Diagnostic Accuracy of Periodic Schiff-Methenamine Silver and Masson’s Trichrome Stains for Immune Complex Deposits in Lupus Nephritis
Context: The Immunofluorescence technique is considered gold standard in the diagnosis of lupus nephritis. Special stains like Periodic Schiff-Methenamine stain (PASM) and Masson’s Trichrome (MT), which are more easily accessible, are hypothesized to have an accuracy similar to Immunofluorescence in diagnosing lupus nephritis. Aims: The aim of this study is to assess the diagnostic accuracy of Periodic Schiff-Methenamine stain (PASM) and Masson’s Trichrome (MT) stains for immune complex deposits in lupus nephritis. Settings and Design: The study was conducted in a laboratory environment. Renal biopsy samples, which showed full-house deposits on Immunofluorescence were considered. The corresponding biopsy slides were further studied under a light microscope using special stains like PASM and MT. Methods and Material: Fuchsinophilic (red) deposits in the glomeruli were identified as sub-endothelial, sub-epithelial and mesangial deposits under the light microscope and were used to classify lupus nephritis as per the ISN/RPS classification. Statistical analysis used: Diagnostic accuracy study was carried out and the degree of agreement between special stains and Immunofluorescence was expressed as frequencies and percentages. Results: 86.84% of the sample showed agreement between special stains (PASM and MT) and Immunofluorescence. This was most evident in class III and IV lupus nephritis cases with 96.42% agreement. Conclusion: Special stains like PASM and MT were accurate enough to be used in resource limited areas, where Immunofluorescence is not readily available.
Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease, where autoantibodies are produced against normal body tissues. This disease affects multiple organ systems, including kidney. When it affects the kidney, it is called ‘Lupus Nephritis’. The renal manifestations are due to the deposition of circulating immune complexes in the glomeruli. These immune complexes could be deposited either in the mesangial, sub-endothelial or sub-epithelial locations in the glomeruli. Using this as one of the criteria, an ISN/RPS (International Society of Nephrology and the Renal Pathology Society) classification has been developed which classifies lupus nephritis into 6 classes [1, 2].
These deposits are seen distinctly under the light microscope using special stains like Periodic Schiff- Methenamine stain (PASM) and Masson’s Trichrome (MT) stains. For example, in class III and IV lupus nephritis, fuschinophillic (red) sub-endothelial deposits can be seen along the capillary walls. In case of a class V lupus nephritis, sub-epithelial deposits are seen as irregular thickening of the capillary walls due to presence of ‘spikes’ external to the basement membrane.
When the kidney is affected in SLE, the risk of morbidity and mortality is the highest and needs immediate and targeted treatment. A much higher percentage of patients can be detected accurately with renal disease if biopsies are performed systematically on all SLE patients with light microscopic and Immunofluorescence studies [3, 4, 5, 6].
Studies have shown that there is a good relationship between renal function and patterns of glomerular deposits as determined by light microscopic and immunofluorescence studies [7]. Therefore, the decision to start on immunosuppressive therapy depends on the light microscopic and immunofluorescence results.
Even though Immunofluorescence and electron microscopy are regarded as the gold standards in the diagnosis of lupus nephritis, Lin J, et al. [8] they are expensive and not easily available in every place. On the other hand, special stains are more easily available in resource-limited areas. Therefore, studying the morphological findings using special stains to diagnose lupus nephritis can be advantageous in these areas [9].
Masson’s Trichrome stain is less expensive and can identify most aspects of glomerular pathology, especially in the most commonly occurring classes, such as class III and IV [10]. It has been shown to have a good agreement with electron microscopic and immunofluorescence studies [11].
An easily available diagnosis using special stains like PASM and MT in Light microscopy, which are more abundantly accessible at many places, is therefore considered advantageous [9].
The aim of this project is to assess the diagnostic accuracy of Periodic Schiff-Methenamine stain (PASM) and Masson’s Trichrome (MT) stains for immune complex deposits in lupus nephritis.
Subjects and Methods
This study was approved by the Institute Ethics Committee for Human Studies at Jawaharlal Nehru Institute of Post Graduate Medical Education and Research (JIPMER), Puducherry, India. Its retrospective study. Cases suspected as lupus nephritis in view of the clinical symptoms and whose renal biopsies showed ‘full-house’ deposits under Immunofluorescence (deposits containing IgG, IgM, IgA, C1q, C4, C3) were considered for this study. Corresponding slides stained with the special stains (i.e., PASM and MT) were then collected from the Department of Pathology. Data collection period extended from January 2017 to 30th July 2017.
Fifty-three cases of lupus nephritis was the initial expected sample size. However, the number of patients with lupus nephritis showing full-house deposits under Immunofluorescence within the data collection period was limited. Therefore, only 38 lupus nephritis cases could be studied. A diagnostic accuracy study was carried out to arrive at the frequencies and percentages.
Data was collected in a de-identified format, that is, without collecting patient identifiers. The slides were identified by their biopsy numbers that had been already assigned to them. The slides collected were studied under the light microscope. Blinding was done to mask the Immunofluorescence pattern. Fuchsinophilic (red) deposits in glomeruli were identified as mesangial, sub-endothelial and sub-epithelial deposits using PASM and MT stains and the class of lupus nephritis was assigned as per the ISN/RPS classification [1].
Each slide was assigned class I if there were no deposits observed under the light microscope. Class II was assigned if mesangial deposits were observed. If sub-endothelial deposits were observed, the slide was identified as class III
or IV. Class V was assigned if sub-epithelial deposits were seen.
After sample collection and classification using PASM and MT stains was completed, the Immunofluorescence result for each slide studied was unmasked. Thereafter, a comparison chart was prepared using the results from Immunofluorescence as well as those obtained under special stains.
A diagnostic accuracy study was carried out. Distribution
of data on the status of fuchsinophilic deposits in glomeruli was expressed as frequencies and percentages. The percentage of agreement between special stains (PASM and MT) and Immunofluorescence results was calculated and the diagnostic accuracy of the special stains was estimated.
Results
Out of the total 38 samples, 28 were identified as Class III and class IV lupus nephritis using special stains, i.e., PASM and MT stains (Table 1 & Figure 1).
| Immunofluorescence results | Results using special stains | |
|---|---|---|
| Class | Frequency | Frequency |
| I | 2 (5.26%) | 3 (7.89%) |
| II | 4 (10.52%) | 4 (10.52%) |
| III | 20 (52.63%) | 17 (44.73%) |
| IV | 11 (28.94%) | 11 (28.94%) |
| V | 1 (2.63%) | 2 (5.26%) |
| III + V | 0 | 1 (2.63%) |
| Total | 38 (100) | 38 (100) |
Table 1: Frequency table of Immunofluorescence results and results from special stains.
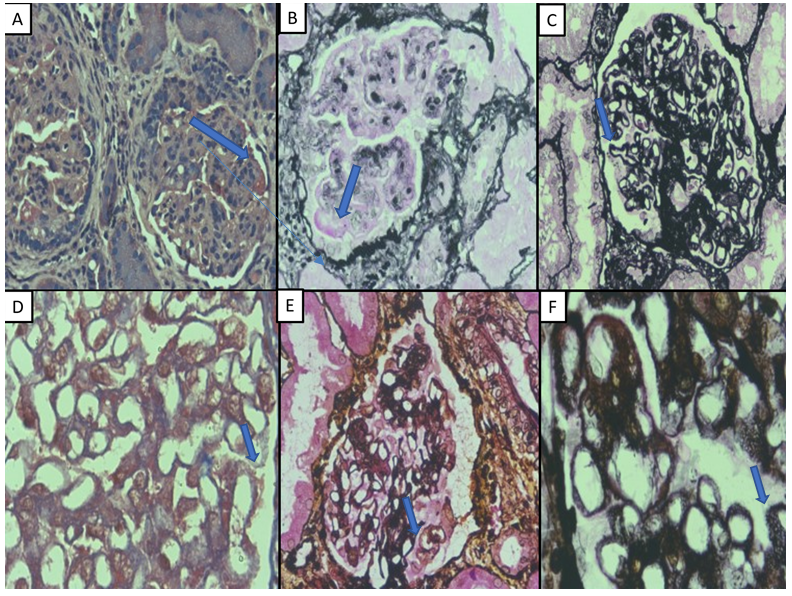
Figure 1: Fuchsinophilic deposits seen in various classes of lupus nephritis using PASM and MT stains (A and B): class IV lupus nephritis, sub-endothelial deposits using MT (X 400) and PASM (X400); (C and D): class V lupus nephritis, sub-epithelial deposits (spikes) using PASM (X400) and MT (X 1000); (E): class II lupus nephritis, mesangial deposits with PASM (X400). (F): class III with class V lupus nephritis, sub-endothelial and sub-epithelial deposits by PASM (X1000).
This makes them the most common classes that were observed. They represented 44.73% and 28.94% of the total sample size respectively. Out of these 28 cases, 27 (96.42%) had morphological findings coinciding with Immunofluorescence results. The remaining one case (out of the 28 cases) was reported to be class I by Immunofluorescence results. These findings suggest a strong agreement between Light Microscopy using PASM and MT stains and Immunofluorescence.
Table 1 shows the number of slides of each class as observed using PASM and MT stains and also as reported by immunofluorescence studies. The percentage of each class is mentioned.
Out of the remaining ten samples viewed under the light microscope, three cases were identified as class I lupus nephritis with no detectable deposits under the light microscope. However, only one out of those three cases coincided with the Immunofluorescence result. The other two were reported as class III by Immunofluorescence. Another four cases out of the ten were identified as class II using special stains; all of them also coincided with the Immunofluorescence results (100% agreement; Table 2 and Graph 1). One case was reported as III + V using special stains; this case had sub-endothelial and sub- epithelial deposits. This finding did not agree with the Immunofluorescence result as it reported the case as class III. Two cases were identified as class V using PASM and MT, out of which only one coincided with Immunofluorescence results (50% agreement).
| *PASM and MT results** | Immunofluorescence results | Row total | ||||
|---|---|---|---|---|---|---|
| I | II | III | IV | V | ||
| I | 1 | 0 | 2 | 0 | 0 | 3 |
| II | 0 | 4 | 0 | 0 | 0 | 4 |
| III | 1 | 0 | 16 | 0 | 0 | 17 |
| IV | 0 | 0 | 0 | 11 | 0 | 11 |
| III + V | 0 | 0 | 1 | 0 | 0 | 1 |
| V | 0 | 0 | 1 | 0 | 1 | 2 |
| Column total | 2 | 4 | 20 | 11 | 1 | 38 |
Table 2: Cross tabulation of special stains and Immunofluorescence results. *Periodic Schiff-Methenamine (PASM) **Masson’s Trichr
Table 2: Cross tabulation of special stains and Immunofluorescence results. *Periodic Schiff-Methenamine (PASM) **Masson’s Trichrome stain Table 2 is a cross tabulation of the results from special stains and immunofluorescence. Rows consist of the number of slides of each class as seen using the special stains. The columns consist of number of slides of each class as per immunofluorescence results.
Numbers highlighted in red are those cases in which light microscopy results did not coincide with Immunofluorescence results.
Graph 1 represents the percentage of findings using special stains that coincide (blue) and that does not coincide (orange) with the immunofluorescence results. The numbers within the bars represent frequencies.
In total, 33 out of 38 (86.84%) cases showed concordant results using special stains (PASM and MT stains) and Immunofluorescence. Class III and class IV lupus nephritis had a strong agreement (94.11% and 100% respectively) between results using special stains and Immunofluorescence. Diagnosis of Classes I and III+V showed divergence between these two techniques.
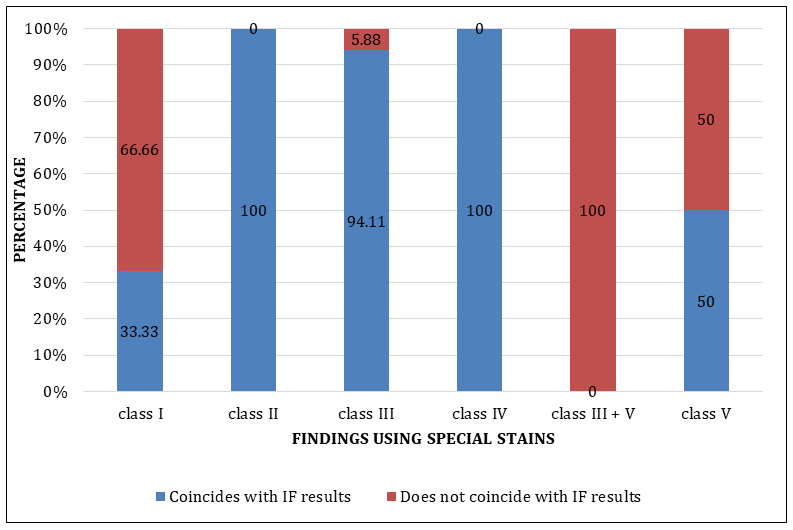
Graph 1: Graphical representation of the concordance between special stains (PASM and MT) and Immunofluorescence (IF) results.
Discussion
Lupus nephritis is classified into six classes, each of which have different clinical, morphological as well as treatment modalities. Hence, the diagnosis of the class of lupus nephritis is important. In the present study special stains like PASM and MT stain are hypothesized to have an accuracy similar to Immunofluorescence in classifying lupus nephritis. However, the efficacy of special stains in diagnosing lupus nephritis has not been studied widely. There is only one paper among the literature reviewed that studied the correlation between special stains, electron microscopy and immunofluorescence techniques with renal function in lupus nephritis [7]. Hence, primary research was undertaken to study the diagnostic accuracy of special stains like PASM and MT.
The study showed that the identification of lupus nephritis using special stains like PASM, and MT stains compared well with Immunofluorescence results, with an overall agreement rate of 86.84%. Most of the cases diagnosed using PASM and MT stains were either class III or IV. These were also the classes that were most commonly reported by Immunofluorescence studies. These findings are also in accordance with the study conducted by TK Chow, et al. [10] and Akhter S [12] where class IV had been reported to be the most common form of lupus nephritis. Their study also showed that class I and VI were the least common, which was also observed in our study in which only 3 specimens out of the total 38 were reported as class I. There were no specimens reported as class VI either under Light Microscopy or Immunofluorescence.
The present study also concluded that the class of lupus nephritis can be determined by identifying the patterns of immune deposits using PASM and MT and classifying them using the ISN/RPS criteria.
It was found that sub-endothelial deposits are clearer in PASM stain than in MT stain. In 2 specimens, sub-endothelial deposits were identified using PASM, but not by the MT stain. It was also found that mesangial deposits are generally difficult to identify in PASM and MT stain. This is also stated in the study conducted by Cohen, et al. [13]. Thus, diagnosis of class II lupus nephritis, which requires identification of mesangial deposits, was more difficult using special stains than Immunofluorescence. Among the two special stains used, PASM and MT, the mesangial deposits appeared relatively clearer using MT stain rather than PASM stain. 8 out of 38 slides showed mesangial deposits under MT stain but could not be identified under PASM stain. Interestingly, this finding agrees with the study conducted by Cohen, et al. [11].
The study also highlighted a few disadvantages. If the activity score is low, it is more difficult to identify sub-endothelial deposits using special stains than using Immunofluorescence. This is due to the higher contrast provided by immunofluorescent stains. In 2 cases in the study, occasional sub-endothelial deposits could not be detected using special stains although the Immunofluorescence method had reported class III. The commonest error in assessment of the Masson’s trichrome-stained specimens was the erroneous interpretation of specimens showing minimal change nephropathy or ischemic glomerulopathy by immunofluorescence and electron microscopy.
An alternative explanation is possible for the high degree of agreement between the results from Immunofluorescence and Light Microscopy (using PASM and MT stains). Most of the patients in the Out-Patients department, and detected with lupus nephritis are class III or IV, the identification of which, is easier using the special stains. Class V may also be diagnosed accurately, by the presence of spikes, seen using PASM and MT stains. Using special stains, the real challenge is in the diagnosis of class I and II lupus nephritis showing mesangial deposits which are hard to identify with the special stains. It is also essential that differential diagnoses of class IV and V deposits like, advanced sclerosing lupus nephritis, tubulointerstitial disease, end-stage renal disease with acquired cystic disease, membranoproliferative glomerulonephritis, concomitant vascular or tubulointerstitial lesions, etc. should be carefully looked for [14, 15].
Only full house deposits under Immunofluorescence were considered in the inclusion criteria. Special stains and Immunofluorescence results for an atypical lupus nephritis (non-full house deposits) was not included in the study. Further probing can be done to study accuracy of special stains in cases of atypical lupus nephritis cases which do not have full house deposits.
While conducting the study, slides were collected from January 2017 until July 2017. In some of the slides, staining had faded, and it was difficult to identify deposits. This probably would not have been the case had the identification been done immediately after staining. These slides had to be removed from the study, thus reducing total sample size. The study would become more robust if the sample size is increased to 100 which would also increase the probability of occurrence of classes I, II and V. Additionally, prior therapy was not taken into consideration. It has been reported that steroid treatment reduces the amount of deposits [16]. This can give rise to wrong interpretation.
Despite the disadvantages, it is clear that special stains like MT and PASM can be used in diagnosis of lupus nephritis with an overall accuracy of 86.84% and approaching 100% for specific classes. Indeed, only in case of doubt while using the special stains, need the Immunofluorescence result be sought.
Special stains have implications on treatment options for various classes of lupus nephritis, as different treatment modalities exist for each class [17]. Hence, in areas where Immunofluorescence is not available, use of special stains like PASM and MT attain great importance.
References
-
Markowitz GS, D’Agati VD (2007) The ISN/RPS 2003 classification of lupus nephritis: an assessment at 3 years. Kidney Int 71(6): 491-495.
-
Weening JJ, D’Agati VD, Schwartz MM, Seshan SV, Alpers CE, et al. (2004) The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int 65(2): 521-530.
-
Mittal B, Rennke H, Singh AK (2005) The role of kidney biopsy in the management of lupus nephritis. Curr Opin Nephrol Hypertens 14(1): 1-8.
-
Schwartz MM, Bernstein J, Hill GS, Holley K, Phillips EA (1989) Predictive value of renal pathology in diffuse proliferative lupus glomerulonephritis. Lupus Nephritis Collaborative Study Group. Kidney Int 36(5): 891-896.
-
Hill GS, Delahousse M, Nochy D, Tomkiewicz E, Rémy P, et al. (2000) A new morphologic index for the evaluation of renal biopsies in lupus nephritis. Kidney Int 58(3): 1160-1173.
-
Grande JP, Balow JE (1998) Renal biopsy in lupus nephritis. Lupus 7(9): 611-617.
-
Sinniah R, Feng PH (1976) Lupus nephritis: correlation between light, electron microscopic and immunofluorescent findings and renal function. Clin Nephrol 6(2): 340-351.
-
Lin J, Markowitz GS, Valeri AM, Kambham N, Sherman WH, et al. (2001) Renal Monoclonal Immunoglobulin Deposition Disease: The Disease Spectrum. J Am Soc Nephrol 12(7): 1482-1492.
-
Weidner N, Oates J, Tung KS (1981) The accuracy of Masson’s trichrome stain in predicting the presence or absence of glomerular immune complexes. Am J Clin Pathol 75(4): 542-545.
-
Chow TK, Looi LM, Cheah PL (2015) A comparison of 1995 WHO classification with 2003 ISN/RPS classification of lupus nephritis: a single centre observation. Malays J Pathol 37(3): 239-246.
-
Cohen AH (1976) Masson’s trichrome stain in the evaluation of renal biopsies: An appraisal. Am J Clin Pathol 65(5): 631-643.
-
Akhter S, Kamal M (2013) Histomorphological patterns of lupus nephritis with evaluation of WHO 1982 and ISN/RPS 2003 classifications. Mymensingh Med J 22(3): 557-566.
-
Cohen AH, Border WA, Glassock RJ (1978) Nephrotic syndrome with glomerular mesangial IgM deposits. Lab Invest 38(5): 610-619.
-
Jagtap SV (2020) Multilocular cystic renal neoplasm- low malignant potential (MCRN-LMP)- review. Ann Urol Oncol 3(2): 97-102.
-
Najafi CC, Korbet SM, Lewis EJ, Schwartz MM, Reichlin M, et al. (2001) Significance of histologic patterns of glomerular injury upon long-term prognosis in severe lupus glomerulonephritis. Kidney Int 59(6): 2156-2163.
-
Grisham E, Gerber MA, Churg J (1982) Patterns of renal injury in systemic lupus erythematosus: light and immunofluorescence microscopic observations. Am J Kidney Dis 2(S1): 135-141.
-
Mok CC (2012) Understanding lupus nephritis: Diagnosis, management and treatment options. Int J Womens Health 4: 213-222.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet