Mixed Invasive Ductal and Lobular Carcinoma of the Breast (IDC-L): Rare Morphological Subtype
Mixed Ductal-Lobular carcinomas (MDLs) show both ductal and lobular morphology. These are rare subtype of invasive breast cancer. We are reporting a 50 year female patient presented to surgical unit having complaint of lump in right breast which was gradually increasing in size. On clinical examination upper inner quadrant of right breast showed a single large lump measuring 4 x 3 x 2.5 cm, firm, tender and fixed posteriorly to chest wall. On sonomammography showed an ill-defined predominantly hypoechoic non circumscribed lesion measuring 8.1 x 2.5 X 2.2 cm with macro and microlobulations reported as BIRADS V highly suggestive of malignancy right breast mass. On histopathology we reported as Invasive breast carcinoma (30%) with invasive lobular carcinoma (60%) and focal neuroendocrine differentiation<10% (RB score = 2+3+2=7) Grade II. On immunohistochemistry tumor was ER, PR positive, and Her2 negative. We are presenting this mixed invasive ductal– lobular carcinomas case for its rarity with clinical, imaging, histomorphological and immunohistochemistry features.
Introduction
Mixed Ductal-Lobular carcinomas (MDLs) show both ductal and lobular morphology. They represent collision of different morphological tumors or evolve from a common progenitor. The WHO classification (2012) of breast tumors defined IDC-L as having an invasive lobular carcinoma (ILC) pattern in at least 50% of the tumor and an IDC pattern in between 10% and 49% [1]. IDC-L accounts for 3-5% of all breast cancers [2]. The available literature on IDC-L is sparse and has been conflicting with regards to outcomes and the response to neoadjuvant chemotherapy. In our case patient present with gradually increasing lump in right breast of 9 months duration. On histopathology reported as Mixed Ductal-Lobular carcinomas (MDLs). We are presenting this case for its rarity with clinical, imaging, histomorphological features.
A 50 year female patient presented to surgical unit having complaint of lump in right breast since 9 months, which was gradually increasing in size. It was associated with pain, tenderness in right breast. On clinical examination upper inner quadrant of right breast showed a single large lump measuring 4 x 3 x 2.5 cm, firm, tender and fixed posteriorly to chest wall. Overlying skin was puckered. There was no any significant family/hormonal history. There was no any systemic illness noted. On sonomammography showed an ill-defined predominantly hypoechoic non circumscribed lesion measuring 8.1 x 2.5 X 2.2 cm with macro and microlobulations. The spiculations and angulations were noted in right upper quadrant from II - 2 0’ clock position. The lesion was reaching the subcutaneous tissue with loss of fat planes with the overlying skin and was indenting the underlying pectoralis muscle with loss of fat planes. The lesion showed internal vascularity with RI 0.74.The lesion showed intermediate hardness on elastography studies. Distance of the lesion from the skin surface was 0.5 cm. Distance of the lesion from the nipple areola complex was 2.3 cm. Right axilla showed lymph nodes, few of maintained fatty hilum and few of them showing morphology and increased cortical thickness, suspicious for metastasis. Final impression given was BIRADS V, highly suggestive of malignancy right breast mass. The left breast and left axillary region was normal. There was no evidence of any systemic metastasis. Fine needle aspiration cytology done showed cellular smear with neoplastic cells arranged in clusters, sheath, in rows and scattered singly, reported as positive for carcinoma cells. Right Modified radical mastectomy was done. We received right breast mass, with axillary clearance.
On gross examination a specimen of right breast with mass totally measuring 21.5 x 17 x 3 cm and was weighing 550 Gms (Figure 1). The covering skin flap measured 15.2 x 7.5 cm. The nipple, areola appeared unremarkable. Serial cut sectioning revealed a tumor measuring 4.4 x 2.2 x 1.6 cm, located in upper inner quadrant of right breast. Tumor was grey white and firm in consistency (Figure 2). Tumor was infiltrating borders and was seen involving the skin. Cut section was grey white, with focal areas of necrosis and hemorrhage. Deep surgical margin was 0.2 cm away from tumor. The Right Axillary Clearance on serial cut sections revealed 23 lymph nodes. Largest lymph node measured 0.9 x 0.5 x 0.3 cm.
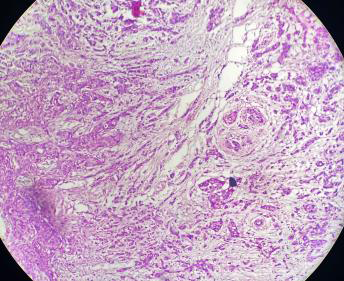
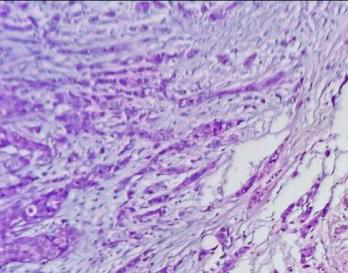
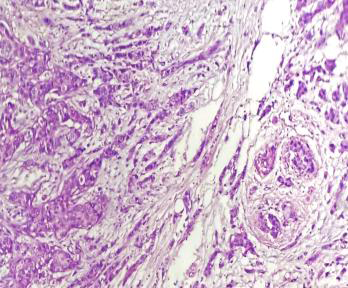
On histopathology the ILC areas showed tumor cells of low grade, arranged in single files, cords and single cells and at peripheral areas arranged concentrically around normal ducts, giving a targetoid appearance. The IBC areas showed tumor with glandular and solid areas with grade two nuclear features, while in focal neuroendocrine differentiation cells were composed of uniform tumor cells showing round to oval nuclei with salt and pepper chromatin. We reported as Invasive breast carcinoma (30%) with invasive lobular carcinoma (60%) and focal neuroendocrine differentiation (RB score = 2+3+2=7) Grade II (Figures 3-5). The tumor was reaching up to the skin. The lymphovascular invasion was noted .There was no evidence of neural invasion. Deep surgical margin was free from tumor. Adjacent breast tissue showed fibrocystic change. The one right axillary lymph node showed tumor metastasis. On immunohistochemistry tumor was ER, PR positive and Her2 negative.


Discussion
The breast carcinoma on histological examination shows various types .Among these invasive breast carcinoma (IBC) is the most common type, accounting for approximately 80% of all breast cancer cases. The invasive lobular carcinoma (ILC) accounts for 5% to 15%. The coexistence of mixed ductal-lobular carcinomas has attracted increased attention toward the mechanism and prognosis of these cases. There is a trend of increased incidence about 2-fold of invasive ductal-lobular breast carcinoma from last three decades [3]. As the ILC shows lower histological grade prognosis is good as compare to IBC. In our case fine needle aspiration cytology was done and reported as positive for carcinoma cells. FNAC of lobular hyperplasia and invasive lobular carcinoma is associated with high rate of equivocal diagnosis, so careful evaluation is required. Areas with neuroendocrine features like neoplastic cell with salt pepper chromatin has to look for Jagtap SV and Trivedi S, et al. [4, 5].
ILC on histological examination showed tumor cells of low grade, arranged in single files, cords and single cells and at peripheral areas arranged concentrically around normal ducts, giving a targetoid appearance. The ILC immunohistochemistry shows the loss of E-cadherin expression. Also tumor shows more estrogen receptor and progesterone receptor expression, and lower expression of human epidermal growth factor receptor 2.
It is found that IDC-L patients had lower tumor grade and higher hormone receptor positive proportions than IDC patients [6, 7]. In our case tumor showed grade II with immunohistochemistry tumor was ER, PR positive, and Her2 negative. Reed AEM, et al. observed that the MDLs more frequently coexist with ductal carcinoma in situ (DCIS) than with lobular carcinoma in situ (LCIS) [8].
The clinical significance of mixed invasive ductal and lobular carcinoma (IDC-L) in practice is often associated with uncertainty related to its prognosis and response to systemic therapies. In the study by Nasrazadani A, et al. stated that a prominent role for the lobular component in this mixed subtype in driving biology, including response to neoadjuvant therapy and metastatic dissemination [9]. In our case the invasive lobular carcinoma component was predominant (60%) and also the nodal metastasis was noted in only one axillary lymph node.
The patients with IDC-L had a higher frequency of lymph node metastases despite the presence of features typically considered to be prognostically favorable. In the IDC-L, Tumor-Node-Metastasis (TNM) stage III was predominantly observed in the study by Zengel B, et al. [10]. IDC-L is associated with a survival advantage. It predicts a worse prognosis than IDC for patients both in the ER-positive and ER-negative subgroup [6]. The various studies showed that the MDLs are associated with a better prognosis than IDC, but a poorer prognosis than ILC [11]. The data may imply that Mixed IDC-L tumors may behave clinically more like ILC than IDC, but larger studies are needed to study this rare breast cancer subtype.
Conclusion
Mixed invasive ductal and lobular carcinoma is a rare subtype of invasive breast cancer. We are presenting this case for its rarity with clinical, imaging, histomorphological features.
References
-
Nenutil R (2015) A revolution postponed indefinitely. WHO classification of tumors of the breast 2012: the main changes compared to the 3rd edition (2003). Cesk Patol 51(1): 23-25.
-
Li CI, Uribe DJ, Daling JR (2005) Clinical characteristics of different histologic types of breast cancer. Br J Cancer 93(9): 1046-1052.
-
Bharat A, Gao F, Margenthaler JA (2009) Tumor characteristics and patient outcomes are similar between invasive lobular and mixed invasive ductal/ lobular breast cancers but differ from pure invasive ductal breast cancers. Am J Surg 198(4): 516-519.
-
Jagtap SV, Beniwal A, Shah HP, Jagtap SS (2016) Application of Probabilistic Approach in Reporting Breast Lesions on Fine Needle Aspiration Cytology: Institutional Study. National Journal of Laboratory Medicine 5(2): 17-21.
-
Trivedi S, Dixit N, Suri M (2021) Fine needle aspiration cytology of primary neuroendocrine tumor of the breast and its differential diagnosis. Diagn Cytopathol 49(1): 171-175.
-
Xiao Y, Ma D, Ruan M, Zhao S, Liu XY, et al. (2017) Mixed invasive ductal and lobular carcinoma has distinct clinical features and predicts worse prognosis when stratified by estrogen receptor status. Sci Rep 7: 10380.
-
Jagtap SV, Beniwal A, Chougule PG, Shah HP, Jagtap SS (2016) Invasive lobular carcinoma of breast histopathological subtypes: clinicopathological study. Int J Health Sci Res 6(7): 105-111.
-
Reed AEM, Kutasovic JR, Nones K, Saunus JM, Silva LD, et al. (2018) Mixed ductal-lobular carcinomas: evidence for progression from ductal to lobular morphology. J Pathol 244(4): 460-468.
-
Nasrazadani A, Atkinson J, Li Y, McAuliffe P, Jankowitz R, et al. (2020) Mixed invasive ductal and lobular carcinoma (IDC/L) behaves similarly to invasive lobular carcinoma (ILC) with regard to neoadjuvant chemotherapy response and metastatic dissemination. Cancer Res 80(4S): P2-16-26.
-
Zengel B, Yararbas U, Duran A, Uslu A, Eliyatkin N, et al. (2015) Comparison of the clinicopathological features of invasive ductal, invasive lobular, and mixed (invasive ductal + invasive lobular) carcinoma of the breast. Breast Cancer 22(4): 374-381.
-
Rakha EA, Gill MS, Sayed MEE, Khan MM, Hodi Z, et al. (2009) The biological and clinical characteristics of breast carcinoma with mixed ductal and lobular morphology. Breast Cancer Res Treat 114(2): 243-250.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet