An Extremely Rare Case of Primary Ovarian Teratoid Carcinosarcoma: Cytological, Pathological and Immunohistochemical Findings
An ovarian teratoid carcinosarcoma transformed from mature cystic teratoma, closely resembling its nasopharyngeal one, and occurs in advanced clinical stages, and behaves in a highly aggressive manner. An extremely rare case of primary ovarian teratoid carcinosarcoma is reported with cytological, pathological and immunohistochemical findings. A 49-year-old woman presented to our hospital, complaining of prolonged menstruation. Enhanced computed tomography showed ovarian mature cystic teratomas, however rt-ovarian tumor had invaded to the surface of the rectum, suggesting malignant transformation, and adenomyosis was also suspected. Optimal surgery could be performed. The imprint and ascitic cytology specimens revealed two different patterns of atypical cells suggestive of adenocarcinoma and pleomorphic sarcoma. Pathological findings of the small part of the right ovary revealed adenocarcinoma and pleomorphic sarcoma, immunohistochemically, positive for AE1/ AE3, vimentin and Pax-8, and negative for desmin for the both above components. Her genomic instability score was 73, showing homologous recombination deficiency (HRD) positive showing positive, but tumor BRCA1/2 mutations showed no clinically significant mutations. Thus, final diagnosis was primary rt-ovarian teratoid carcinosarcoma, pT3CN1M0, optimal surgical state, HRD positive and BRCA1/2 no mutations. The patient received the six courses of the chemotherapy with ifosfamide and cisplatin. And niraparib, a PARP inhibitor, monotherapy started. The patient was free from tumor recurrence twelve months after the first visit.
Introduction
Mature cystic teratoma is a common ovarian germ cell tumor comprising 30-45% of all ovarian tumors, which occurs during reproductive age [1]. Malignant transformation occurs in under 2% of mature cystic teratoma [2]. There are various histological types of malignant transformation such as squamous cell carcinoma (SCC), adenocarcinoma, sarcoma, malignant melanoma and mixed histology [3]. Meanwhile, teratoid carcinosarcoma (CS) was first reported in the nasopharynx and ovarian teratoid CS transformed from mature cystic teratoma, described in 1989 [4, 5], closely resembling its nasopharyngeal one. All reported cases of ovarian teratoid CS occurred in advanced clinical stages, and behaved in a highly aggressive manner [6, 7]. Most of malignant transformation cases arising in mature cystic teratoma have been reported to be of SCC and that the mutation of p53 might be one of the genetic events in the malignant transformation of a mature cystic teratoma [8]. To our knowledge, seven ovarian teratoid CSs have been reported in the literature [6, 7]. We herein present an extremely rare case of ovarian teratoid CS with cytological, histological and immunohistochemical findings, and in addition successful treatment of surgery and chemotherapy with ifosfamide and cisplatin, and niraparib.
Case Report
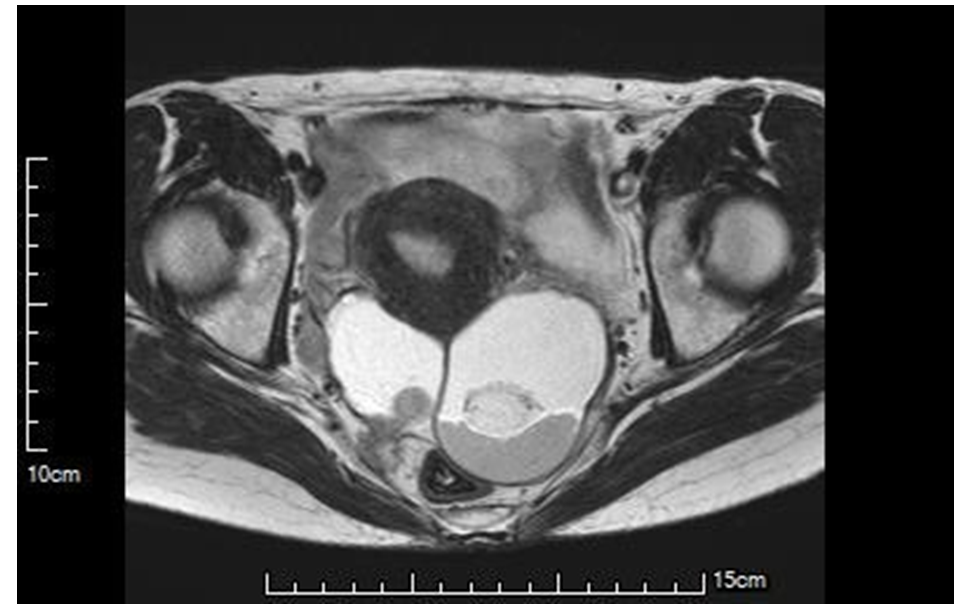
A 49-year-old female, gravida two para two, presented to Gujo City Hospital because of prolonged menstruation. Bilateral cystic tumors were detected on pelvic ultrasound examination. Enhanced computed tomography (CT) showed two pelvic masses, measuring 6.9 x 6.2 cm in her left and 5.0 x 4.2 cm in her right adnexa, suggesting ovarian mature cystic teratomas, however rt-ovarian tumor had invaded toward the back side, suggesting malignant transformation and adenomyosis was also suspected (Figure 1). Hypermenorrhea induced a severe iron deficient anemia (Hb 6.7 g/dl). No other lesions could not be detected except for benign multi-cystic lesions in the mammas by whole body CT. Other laboratory data, including LDH [152 (119-229) IU/L] showed within normal ranges. Tumor markers were as follows: CA125 10.6 (~35) U/ml, CA19-9
47.8 (~37) U/ml, SCC 1.0 (~2.5) ng/ml and CEA 1.6 (~5.0) ng/ml. Red blood cell transfusions were performed for an early surgery. CIN2 was also detected before surgery by biopsies due to uterine cervical smear showing low-grade intraepithelial lesion. Four weeks after her first visit to our hospital, the patient underwent an exploratory laparotomy, under working diagnosis of rt-ovarian malignant tumor, highly suspected of malignant transformation from mature cystic teratoma. At the laparotomy, the bilateral ovaries were enlarged and almost replaced by the tumor, but not ruptured. Some ascites was incubated and submitted to the cytological examination. Bilateral salpingo-oophorectomies were performed by releasing the adhesion without perforations. Rt-ovarian tumor had invaded to the serous side of her rectum. The invaded lesion was released by gastroenterological surgeons without rupture of the rectum. Following, an abdominal hysterectomy, pelvic lymphadenectomy, and partial omentectomy and leaving the serous side of the rectum were performed. Optimal tumor-reductive surgery could be performed. We therefore indwelled subcutaneous reservoir for an intra-pelvic chemotherapy. Macroscopically, bilateral ovaries appeared “mature cystic teratoma”, but right ovary had a ridged part (2.2 x 1.4 cm, arrow in Figure 2). On the imprint and ascitic cytology specimens, two different patterns of atypical cells suggestive of adenocarcinoma showing glandular formation (Figure 3A) and pleomorphic atypical ones suggesting sarcoma were recognized (Figure 3B).
Pathological findings of the protrusion part of the inside of the right ovary revealed adenocarcinoma and pleomorphic sarcoma (Figure 4A, 4B). Immunohistochemically, AE1/AE3, (Figure 4C), vimentin and Pax-8, (Figure 4D) were positive, and desmin and P40 were negative for the both above two components. Thus, the pleomorphic sarcoma component revealed epithelial marker positive one. Also, pathological findings of the left and except for the protrusion part of the right ovary showed mature cystic teratoma, including well- differentiated squamous and bronchial epithelia, bone, fat tissue, and ganglioneuroma as a heterogenous component in the right ovary was recognized (Figure 5A). The ganglioneuroma-like part showed positive reaction for S100 and CD56 (Figure 5B and 5C). Immature teratoma and SCC lesions could not be found in bilateral ovaries. Metastases in the rt-obstructive lymph nodes were also detected, but other disseminations in the pelvic and abdominal cavities nor omentum. CIN2 of the uterine cervix and adenomyosis were also detected.

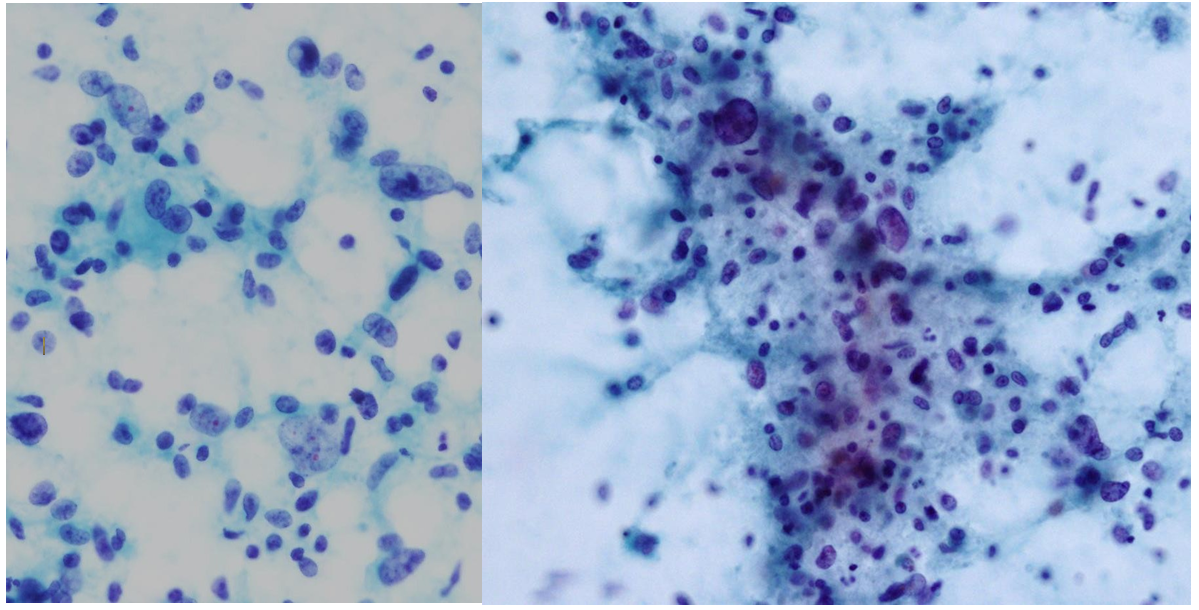
(A) (B) Figure 3: A) Cell clusters consisted of neoplastic cells with dense and hyperchromatic nuclei are observed. Glandular patterns are also noted, suggesting adenocarcinoma (Papanicolaou stain, x 80). B) Scattered neoplastic cells in various size were prominent. Highly dense and hyperchromatic nuclei are observed, suggesting sarcomas (x 80).
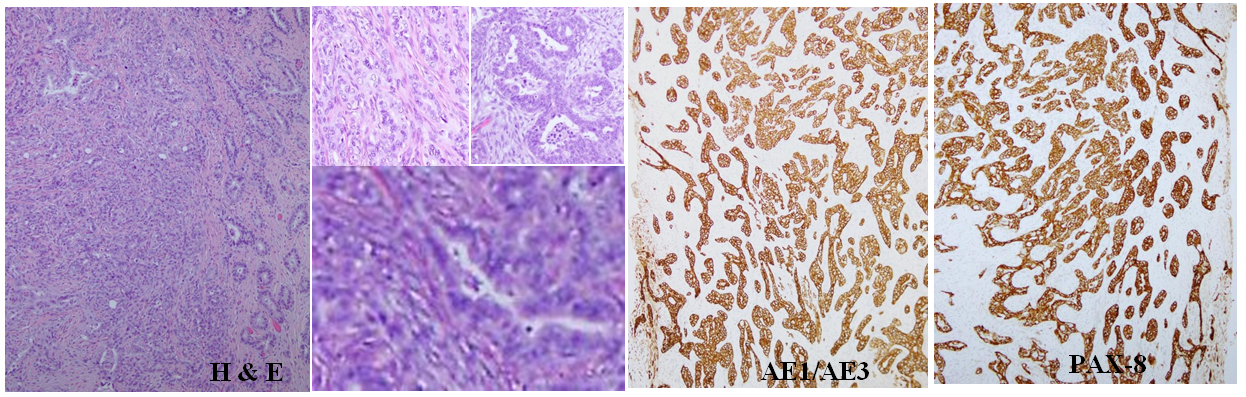
(A) (B) (C) (D) Figure 4: A) Photomicrograph of the ridged part in the right ovary (H&E stain, x 50). The left two-thirds showed pleomorphic sarcoma and the right one-thirds revealed adenocarcinoma. B) Left upper showed pleomorphic sarcoma (H&E stain, x 100). Right upper showed adenocarcinoma (H&E stain, x 100). Under showed intermixing of the two components (H&E stain, x 400. C) Immunohistochemical stainings with AE1/AE3 were positive in the both sarcomatous and adenocarcinoma elements (sABC stain, x 50). D) Immunohistochemical stainings with Pax-8 were also positive for the both sarcomatous and adenocarcinoma elements (sABC stain, x 50).
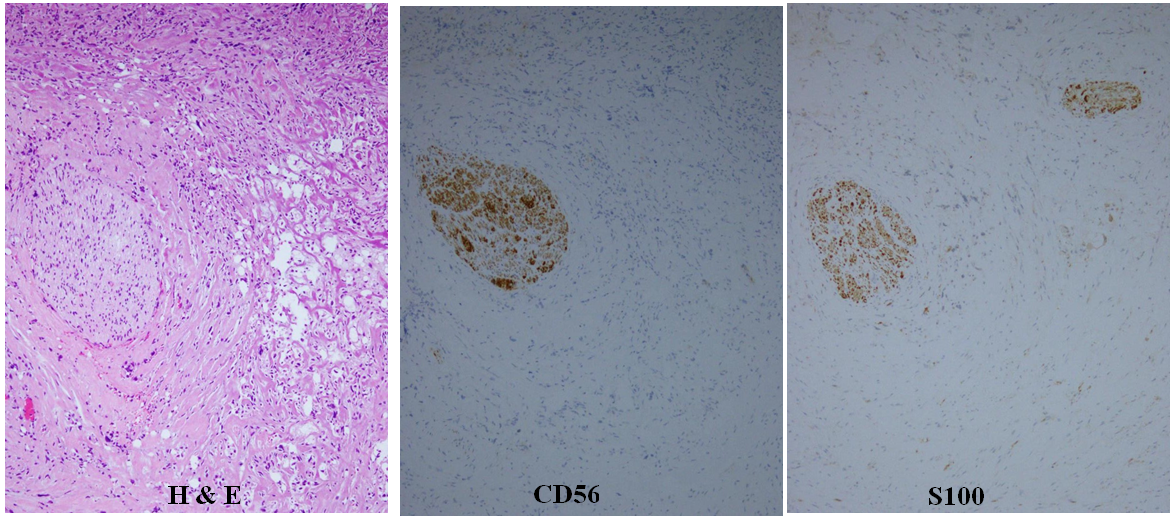
(A) (B) (C) Figure 5: A) A part of the right ovary showed ganglio-neurinoma (H&E stain, x 50). Ganglioma and neurinoma are present, but malignant findings are not recognized. B) Immunohistochemical stainings with CD56 is positive in the neurinomatous part (sABC stain, x 50). C) Immunohistochemical stainings with S100 is also positive in the neurinomatous and some of gangliomatous parts (sABC stain, x 50).
We next determined homologous recombination deficiency (HRD) and tumor BRCA1/2 mutations by Myriad myChoice system® (Myriad Genetic Laboratories, Inc) [9]. Her genomic instability score was 73 (~41), showing HRD positive, but tumor BRCA1/2 mutations showed no clinically significant mutations. From the above results, niraparib, a [poly (ADP-ribose) polymerase)] (PARP) inhibitor is an effective candidate for this patient [10], and will be administered.
Thus, final diagnosis was rt-ovarian primary teratoid carcinosarcoma, pT3CN1M0, optimal surgical state, HRD positive and BRCA1/2 no mutations. CIN2 and adenomyosis were also detected. The patient showed uneventful clinical course after the operation. Three weeks after the operation, she was administered six courses of the chemotherapy with ifosfamide (1.5 g/m2, Day 1, 2 and 4) and cisplatin (15 mg/m2, Day 1, 2 and 4, intra-peritoneal administration through the reservoir) [11, 12, 13]. After the above ifosfamide and cisplatin (IP) chemotherapy, niraparib, a PARP inhibitor, monotherapy started, and will be administered for two years. The patient was free from tumor recurrence twelve months after the first visit.
Discussion
We herein report an extremely rare case of ovarian teratoid CS, only under ten cases have been reported in the literature, and all reported cases of ovarian teratoid CS occurred in advanced clinical stages, and behaved in a highly aggressive manner [6, 7]. This case has not shown the recurrent signs up to date. Most reported cases had immature part of the CS tumor [6, 7], whereas this case had no immature one. Also, all reported cases were advanced stages complaint of symptoms caused by tumors, whereas the present case had prolonged menstruation probably due to adenomyosis, and had no symptoms caused by tumor. Fortunately, the exact CS part was small and it might have a short time after malignant transformation arising from the mature cystic teratoma.
SCC, which arises from the ectoderm, accounts for 80% of malignant transformations of ovarian mature cystic teratoma [2, 3]. Other reported types of the malignant transformation include basal cell carcinoma, melanoma, adenocarcinoma, thyroid carcinoma and carcinoid [2, 3]. In this case, the epithelial elements showed morphologically adenocarcinoma, different from SCC. Also, P40, commonly showing positive for SCC [14], revealed negative for the epithelial elements. Thus, the epithelial element was diagnosed as adenocarcinoma. In this case, the sarcoma element immunohistochemically showed same pattern with adenocarcinoma, showing positive for AE1/AE3, vimentin and Pax-8, and negative for desmin, like as epithelial pattern. The current concept of the histogenesis of CS is that the sarcomatous component derives from the carcinomatous component through an epithelial mesenchymal transition and metaplastic change of carcinoma cells [15]. The pleomorphic sarcoma might be derived from adenocarcinoma through dedifferentiation. Epithelial to mesenchymal transitions are transdifferentiated programs required for tissue morphogenesis during ontogenesis and these programs reemerge during tissue repair and in tissue neoplasms [16].
Most reported ovarian teratoid CS cases showed the elevated tumor markers, such as CA125, CA19-9, LDH; malignant transformation to squamous cell carcinoma from mature cystic teratoma revealed an elevated SCC level. In the present case, CA19-9 alone was slightly elevated in tumor markers, but CA19-9 has been reported to be high even benign mature cystic teratoma [17, 18]. CA19-9 may not be tumor marker showing the disease recurrence in this case.
In the present case, her genomic instability score was 73, showing positive HRD, but tumor BRCA1/2 mutations showed no clinically significant mutations. High level HRD has been sensitive to inhibitors of a PARP [9, 10]. IP regimen as well as paclitaxel and carboplatin, and bevacizumab have been used for ovarian CSs, but the results remained controversial [12, 19]. The IP regimen and PARP inhibitor(s) have been effective in the present case. The patient has been free from tumor recurrence up to now.
Conclusion
Ovarian teratoid carcinosarcoma is extremely rare and behaves in a highly aggressive manner. The cytological, histological and immunohistochemical findings were reported. In this case, optimal surgery, ifosfamide and cisplatin chemotherapy and a PARP inhibitor induced a good clinical course.
Acknowledgement
We thank the editor and reviewers for the constructive comments, which helped us to improve the manuscript. The written consent was approved by the patient before writing this case report.
Competing interests
The authors declare that they have no competing interests.
Ethical Approval
The ethical approval of our hospital was obtained the ethical committee before writing this case report (ethical approval no. 22052702).
References
-
Baum S, DiGregorio K, Alhassan R, Jormark S, Villella J (2019) Management options for a patient with squamous cell carcinoma arising in a mature cystic teratoma of the ovary. J Exp Ther Oncol 13(1): 45-48.
-
Gadducci A, Guerrieri ME, Cosio S (2019) Squamous cell carcinoma arising from mature cystic teratoma of the ovary: A challenging question for gynecologic oncologists. Crit Rev Oncol Hematol 133: 92-98.
-
Rim SY, Kim SM, Choi HS (2006) Malignant transformation of ovarian mature cystic teratoma. Int J Gynecol Cancer 16(1): 140-144.
-
Shanmugaratnam K, Kunaratnam N, Chia KB, Chiang GS, Sinniah R (1983) Teratoid carcinosarcoma of the paranasal sinuses. Pathology 15(4): 413-419.
-
Gersell DJ, Duncan DA, Fulling KH (1989) Malignant mixed müllerian tumor of the uterus with neuroectodermal differentiation. Int J Gynecol Pathol 8(2): 169-178.
-
Matsuura Y, Kitajima M, Hachisuga T, Tanimoto A, Okura N, et al. (2010) Malignant mixed müllerian tumor with malignant neuroectodermal components (teratoid carcinosarcoma) of the ovary: Report of a case with clinicopathologic findings. J Obstet Gynaecol Res 36(4): 907-911.
-
Fox C, Allen N, Schimp V, Maksem J (2019) Ovarian teratoid carcinosarcoma is an aggressive tumor of probable mullerian derivation with a carcinosarcomatous and mixed germ-cell morphology. Case Rep Oncol 12(1): 241-247.
-
Yoshioka T, Tanaka T (1998) Immunohistochemical and molecular studies on malignant transformation in mature cystic teratoma of the ovary. J Obstet Gynaecol Res 24(2): 83-90.
-
Telli ML, Timms KM, Reid J, Hennessy B, Mills GB, et al. (2016) Homologous recombination deficiency (HRD) score predicts response to platinum-containing neoadjuvant chemotherapy in patients with triple- negative breast cancer. Clin Cancer Res 22(15): 3764- 3773.
-
Moore KN, Secord AA, Geller MA, Miller DS, Cloven N, et al. (2019) Niraparib monotherapy for late-line treatment of ovarian cancer (QUADRA): a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol 20(5): 636-648.
-
Hain JAR, Birrer M, Carmen MGD (2016) Carcinosarcoma of the ovary, fallopian tube, and peritoneum: Prognostic factors and treatment modalities. Gynecol Oncol 142(2): 248-254.
-
Brackmann M, Stasenko M, Uppal S, Erba J, Reynolds RK, et al. (2018) Comparison of first-line chemotherapy regimens for ovarian carcinosarcoma: a single institution case series and review of the literature. BMC Cancer 18(1): 172.
-
Rutledge TL, Gold MA, McMeekin DS, Huh WA, Powell MA, et al. (2006) Carcinosarcoma of the ovary-a case series. Gynecol Oncol 100(1): 128-132.
-
Bishop JA, Feldstein JT, Westra WH, Pelosi G, Travis WD, et al. (2012) p40 (ΔNp63) is superior to p63 for the diagnosis of pulmonary squamous cell carcinoma. Mod Pathol 25(3): 405-415.
-
Amant F, Vloeberghs V, Woestenborghs H, Moerman P, Vergote I (2003) Transition of epithelial toward mesenchymal differentiation during ovarian carcinosarcoma tumorigenesis. Gynecol Oncol 90(2): 372-377.
-
Singh A, Settleman J (2010) EMT, cancer stem cells and drug resistance: an emerging axis of evil in the war on cancer. Oncogene 29(34): 4741-4751.
-
Coskun A, Kiran G, Ozdemir O (2008) CA 19-9 can be a useful tumor marker in ovarian dermoid cysts. Clin Exp Obstet Gynecol 35(2): 137-139.
-
Lin SC, Yen RF, Chen YK (2020) Dermoid cyst with secretion of CA 19-9 detected by 18F-FDG PET/CT: a case report. Medicine (Baltimore) 99(10): e18988.
-
Fujii H, Yoshida M, Gong ZX, Matsumoto T, Hamano Y, et al. (2000) Frequent genetic heterogeneity in the clonal evolution of gynecological carcinosarcoma and its influence on phenotypic diversity. Cancer Res 60(1): 114-120.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet