Role of Insulin Resistance in Males with Early Androgenetic Alopecia
Early androgentic alopecia (EAA): is an androgen related disorder. It could be a clinical marker of insulin resistance and hyperinsulinaemia in men with EAA
Introduction
Androgenetic alopecia (AGA) is a common hair loss disease with genetic predisposition among men and women, commence at any age after puberty. It may significantly affect a variety of psychological and social aspects of one's life and the individual's overall quality of life [1].
Insulin resistance refers to state where insulin receptors sites on cell walls become unresponsive to the presence of insulin causing inability to move glucose into cells and accumulation of glucose in the blood [2]. Sex hormone-binding globulin (SHBG) is the circulating steroid-binding protein produced by the liver that binds testosterone with high affinity. It is an important regulator of androgen homeostasis and functions as a modulator of androgen delivery to the tissues. SHBG concentration falls during puberty in both boys and girls. Serum SHBG levels are primarily regulated by sex steroids and thyroxin [3]. It has been suggested that the link between total testosterone and insulin resistance is due to the negative relationship between SHBG and insulin [4]. Insulin is an important regulator of SHBG production by the liver [5]. Insulin resistance may also have an effect on scalp circulation causing vasoconstriction of blood capillaries with reduced blood flow and, therefore, worsening of AGA [6]. Subcutaneous blood flow was shown to be reduced in early male pattern baldness when compared with a hair-bearing scalp. Microvascular insufficiency with local tissue hypoxia was also demonstrated in a bald scalp leading to nutritional deficiency in the follicles of the scalp and it enhances the effect of DHT on follicular miniaturization [6]. Smoking harmfully affects the microvasculature of the dermal hair papilla, its geno-toxicants-induce damage to DNA of the hair follicle, imbalance in the follicular protease or antiprotease systems and relative hypoestrogenic state by inducing increased hydroxylation of oestradiol, and inhibition of aromatase [4].
Patients and Methods
Patient
All statistical calculations were done using computer programs. Microsoft excel version 10 and SPSS (statistical package for the social science version 20.00) statistical program. at 0.05 level of probability [8] Comparison of percentage was done using the t stand the One-way ANOVA and Post hoc-LSD tests (the least significant difference)was presented using percentage, mean ±standard deviation. The Pearson linear correlation coefficient was estimated to show the relationship of the physiological parameter to each other [9].
The present study was performed on a total of 30 male patients with early onset of AGA <35 years old aged between 18-50 years old and 30 age matched healthy subjects as a control group. These patients were selected from patients attending the outpatient clinic of Al-Zahraa Hospital and Mansoura Dermatology Hospital in the period between January 2015 and June 2015. Exclusion criteria: we excluded subjects with hypertension (HTN), coronary arterial disease, Apparent obesity, diabetes mellitus, thyroid disease, malignancy, amyloidosis, autoimmune diseases, corticosteroid treatment in both patient and control groups.
Methods
An informed consent was taken before inclusion of the subjects into the study. All patients were subjected to the following: Full history taking: age, onset, course, duration. History of drug intake, smoking, medical disorders, family history of AGA, family history of DM and HTN, Dyslipidemia. We examined all groups to exclude the presence of other dermatologic skin disease, and determine the grading of AGA according to Hamilton– Norwood classification. Measurement of (BMI) and waist circumference, BP, FPG level by Trinder. GOD-POD (glucose oxidase-glucose peroxidase) using SPINREACT (SPINREACT, S.A.u. Santa Coloma, Spain). Normal values are (70-110) mg/dl., blood cholesterol by CHOD-POD. Enzymatic colorimetric using SPINREACT (SPINREACT, SA/S.A.u. Santa Coloma, Spain). Normal values are (150- 220mg/dl) of blood TG:by GPO-POD. Enzymatic colorimetric using SPINREACT (SPINREACT, S.A.u. Santa Coloma, Spain). Normal values are (50-150mg/dl). HDL cholesterol and LDL cholesrerol: CHOD-POD. Enzymatic colorimetric using SPINREACT (SPINREACT, SA/S.A.u. Santa Coloma, Spain). LDL cholesterol levels were measured using Fried Wald formula LDL=Total cholesterol-(HDL+TG/5). Normal values of HDL cholesterol are (45-65mg/dl). Normal values of LDL cholesterol are up to 150 mg/dl, serum Insulin: Insulin Resistance (HOMA-IR): Homeostatic model assessment for insulin resistance (HOMA-IR) was calculated using the updated model [(fasting insulin (mIU/ml) × fasting glucose (mmol/l)/22.5]. And value above 2.5 was considered to indicate IR [7].
Statistical Analysis
Results
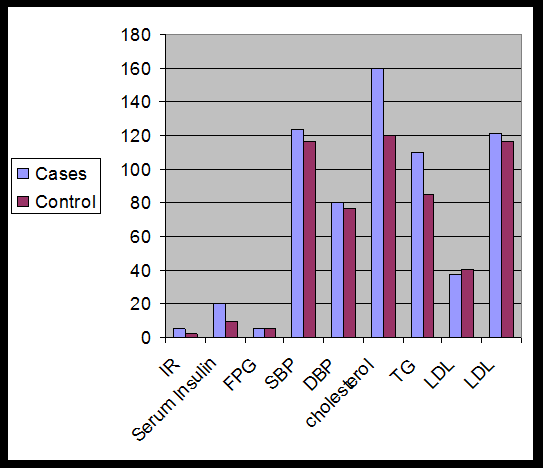
| Control no=30 | Control no=30 | T test | P value | |||||||||
| IR | 5.45 ± 6.37 | 2.75 ± 1.68 | 2.239 | 0.029 | ||||||||
| Serum insulin(mIU/ml) | 22.79±26.43 | 12.39± 7.65 | 2.07 | 0.043 | ||||||||
| FPG(mmol/l) | 5.21± 0.71 | 5.07± 0.66 | 0.764 | 0.448 | ||||||||
| SBP | 125.00± 7.99 | 117.17 ±12.08 | 2.962 | 0.004 | ||||||||
| DBP | 81.33± 7.30 | 77.33 ±9.07 | 1.881 | 0.065 | ||||||||
| Cholesterol(mg/dl) | 185.87± 35.76 | 154.34 ± 31.79 | 3.598 | 0.001 | ||||||||
| TG(mg/dl) | 127.33 ±50.56 | 100.50± 26.79 | 2.568 | 0.013 | ||||||||
| HDL(mg/dl) | 38.17± 13.34 | 41.33±13.89 | -0.901 | 0.371 | ||||||||
| LDL (mg/dl) | 122.23 ± 32.88 | 117.13± 29.25 | 0.635 | 0.528 |
Table 1: Comparison of IR, serum insulin, FPG, BP, lipid profile, BMI, waist circumference between patient and control Table 1: C
| Grading of androgenetic | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 5 | 6 | F ratio | P value | |||||||||||||||||
| alopecia | |||||||||||||||||||||||
| IR | 1.36 ± 0.93 | 2.32 ± 0.95 A | 4.13±0.92 A | 10.42 ±7.74 b | 14.12±12.60 b | 5.372 | 0.003 * |
Table 2: Comparison of IR in relation to different grades of AGA.
| IR | Age≤ 35 | Age >35 | T test | P value | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| patient group | 2.48±1.34 | 8.04± 7.84 | 2.615 | 0.014 | ||||||||||
| control group | 2.57±1.81 | 3.07±1.47 | 0.744 | 0.463 |
Table 3: Comparison of IR in different age group of cases and control (<35, >35) ys old.
| Duration | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T test | P value | |||||||||
| <10(years) | >10(years) | |||||||||
| IR | 4.99±7.30 | 5.68± 5.68 | 0.274 | 0.786 |
Table 4: Comparison of IR as regards the duration of AGA (<10, >10 years) Table 4: Comparison of IR as regards the duration of AG
| IR | Smokers | Non smokers | T test | P value | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| patients | 2.20±0.96 | 7.93± 7.59 | 2.694 | 0.012 | ||||||||||
| control | 1.54±0.48 | 3.97± 1.69 | 4.398 | 0 |
Table 5: Comparison of IR as regards smoking in patients and control group.
There was significant increase in IR in smokers in both cases and control groups.
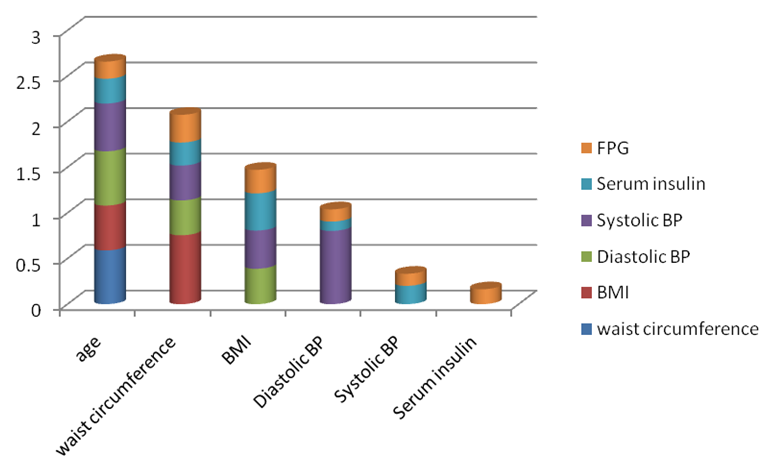
• Systolic blood pressure is strongly positive correlated with diastolic blood pressure and positively correlated with age and BMI, while weakly correlated with waist circumference, Serum insulin and FPG.
• Serum insulin is positively correlated with BMI and weakly correlated with all parameters.
• FBG is positively correlated with waist circumference and weakly correlated with all parameters.
| -family history of AGA | +ve family history of AGA | T test | P value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| IR | 6.64±5.69 | 5.26± 6.55 | 0.398 | 0.694 NS |
Table 6: Comparison of IR in patients with +ve and -ve family history of androgenetic alopecia in patients group.
There was no statistically significant difference in IR between patient with +ve & -ve family history of AGA.
Discussion
(AGA) is an androgen related disorder that is characterised by hair loss in genetically predisposed persons [10]. Dihydrotestosterone (DHT) binds to the androgenic receptor on the pilous follicle of the scalp that triggers genes responsible for gradual transformation of the large terminal follicles to villous ones. This process is more prominent in the fronto-temporal area and vertex in men, and over the crown in women [11]. Insulin resistance (IR) is defined as an impaired biological response to exogenous or endogenous insulin, which suppress glucose production and transport [12].
This study was conducted to evaluate the role of insulin resistance with EAA. A total number of 30 male patients their ages ranged from 18 to 50 with early onset of AGA <35 years old and 30 healthy subjects aged between (18- 50) years old were enrolled in this study. Regarding IR, we found that Patient group had statistically significant increase in insulin resistance than control group (P value <0.05). This could be explained that subcutaneous blood flow was shown to be reduced in early male pattern baldness when compared with hair- bearing scalp, IR causes microvascular insufficiency and local tissue hypoxia leading to nutritional deficiency in the follicles of the scalp and it enhances the effect of DHT on follicular miniaturization [6]. Our result coincided with Matilinian et al. who had shown that hyperinsulinaemia is significantly higher among men with early AGA. In their study, cases with ≥ 3 stage AGA and early-onset AGA (<35 years) according to the Norwood–Hamilton scale were chosen among 19 to
50 year old males. It was observed that alopecia cases had risk factors associated with IR compared with patients without alopecia, and that hyperinsulinemia was two-fold more frequent in alopecia cases [13]. Also our result agreed with (Hirrso et al) who investigated insulin sensitivity in 55-year-old AGA males using the QUICKI; they demonstrated a reduction in insulin sensitivity in the AGA group [14]. Also our result coincided with Ekmekçi et al. who conducted a partially similar study with 66 female participants, and compared IR and insulin sensitivity indices in 41 women with AGA against 25 healthy, non- obese women. Their results showed that IR is more common among women with AGA [12]. Also our result was consistent with González et al. who found that a relationship exists between IR and early baldness. Their study included 80 participants with AGA and 80 controls that were age- and weight-matched. Both groups comprised obese and non-obese cases. The Homeostatic model assessment for insulin resistance (HOMA-IR index) [fasting insulin (mIU/ml) × (fasting glucose (mmol/l)/22.5] was found to be significantly higher among both obese and non-obese participants with AGA compared to the Control, which is similar to the findings of the current study [15]. Regarding serum insulin level, we found statistically significant increase in serum insulin levels in androgenetic alopecia group than control group and so, our study assured that hyperinsulinemia play a role in male with early androgenetic alopecia. This can be clarified by positive correlation between testosterone levels and insulin sensitivity in men. It has been suggested that the link between total testosterone and insulin resistance is due to the negative relationship between steroid-binding protein (SHBG) and insulin. Lower SHBG levels in male with AGA may be a marker for hyperinsulinaemia and IR. This result was consistent with (Acibucu et al) who found higher levels of insulin in case group than in the control group, but the difference was not statistically significant [16]. Regarding lipid profile (blood cholesterol, blood triglycerides, HDL cholesterol and LDL cholesterol). We found higher levels of blood cholesterol and Triglycerides and LDL cholesterol in AGA group than in control group while there was a decrease in HDL but there was no statistically meaningful difference in the LDL and HDL values. And so, our study confirmed that there is a strong relationship between male with EAA and dyslipidemia. Tall explained this by the action of androgen on lowering HDL and increasing cholesterol and triglyceride levels in male with androgenetic alopecia [17]. The result coincided with (Şaşmaz et al) who compared the serum total cholesterol, HDL, LDL, TG and lipoprotein A levels in 41 male vertex type AGA patients and 36 controls with normal hair texture. They found significantly higher levels of serum TG and lipoprotein A in the AGA group, and higher total cholesterol and LDL cholesterol levels but not statistically significant [18]. The result was against (Guzzo et al) who compared the serum lipid profile of 50 Hamilton III and IV vertex alopecia patients with a control group, and found no difference in HDL, LDL, total cholesterol, TG and total cholesterol/LDL rates [19]. In our study we found that FPG level is higher in patients group than control group but this was not statistically significant. This can be explained by impaired glucose tolerance in patients who are resistant to the action of insulin leading to hyperglycaemia. Our result coincided with (Nabaie et al) who could not demonstrate a significant difference between AGA cases and control group [20]. We graded androgenetic alopecia and found statistically significant correlation between IR and grades of AGA. Our result was against (Acibucu et al) who showed that the difference was not found to be statistically meaningful [16]. We found statistically significant difference of SBP between AGA group and control group. Systolic blood pressure was higher in AGA group than control group and the average diastolic blood pressure was determined to be higher in the AGA group. This could be explained by those androgens which bind to mineralocorticoid receptors might be responsible for the observed difference in blood pressure and for instance may participate in the higher susceptibility to hypertension in men [21]. This result agreed with (Arias et al) who found that the mean systolic blood pressure values were higher in patients with AGA than in control subjects. There are androgen mediated receptors accelerating the atherosclerotic process in the vascular endothelium. Androgens can accelerate atherosclerosis by proliferation of smooth muscle cells in vessels [22]. IR was higher in smokers group than non-smokers group in both groups. Smoking increases the risk of IR through decreasing insulin sensitivity. Smoking has harmful effect on the micro vasculature of the dermal hair papilla by which smoking influences AGA [4]. Our result coincided with Eliasson et al. who showed that smoking cessation improves insulin sensitivity in healthy middle-aged men forty male, non-obese healthysmokers participated in this open parallel study with 8 weeks of follow-up [23]. We also found high statistically significant relation of waist circumference and BMI in AGA group in comparison with control group. BMI had positive associations with indices of IR in male with EAA. This result coincided with Acibucu et al. who did a study in two groups compared with respect to waist circumference. Waist circumferences in patient group were found to be higher than those in control group [17]. This result did not agree with Ceyda et al. who observed no statistically significant difference between the AGA and control groups with respect BMI, and waist circumference [24]. In our study we found that IR increases with group age above 35 years old. This can be explained by impaired insulin metabolism associated with age (biological aging) leading to decrease in both insulin secretion and insulin sensitivity. Thus, insulin resistance is increased. Our result coincided with (Ele Ferrannini et al) who analyzed euglycemic insulin clamp (1mU
- min"1
- kg"1) data collected at 20 centers throughout Europe from 1,146 men and women with normal glucose tolerance, ranging in age from 18 to 85 years. In the whole group, insulin action (as the M value) declined slightly with age (at a rate of 0.9 junol
- min"1
- kg"1 per decade of life, 95% CI = 0.4-1.3, P = 0.0002) [25, 26].
Conclusions and Recommendations
According to the present results, we conclude that (AGA) is an androgen related disorder that may be associated with IR, dyslipidemia and hypertension.
Male with EAA should be screened for IR, dyslipidemia andhypertensionas. EAA could be a clinical marker for these disorders. However large prospective studies are recommended.
References
-
Han SH, Byun JW, Lee WS, Kang H, Kye YC, et al. (2012) Quality of life assessment in male patients with androgenetic alopecia: result of a prospective, multicenter study. Ann Dermatol 24(3): 311-318.
-
Jake Paul Fratkin (2012) Understanding insulin resistance. Oregon Association of Acupuncture and Oriental Medicine pp. 1-12.
-
Kapoor D, Malkin CJ, Channer KS, Jones TH (2005) Androgens, insulin resistance and vascular disease in men. Clinical Endocrinology 63(3): 239-250.
-
Severi G, Sinclair R, Hopper JL, English DR, McCredie MR, et al. (2003) Androgenetic alopecia in men aged 40–69 years: prevalence and risk factors. Br J Dermatol 149(6): 1207-1213.
-
Tsai EC, Matsumoto AM, Fujimoto WY, Boyko EJ (2004) Association of bioavailable, free, and total testosterone with insulin resistance: influence of sex hormone–binding globulin and body fat. Diabetes Care 27(4): 861-868.
-
Chen W, Thiboutot D, Zouboulis C (2002) Cutaneous androgen metabolism: basic research and clinical perspectives. J Invest Dermatol 119(5): 992-1007.
-
Rossner SM, Neovius M, Mattsson A, Marcus C, Norgren S (2010) HOMA-IR and QUICKI: decide on a general standard instead of making further comparisons. Acta Paediatr 99(11): 1735-1740.
-
Snedecor GW, Cochran WG (1980) Statistical Methods. (7th Edn), Ames: Iowa State University Press.
-
Härdle W, Simar L (2007) Applied Multivariate Statistical Analysis. (2nd Edn), Springer, pp. 420.
-
Zouboulis CC, Chen WC, Thornton MJ, Qin K, Rosenfield R (2007) Sexual hormones in human skin. Hormone and Metabolic Research 39(2): 85-95.
-
Hanneken S, Ritzmann S, Nöthen MM, Kruse R (2003) Androgenetic alopecia. Current aspects of a common phenotype. Hautarzt 54(8): 703-712.
-
Ekmekçi TR, Ucak S, Basat O, Koslu A, Altuntas Y (2009) The presence of insulin resistance and comparison of various insulin sensitivity indices in women with androgenetic alopecia. Eur J Dermatol 17(1): 21-25.
-
Matilainen V, Koskela P, Keinänen-Kiukaanniemi S (2000) Early androgenetic alopecia as a marker of insulin resistance. Lancet 356(9236): 1165-1166.
-
Hirsso P, Laakso M, Matilainen V, Hiltunen L, Rajala U, et al. (2006) Association of insulin resistance linked disease and hair loss in elderly men. Finnish population based study. Cent Eur J Public Health 14(2): 78-81.
-
González-González JG, Mancillas-Adame LG, Fernández-Reyes M, Gómez-Flores M, Lavalle- González FJ, et al. (2009) Androgenetic alopecia and insulin resistance in young men. Clin Endocrinol 71(4): 494-499.
-
Acibucu F, Kayatas M, Candan F (2010) The association of insulin resistance and metabolic syndrome in early androgenetic alopecia. Singapore Med J 51(12): 931-936.
-
Tall AR (2007) CETP inhibitors to increase HDL cholesterol levels. N Engl J Med 356(13): 1364-1366.
-
Sasmaz S, Senol M, Ozcan A, Dogan G, Tuncer C, et al. (1999) The risk of coronary heart disease in men with androgenetic alopecia. J Eur Acad Dermatol Venereol 12(2): 123-125.
-
Guzzo CA, Margolis DJ, Johnson J (1996) Lipid profiles, alopecia, and coronary disease: any relationship? Dermatol Surg 22(5): 481.
-
Nabaie L, Kavand S, Robati RM, Sarrafi-Rad N, Shahgholi L, et al. (2009) Androgenic alopecia and insulin resistance: are they really related?. Clin Exp Dermatol 34(6): 694-697.
-
Quinkler M, Diederich S, Bahr V, Oelkers W (2004) The role of progesterone metabolism and androgen synthesis in renal blood pressure regulation. Horm Metab Res 36(6): 381-386.
-
Arias-Santiago S, Gutiérrez-Salmeron MT, Castellote- Caballero L, Buendia-Eisman A, Naranjo-Sintes R (2010) Androgenetic alopecia and cardiovascular risk factors in men and women: a comparative study. J Am Acad Dermatol 63(3): 420-429.
-
Eliasson B, Attvall S, Taskinen MR, Smith U (1997) Smoking cessation improves insulin sensitivity in healthy middle-aged men. Eur J Clin Invest 27(5): 450-456.
-
Mumcuoglu C, Ekmekci TR, Ucak S (2011) The investigation of insulin resistance and metabolic syndrome in male patients with early-onset androgenetic alopecia. Eur J Dermatol 21(1): 79-82.
-
Ferrannini E, Vichi S, Beck-Nielsen H, Laakso M, Paolisso G, et al. (1996) Insulin Action and Age. European Group for the Study of Insulin Resistance (EGIR). Diabetes 45(7): 947-953.
-
Norwood OT (1975) Male pattern baldness Classification and incidence. South Med J 68(11): 1359-1365.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling