Apocrine Carcinoma of Breast -Uncommon Variant of Breast Malignancy
Apocrine carcinoma of breast is an extremely uncommon, special variant of breast malignancy with an incidence of <1%. A case of 70 year female presented with large right breast mass with extensive skin ulcerations and right axillary lymphadenopathy of 4 months. On sonomamography of Breast Imaging Reporting and Data System showed irregular heterogeneous echotexture mass (BI-RADS) IV. On fine niddle aspiration cytology reported as positive for carcinoma cells. Patient underwent modified radical mastectomy. On histopathology diagnosed as invasive apocrine carcinoma type A, of right breast. The tumor grading by Modified Richardson- Bloom criteria- it was (2+3+2) grade II. Right axillary lymph nodes 18 were involved by the tumor. The immunohistochemistry study showed ER, PR, Her 2 neu negative. The neo-adjuvant therapy was given. On follow-up of 8 months satisfactory healing and no recurrence was noted. Conclusion: Apocrine carcinoma has better prognosis than invasive breast carcinoma (NOS). These are characteristic triple negative breast cancer. We are presenting this case for its rarity, clinical behavior, histomorphological, immunohistochemical features.
Introduction
Apocrine carcinoma of breast is a extremely uncommon, special variant of breast malignancy with an incidence of <1% of all invasive cancer in women [1]. To dignose pure primary apocrine can of breast requires > 90% of tumor cells have cytologic or immunohistochemical features of apocrine cells [2]. There is lack of uniform application of diagnostic criteria for definitions of apocrine carcinoma in the literature. The most recent WHO classification of breast tumors offers an imprecise definition of apocrine carcinoma of the breast [3].
A case of 70 year female presented with large right breast mass with extensive skin ulcerations and right axillary lymphadenopathy of 6 months duration. There was no any significant history of hormonal use, trauma, any medication or previous surgical intervention. Other left side breast was normal. There were no any other significant findings on systemic examination. On sonomamography of Breast Imaging Reporting and Data System of right breast showed irregular heterogeneous echotexture mass (BI-RADS) IV. The mass measuring 4.5x3x2.5 cm. Patient’s therapeutic intervention was right sided modified radical mastectomy. On gross examination of specimen (figures 1 & 2).
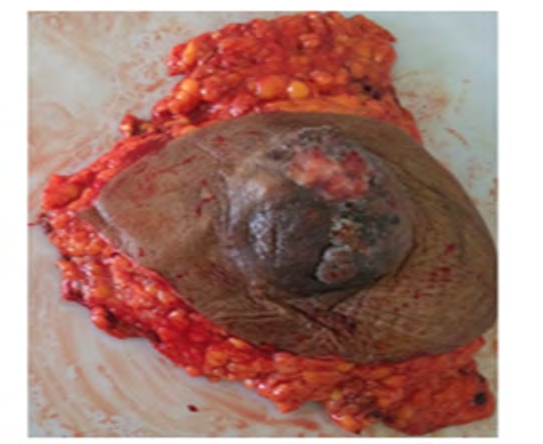
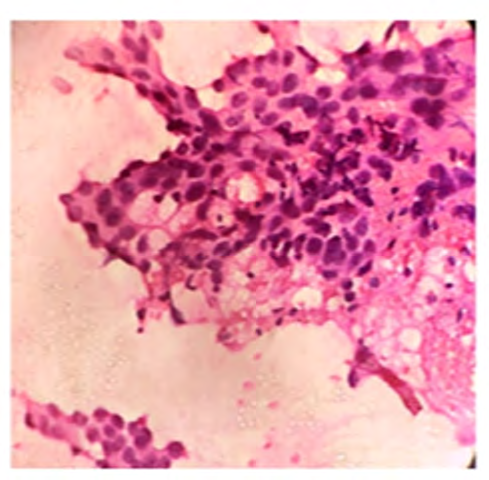
Right breast showed mass measuring 4.8x3.5x2.5cm. On cut section showed grey, white, firm, solid, irregular tumor situated subarolar reagion. Overlying skin showed ulceration and nipple areola dystruction. On fine needle aspiration cytology reported as positive for carcinoma cells (figure 3).

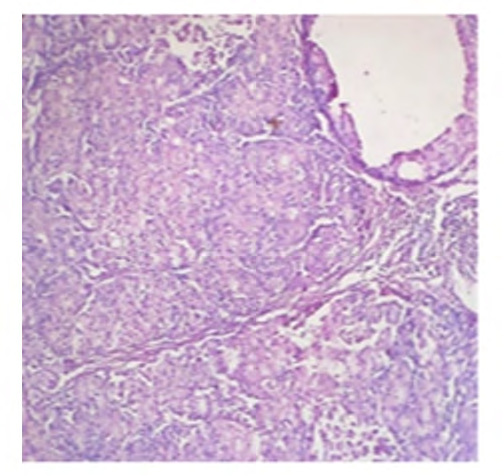
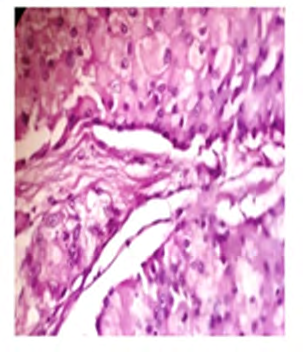
On microscopy showed the tumor of 90% microscopic fields showed features of large tumor cells with sharply defined cell borders .The cell with abundant eosinophilic cytoplasm of granular type, the nucleus to cytoplasm ratio of 1:2. The nuclei are round, large and vesicular and moderately pleomorphic. On histopathology diagnosed as invasive apocrine carcinoma type A- right breast (figures 4 & 5).
The tumor grading by Modified Richardson- Bloom criteria- it was (2+3+2) grade II. Right axillary lymph nodes 18 were involved by the tumor. Adjacent breast tissue showed areas of apocrine adenosis, inflammation. The immunohistochemistry of breast was ER, PR, and Her2 neu negative (figures 6-8).
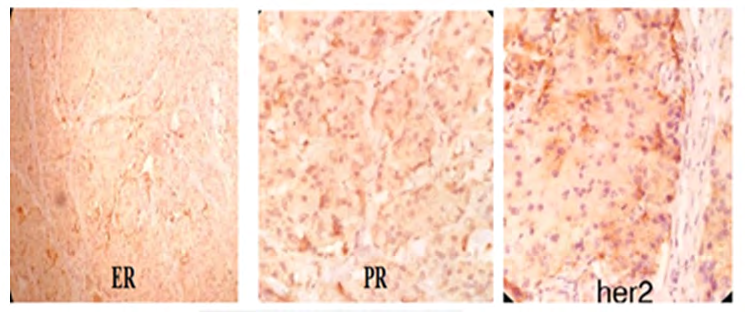
Figure 6,7 and 8: IHC Study showing triple-negative breast cancer for ER, PR, and Her 2 neu.
The neo-adjuvant therapy was given. On follow-up of 8 months satisfactory healing and no recurrence was noted.
Discussion
The breast apocrine carcinoma is a rare, unique, and morphologically distinctive type of invasive ductal carcinoma. It constituting between 0.3 and 4% of all invasive cancer in women [4]. The average age of the patients with invasive apocrine carcinoma is 48-60 years [5]. Apocrine carcinomas clinically present with palpable lump in breast, rarely with nipple bloody discharge or as a cyst [3, 6]. In our case patient was reported in advance disease course with large breast mass involving skin and ulceration. Apocrine carcinomas tend to be unilateral. It may be noted as multicentric lesions. Japaze has proposed the criteria to dignose apocine carcinoma are in the tumor at least 75% of microscopic fields must show features of large tumor cells with sharply defined cell borders. The cell with abundant eosinophilic cytoplasm of usually granular type, the nucleus to cytoplasm ratio of 1:2 or more, the nuclei are round, large and vesicular or may be pleomorphic [7].
In our case on morphology showed round neoplastic tumor cells having distinct cell margins with abundant eosinophilic and granular cytoplasm, centrally to eccentrically located nuclei with prominent nucleoli and distinctive cell borders. (Figure 4&5). There are two types of cell types of apocrine carcinoma of the breast has been described type A and type B. In type a cell are having abundant granular and intensely eosinophilic cytoplasm and in type B cell are having abundant vacuolated or foamy cytoplasm [8]. In our case it is of type a cells. The granules in type a are PAS+ diastase resistant. Apocrine differentiation can be seen in other breast carcinoma subtypes mainly medullary and pleomorphic lobular carcinoma [9]. The other conditions for differential diagnosis are secretory carcinoma, oncocytic carcinoma, lipid rich carcinoma. Some benign conditions like apocrine metaplasia, histiocytic proliferation should be properly look for.
Apocrine epithelium has the characteristic negative for estrogen receptor-alpha (ER), progesterone receptor (PR), Her-2 neu and is positive to steroid receptor- androgen receptor (AR) [10]. Many study showed that specific apocrine marker is GCDFP-15+, however, GCDFP-15 protein expression appears to be reduced in advanced apocrine carcinomas. Apocrine carcinomas has better prognosis than invasive breast carcinoma (NOS) as there seems to be a potential unique response to androgen (fluoxymesterone) administration as a part of treatment. In males very rarely apocrine carcinoma brest were noted, the most common histological types of male breast cancer are IBC of no specific type (90%), followed by invasive papillary and medullary carcinomas of the breast [11].
New approach to androgen receptor as a targeted therapy for breast cancer will be helpful for patients [12]. Triple-negative apocrine carcinoma (TNAC) of the breast is had a better prognosis than patients with TNBC, and chemotherapy was associated with survival advantages in TNAC patients [13]. Most of apocrine breast carcinomas were immunohistochemically-positive for androgen receptor (AR). Anti-androgenic therapies can potentially serve as a cancer- targeting therapy for apocrine breast carcinoma. In our case positive for androgen receptor (AR) and the neo-adjuvant therapy was given. On follow-up of 9 months satisfactory healing and no recurrence was noted.
Conclusion
Apocrine carcinoma is a rare and distinct morphological type of invasive breast cancer. It has better prognosis than invasive breast carcinoma. We are presenting this case for its rarity, clinical behaviour, histomorphological, immunohistochemical features.
References
-
Gayatri BG, Mondita B, Asha B, Vishal A (2012) Study on apocrine carcinoma of breast: histomorphologic features and immunohistochemical behavior. International Journal of Basic and Applied Medical Sciences 2(3): 190- 193.
-
O’Malley FP, Pinder SE, Muligan AM (2011) Breast Pathology, 2nd (Edn.), Saunders Elsevier.
-
Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ (2012) WHO classification of tumours of the breast, 4th(Edn.), IARC, Lyon.
-
Dellapasqua S, Maisonneuve P, Viale G, Pruneri G, Mazzarol G, et al. (2013) Immunohistochemically Defined Subtypes and Outcome of Apocrine Breast Cancer. Clin Breast Cancer 13(2): 95-102.
-
Tanaka K, Imoto S, Wada N, Sakemura N, Hasebe K (2008) Invasive apocrine carcinoma of the breast: clinicopathologic features of 57 patients. Breast J 14(2): 164-168.
-
Mardi K, Sharma J, Sharma N (2004) Apocrine carcinoma of the breast presenting as a solitary cyst: cytological and histopathological study of a case. Indian J Pathol Microbiol 47(2): 268-270.
-
Japaze H, Emina J, Diaz C, Schwam RJ, Gercovich N (2005) Pure invasive apocrine carcinoma of the breast: a new clinicopathological entity. Breast 14(1): 3-10.
-
Eusebi V, Millis RR, Cattani MG, Bussolati G, Azzopardi JG (1986) A morphologic and immunocytochemical study. Am J Pathol 123(3): 532-541.
-
Jagtap SV, Beniwal A, Shah HP, Bhosale SJ, Chougale PG, et al. (2016) medullary carcinoma of breast: Clinicopathological study. J Evid Based Med Health 3: 2256-2260.
-
Mills AM, Gottlieb CE, Wendroth SM, Brenin CM, Atkins KA (2016) pure apocrine carcinomas represent a clinicopathologically distinct androgen receptor- positive subset of triple-negative breast cancers. Am J Surg Pathol 40(8): 1109-1116.
-
Jagtap SV, Chougule PG, Khatib W, Shukla DB (2014) Male breast cancer: presenting as synchronous, large, bilateral masses. J Clin Diagn Res 8(4): FD07-FD08.
-
Garay JP, Park BH (2016) Androgen receptor as a targeted therapy for breast cancer. Am J Cancer Res 2(4): 434-445.
-
Wu W, Wu M, Peng G, Shi D, Zhang J (2019) Prognosis in triple-negative apocrine carcinomas of the breast: A population-based study. Cancer Med 8(18): 7523-7531.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet