treatment with Trimethoprim- Sulfamethoxazole (TMP-SMX)
Trimethoprim-sulfamethoxazole (TMP-SMX) is an older antibiotic known for its activity against Staphylococcus aureus, including MRSA [21]. Despite decades of exposure to this antibiotic, the susceptibility of MRSA isolates remains fairly consistent in many regions worldwide, although resistance rates have exhibited significant variation across different regions [21]. Resistance rates have reached as high as 30% in Australia and 85% in India [21]. Previous observational studies have shed light on TMP-SMX as a possible alternative to vancomycin for treating MRSA infections, reporting similar or even favorable outcomes [21]. However, not all findings were promising, as TMP-SMX did not meet the criteria for non-inferiority to vancomycin, and an absolute difference in treatment failure rates at day 7 was found to be 10.4% in favor of vancomycin [21]. In fact, treatment with TMP-SMX was significantly associated with treatment failure, with an odds ratio of 2.00 [21]. Interestingly, the bacteriological cure and adverse event rates remained similar between the groups, and the trial did not define exclusion criteria related to illness severity, making it a pragmatic approach [21].
In the context of community-acquired MRSA (CA- MRSA) in the United States, TMP-SMX and clindamycin have been frequently utilized to treat infected wounds [7]. A randomized, double-blind trial comparing these two antibiotics revealed similar cure rates and adverse event rates between the two [7]. The results summary from this trial showed comparable cure rates for both clindamycin and TMP-SMX, although clindamycin exhibited a lower rate of recurrent infection [7]. This differential effect regarding recurrence has been identified as an area that may require further investigation [7]. Overall, the utilization of TMP- SMX presents a complex picture, with notable strengths in combating certain infections but significant limitations compared to other treatments like vancomycin. The regional variability in resistance, combined with nuanced clinical outcomes, indicates that TMP-SMX’s role in managing MRSA infections must be carefully considered and may be more suited to specific contexts or used in combination with further research [7, 21].
Treatment with Chlorhexidine Gluconate
Chlorhexidine gluconate (CHG) is an antiseptic that plays a vital role in infection control, especially in the context of universal decolonization. Its mechanism of action involves binding to the bacterial cell membrane, leading to disruption and death of the bacterial cells [15]. A notable aspect of CHG is the low prevalence of nonsusceptibility, meaning that resistance to this compound is relatively rare, enhancing its utility in various clinical settings [15]. In the fight against infections, a combined approach utilizing CHG and mupirocin is superior to other strategies. This combination appears to be particularly effective in decolonizing patients of specific bacterial strains, thus reducing the risk of subsequent infections [15]. Interestingly, a secondary analysis of the application of CHG, particularly in conjunction with mupirocin, showed no significant change in mupirocin resistance or CHG susceptibility [15]. This stability in susceptibility levels further emphasizes the potential longevity and efficacy of CHG as a crucial part of infection control protocols.
Treatment with Lactobacillus Rhamnosus
Lactobacillus rhamnosus (L. rhamnosus) has recently attracted attention in the field of medical research for its potential to reduce colonization within the gastrointestinal (GI) tract. A study by Eggers et al. investigated the particular strain L. rhamnosus HN001 and found that it reduced MRSA colonization in the stool, especially for subjects originally colonized outside the GI tract [11]. Interestingly, the reduction was not observed at other body sites. The mechanism through which L. rhamnosus HN001 may achieve this reduction appears to involve competitive inhibition within the GI tract, coupled with the stimulation of systemic immune function [11]. This dual-action approach sets L. rhamnosus HN001 apart from other interventions and suggests a targeted impact on GI-related health.
Challenges in MRSA Research
Research in the field of MRSA presents several challenges, as identified by recent studies. Dadashi et al. noted significant limitations in existing research, including the lack of studies conducted in African regions, potential publication bias, and insufficient data [2]. These gaps may hinder a comprehensive understanding of MRSA in diverse populations and its various treatment methodologies. Additionally, McCool et al. emphasized the difficulties in directly comparing the relative efficacy of new and established agents, as Randomized Controlled Trials (RCTs) are both expensive and complex to execute [4]. This indirect comparison may lead to potential biases in the evaluation and could limit the development and optimization of treatment strategies for MRSA. The highlighted challenges call for a more coordinated global effort and methodological innovations in MRSA research to build a robust evidence base for understanding and combating this prevalent bacterial infection.
Conclusion
The conclusion of this study offers a comprehensive overview of the clinical presentation, treatment strategies, and outcomes of MRSA infections, revealing insights into the intricacies of MRSA management. The study’s single-center sample consisted of a slightly male-dominated distribution, encompassing a wide age range from 6 to 85 years, with a mean age of 34.88 years (SD = 15.71), indicating a substantial dispersion around the mean. The distribution mirrors the generalized population, where MRSA can affect individuals across various age groups and both genders, reinforcing the complexity of managing this infection [1, 13].
In examining treatment modalities, the study found that most participants (68.2%) were administered both topical and oral treatments, aligning with the common practice of using a combination of therapies for effective MRSA management. Among the antibiotics prescribed, sulfamethoxazole-trimethoprim was utilized in 38% of the cases. This is consistent with previous findings that this particular antibiotic has been active against Staphylococcus aureus, including MRSA, though resistance varies across regions [7], [21]. The study further revealed the distribution of affected body parts, providing insights into the localized nature of MRSA infections. The antibiotic susceptibility testing showed varying levels of resistance and susceptibility to different antibiotics. High susceptibility rates were observed for Linezolid (95.5%), Moxifloxacin (97.7%), Quinupristin/ Dalfopristin (97.7%), and Vancomycin (97.7%). Conversely, Penicillin demonstrated a high resistance rate of 84.1%. This aligns with the increasing global concern of antibiotic resistance, which has intensified the challenges of MRSA management [1, 2].
The study’s methodology, encompassing a detailed literature review and a single-center retrospective patient record review, allowed for a nuanced understanding of MRSA management [8, 16, 22]. Ethical considerations were also meticulously observed to maintain the integrity of the research. In conclusion, this investigation highlights the multifaceted nature of MRSA infections and the intricacies of their treatment, shedding light on variations in antibiotic susceptibility, demographic trends, and the anatomical sites most commonly affected. Importantly, the findings enrich the current understanding of MRSA, offering valuable insights for tailoring outpatient management strategies against this pervasive and challenging infection. The study not only contributes to the broader knowledge base surrounding MRSA but also underscores the necessity for ongoing research and innovation in clinical practices, especially in the context of escalating antibiotic resistance. It calls for continued exploration of novel therapeutic approaches, emphasizing the critical need for individualized, patient- centric care in both outpatient and inpatient settings.
Conflicts of Interest
None to declare.
Disclaimer
This research was supported (in whole or in part) by Borealis Dermatology and/or Borealis Dermatology affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of Borealis Dermatology or any of its affiliated entities.
References
-
Azzam A, Khaled H, Mosa M, Refaey N, Saifi MA, et al. (2023) Epidemiology of clinically isolated methicillin- resistant Staphylococcus aureus (MRSA) and its susceptibility to linezolid and vancomycin in Egypt: a systematic review with meta-analysis. BMC Infect Dis 23(1): 263.
-
Dadashi M, Hajikhani B, Sarokhalil DD, Belkum A, Goudarzi M (2020) Mupirocin resistance in Staphylococcus aureus: A systematic review and meta- analysis. J Glob Antimicrob Resist 20: 238-247.
-
Mahjabeen F, Saha U, Mostafa MN, Siddique F, Ahsan E, et al. (2022) An Update on Treatment Options for Methicillin-Resistant Staphylococcus aureus (MRSA) Bacteremia: A Systematic Review. Cureus 14(11): e31486.
-
Cool R, Gould IM, Eales J, Barata T, Arber M, et al. (2017) Systematic review and network meta-analysis of tedizolid for the treatment of acute bacterial skin and skin structure infections caused by MRSA,” BMC Infect Dis 17(1): 39.
-
Zhen X, Lundborg CS, Sun X, Hu X, Dong H (2019) Economic burden of antibiotic resistance in ESKAPE organisms: a systematic review. Antimicrob Resist Infect Control 8: 137.
-
May LS, Rothman RE, Miller LG, Brooks G, Zocchi M, et al. (2015) A Randomized Clinical Trial Comparing Use of Rapid Molecular Testing for Staphylococcus aureus for Patients with Cutaneous Abscesses in the Emergency Department With Standard of Care. Infect Control Hosp Epidemiol 36(12): 1423-1430.
-
Talan DA, Lovecchio F, Abrahamian FM, Karras DJ, Steele MT, et al. (2016) A Randomized Trial of Clindamycin Versus Trimethoprim-sulfamethoxazole for Uncomplicated Wound Infection. Clin Infect Dis 62(12): 1505-1513.
-
Diaz R, Afreixo V, Ramalheira E, Rodrigues C, Gago B (2018) Evaluation of vancomycin MIC creep in methicillin-resistant Staphylococcus aureus infections-a systematic review and meta-analysis. Clin Microbiol Infect 24(2): 97-104.
-
Giorgobiani M, Burroughs MH, Antadze T, Carrothers TJ, Riccobene TA, et al. (2023) The Safety and Efficacy of Dalbavancin and Active Comparator in Pediatric Patients With Acute Bacterial Skin and Skin Structure Infections. Pediatr Infect Dis J 42(3): 199-205.
-
Liu F, Rajabi S, Shi C, Afifirad G, Omidi N, et al. (2022) Antibacterial activity of recently approved antibiotics against methicillin-resistant Staphylococcus aureus (MRSA) strains: A systematic review and meta-analysis. Ann Clin Microbiol Antimicrob 21(1): 37.
-
Eggers S, Barker AK, Valentine S, Hess T, Duster M, et al. (2018) Effect of Lactobacillus rhamnosus HN001 on carriage of Staphylococcus aureus: results of the impact of probiotics for reducing infections in veterans (IMPROVE) study. BMC infectious diseases 18(1): 129.
-
Wozniak TM, Barnsbee L, Lee XJ (2019) Using the best available data to estimate the cost of antimicrobial resistance: a systematic review. Antimicrob Resist Infect Control 8: 26.
-
Alegre ML, Chen L, David MZ, Bartman C, Vavra SB, et al. (2016) Impact of Staphylococcus aureus USA300 Colonization and Skin Infections on Systemic Immune Responses in Humans. J Immunol 197(4): 1118-1126.
-
Curdy S, Lawrence L, Quintas M, Woosley L, Flamm R, et al. (2017) In Vitro Activity of Delafloxacin and Microbiological Response against Fluoroquinolone- Susceptible and Nonsusceptible Staphylococcus aureus Isolates from Two Phase 3 Studies of Acute Bacterial Skin and Skin Structure Infections. Antimicrob Agents Chemother 61(9): e00772-e00817.
-
Hayden MK, Lolans K, Haffenreffer K, Avery TR, Kleinman K, et al. (2016) Chlorhexidine and Mupirocin Susceptibility of Methicillin-Resistant Staphylococcus aureus Isolates in the REDUCE-MRSA Trial. J Clin Microbiol 54(11): 2735-2742.
-
Deeny SR, Worby CJ, Auguet OT, Cooper BS, Edgeworth J, et al. (2015) Impact of mupirocin resistance on the transmission and control of healthcare-associated MRSA. J Antimicrob Chemother 70(12): 3366-3378.
-
Emonet S, Charles PG, Harbarth S, Stewardson AJ, Renzi G, et al. (2016) Rapid molecular determination of methicillin resistance in staphylococcal bacteraemia improves early targeted antibiotic prescribing: a randomized clinical trial. Clin Microbiol Infect 22(11): 946.e9-946.e15.
-
Shi C, Ye J, Xu R, Jin W, Xu S, et al. (2021) Effect of the vancomycin minimum inhibitory concentration on clinical outcomes in patients with methicillin-susceptible Staphylococcus aureus bacteraemia: a systematic review and meta-analysis. BMJ Open 11(1): e040675.
-
Ouangraoua SH, Diallo JT, Zongo I, Kabore NF, Nikiema F, et al. (2021) Impact of mass administration of azithromycin as a preventive treatment on the prevalence and resistance of nasopharyngeal carriage of Staphylococcus aureus. PLoS One 16(10): e0257190.
-
Riordan WO, Manus A, Teras J, Poromanski I, Saldariagga MC, et al. (2018) A Comparison of the Efficacy and Safety of Intravenous Followed by Oral Delafloxacin with Vancomycin Plus Aztreonam for the Treatment of Acute Bacterial Skin and Skin Structure Infections: A Phase 3, Multinational, Double-Blind, Randomized Study. Clin Infect Dis 67(5): 657-666.
-
Paul M, Bishara J, Yahav D, Goldberg E, Neuberger A, et al. (2015) Trimethoprim-sulfamethoxazole versus vancomycin for severe infections caused by meticillin resistant Staphylococcus aureus: randomised controlled trial. BMJ 350: h2219.
-
Leangapichart T, Rolain JM, Memish ZA, Al-Tawfiq JA, Gautret P (2017) Emergence of drug resistant bacteria at the Hajj: A systematic review. Travel Med Infect Dis 18: 3-17.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling