False Positive Conventional Cytogenetic Findings that Mimic the Recurrent Chromosome Abnormalities Associated with Hematolymphoid Disorders
Recurrent chromosome abnormalities as defined in the World Health Organization (WHO) play a major role in diagnosis, prognosis, and treatment. Herein, we describe two cases of hematologic malignancies with chromosomal abnormalities mimicking WHO-define recurrent abnormalities. Both cases demonstrate clinical utility of interphase and metaphase fluorescence in-situ hybridization (FISH) in confirming the WHO defined recurrent cytogenetic abnormalities. The first is a case of chronic myeloid leukemia (CML) with both t(9;22)(q34;q11.2) and inv(3)(q21q26.2) by conventional cytogenetics but no EVI1::MECOM rearrangement by FISH. The second is a case of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) with deletion of 11q (ATM) and a subclone with deletion of 6q (MYB) and t(9;22)(q34;q11.2) detected by conventional cytogenetics but no BCR::ABL1 fusion by FISH. These cases demonstrate that conventional cytogenetics and FISH studies are complementary and especially so when recurrent abnormalities are suggested by karyotype.
Introduction
Chronic myeloid leukemia (CML) is a pluripotent hematopoietic stem cell disorder defined by expression of Investigation Paper the BCR::ABL1 fusion gene, a constitutively activated tyrosine kinase, harbored by the Philadelphia (Ph) chromosome, which is a result of a t(9;22)(q34;q11) or a related variant translocation.
The Ph chromosome is the name given to the derivative chromosome 22 featuring t(9;22)(q34;q11). This small derivative chromosome is a product of reciprocal translocation between the ABL1 and BCR genes on chromosomes 9 and 22, respectively, resulting in formation of the well-known fusion gene, BCR::ABL1. The protein product of this translocation promotes leukemogenesis via unchecked cell proliferation, inhibition of cell differentiation, and resistance to cell death. Although a hallmark feature of CML, the BCR::ABL1 translocation is also seen in cases of acute lymphoblastic leukemia, de novo acute myeloid leukemia (AML), and mixed-phenotype acute leukemia [1, 2].
Cells with the Ph chromosome tend to show genetic instability and are prone to develop multiple and heterogenous genomic abnormalities. This sets the foundation for transformation of the leukemic phenotype from chronic phase to accelerated phase and ultimately blast phase [2].
CML in childhood presents as one of the two clinically distinct syndromes, adult-type CML (ACML) which is Ph(1) positive, and juvenile CML, also known as Juvenile Myelomonocytic Leukemia (JMML), which is Ph(1) negative [3].
In the context of CML, Ecotropic Virus Integration site-1 (EVI1) rearrangement, resulting from either inv(3)(q21q26) or t(3;3)(q21q26), is associated with a more aggressive disease course [1, 2]. EVI1 (MECOM) is a transcription factor with stem cell specific expression patterns which mediates growth of hematopoietic stem cells and plays a role in AML, myelodysplastic syndrome (MDS), and CML [1]. Inv(3) and t(3;3) involving q21q23 breakpoints results in EVI1 expression being controlled by the enhancer for the GATA2 gene at 3q21.7 Furthermore, EVI1 overexpression is implicated in aggressive clinical course in several epithelial malignancies and the targets of its regulatory activity in these cancers are the subject of ongoing research.
Case Presentation
Case 1
A 31-year-old male presented from a community hospital with severe leukocytosis (WBC 356.4 K/uL), thrombocytopenia (PLT 38 K/uL), and symptoms of leukostasis highly suspicious for leukemia. Stat FISH on peripheral blood was negative for t(15;17)/PML::RARA, excluding acute promyelocytic leukemia (APL). Bone marrow examination revealed a hypercellular marrow (100%) with markedly increased granulopoiesis and 4% blast; concurrent flow cytometry reported less than 1% myeloid blasts. FISH identified t(9;22)/BCR::ABL1 with der (22) Ph chromosome, confirming the diagnosis of CML.
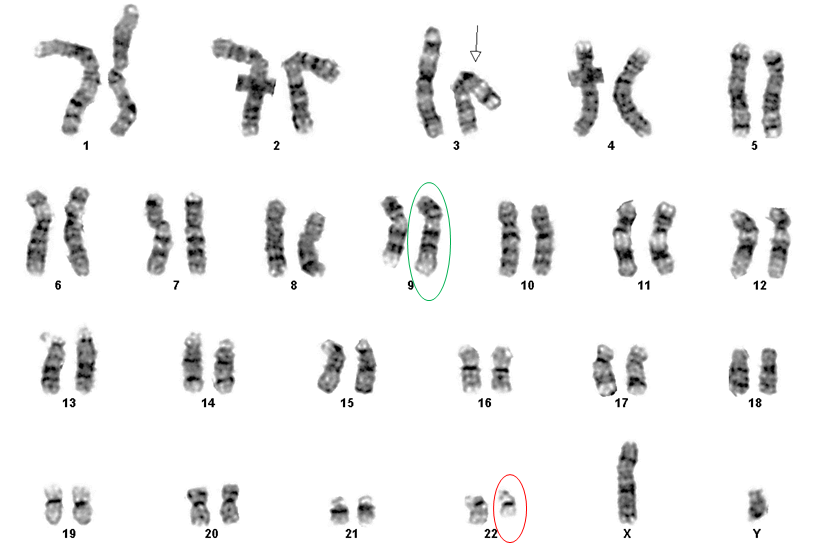
Conventional cytogenetic studies on bone marrow yielded:
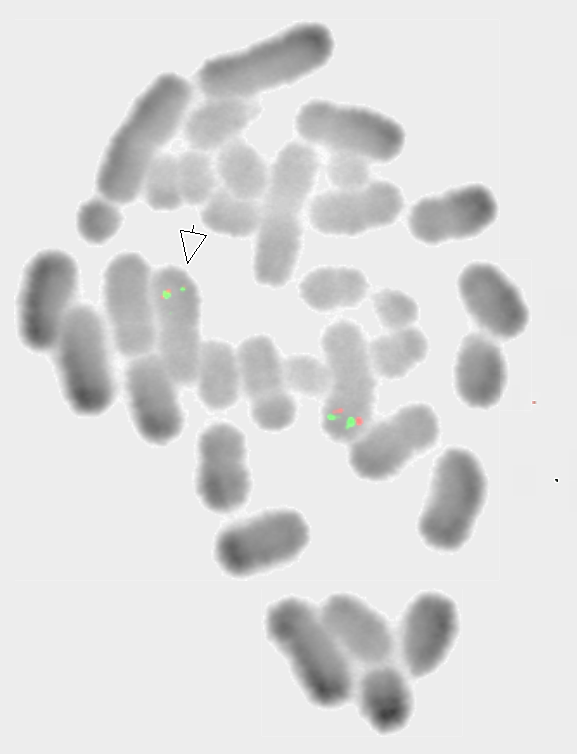
46,XY,inv(3)(q21q26.2),t(9;22)(q34;q11.2)[20] (Figure 1) Interphase FISH with a dual-color dual-fusion probe set identified t (9;22) in 96.5% of cells with positive fusion signal on der(22) on metaphase analysis, but no signal on der (9) due to submicroscopic deletion. A break-apart probe for EVI1 rearrangement was negative on both interphase and metaphase analysis. (Figure 2).
Karyotyping identified two concurrent chromosomal abnormalities associated with the patient’s phenotypic CML. t(9;22)/BCR::ABL1 was confirmed by FISH while EVI1 rearrangement was not identified. The significance of an inv(3) which does not rearrange EVI1 is unknown. FISH results did not change the diagnosis but yielded the correct prognosis for the patient’s disease.
Risk profiles for therapy in CML are based on, depending on scoring system, measures of blood counts, spleen size, and age. EVI1 rearrangement predicts a worse outcome in CML but does not directly factor into risk assessment and therapy decisions [2]. Which generation of tyrosine kinase inhibitor (TKI) to initiate treatment with is informed by risk profiling. Inadequate response to TKI, disease progression under appropriate TKI, or advancement to accelerated or blast phase disease may all be indicators for consideration of hematopoietic cell transplant [4].
Worsening thrombocytopenia and inv (3) raised concern for increased risk of progression to accelerated phase and prompted transplant planning. The patient received a myeloablative chemotherapy regimen prior to a matched sibling donor peripheral stem cell transplant. Five-year post- transplant testing showed no BCR::ABL1 p210 transcripts by reverse transcriptase polymerase chain reaction (RT-PCR). Engraftment analysis showed 100% donor cells. Case 2 A 76-year-old female with melanoma was incidentally diagnosed with small lymphocytic lymphoma (SLL) on axillary sentinel lymph node biopsy while undergoing treatment for her melanoma. Peripheral blood flow cytometry identified the presence of clonal CD5 (+) B cells, with an immunophenotypic profile compatible with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/ SLL). The patient was asymptomatic for several years but had increasing lymphocytosis.
Clinical progression was evident at the 3.5-year mark, with progressively worsening anemia and new lymphadenopathy in cervical, axillary, and inguinal nodes. Staging bone marrow evaluation revealed CLL in a hypercellular marrow (70%), with decreased trilineage hematopoiesis and 96% lymphocytes.
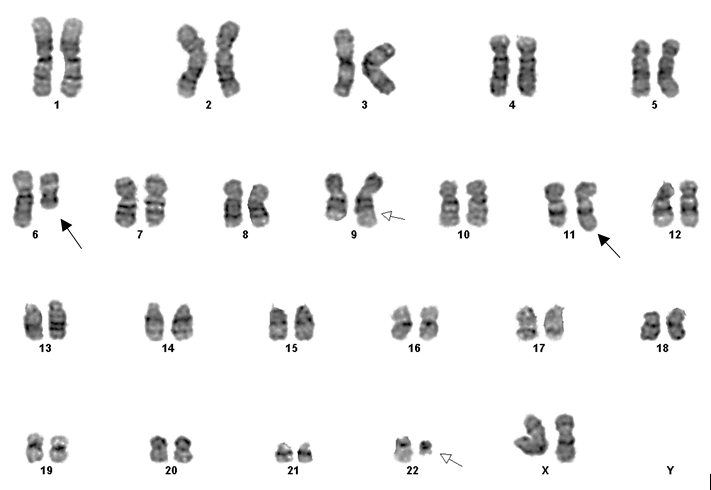
Cytogenetic studies on the bone marrow with DSP30/ IL2 mitogen stimulated culture cells revealed: 46,XX,add(11) (q21)[cp14]/46,sl,del(6)(q21),t(9;22)(q34;q11.2) [cp4]/46,XX[cp2] (Figure 3).
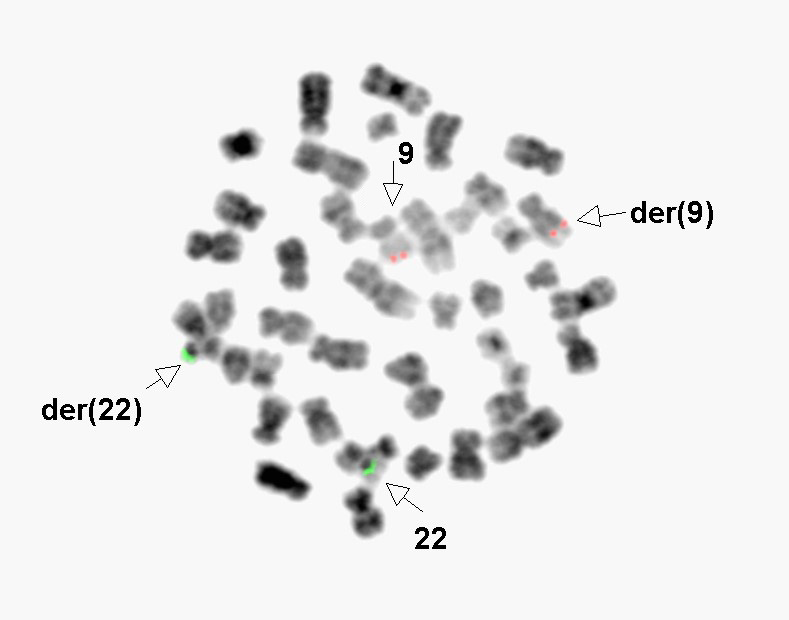
FISH assays for deletions of 6q, 11q, 13q, and 17p, and +12, common abnormalities in CLL, were performed on direct cultured bone marrow cells. Abnormal signals were observed for deletions of 6q and 11q, each at 2%. Conventional cytogenetic studies showing t (9;22) prompted FISH assays for t(9;22)/BCR::ABL1. Dual-color dual-fusion probe sets were performed on both interphase (Figure 4) and metaphase cells and were negative.
These FISH results were different from studies obtained 7 and 25 months previously, which were negative for deletions of 6q, 11q, 13q, and 17p, +12, and t(11;14). A previous conventional karyotype was not available for comparison.
The patient’s bone marrow specimen showed deletion of 11q and a subclone with deletion of 6q and t(9;22) (q23;q11.2). FISH detected both 11q and 6q deletion, but did not identify t(9;22) involving ABL1 and BCR genes. This complex karyotype, defined as having 3 or more structural or numeral aberrations, is associated with a poor outcome. By itself del (11q) is an independent negative prognostic abnormality in CLL/SLL [2].
NCCN guidelines call for testing for del(17p), TP53 mutation, karyotype, and immunoglobulin heavy chain variable region mutation status prior to initiating treatment. Karyotype and IGHV are prognostic but don’t change the treatment algorithm while TP53 or del(17p) do as they predict reduced response to chemotherapy [5].
The degree of bone marrow involvement and presence of bulky adenopathy prompted treatment, initially consisting of Obinutuzumab, ibrutinib, and venetoclax (added after cycle 3) per clinical trial parameters. Response was excellent, with marked improvement of adenopathy prior to cycle 3. Obinutuzumab was discontinued due to neutropenia. Peripheral blood flow cytometry was negative for lymphoma at that time. Bone marrow aspirate and peripheral blood flow cytometry were negative for lymphoma one year later. Biannual peripheral blood flow cytometry has remained negative for evidence of lymphoma to date (2022).
Discussion
Published literature features plentiful information on cytogenetic and FISH concordance and utility in hematological malignancies with concordance rates typically greater than 95%. A search for discordant results in hematolymphoid malignancies yields primarily studies involving AML and MDS diagnosis and monitoring, with few results showing discordances similar to the presented cases.
He et al and Wheeler et al calculated concordance rates between conventional cytogenetics and FISH in studies of adults with AML in published studies of 220 and 204 patients, respectively. He, et al. [6] found 97.7% concordance. Their low number of discordant cases included those with cryptic translocations, with single abnormal metaphase on karyotype, and those with low-level FISH abnormalities. Wheeler et al reported a concordance rate of 95%. Discordance in their study was due to low-level FISH abnormalities and polyploid clones not detected on karyotype. Of their 10 discordant cases, one had clinical relevance with a t (15;17) due to cryptic RARA insertion. Both studies stated that adequate karyotype is sufficient in most cases of adult AML and FISH is usually of little added value but recognized that FISH has high sensitivity in disease monitoring. He et al specifically advocated confirmatory FISH for karyotypes consistent with WHO-defined recurrent abnormalities [6, 7].
Cherry, et al. [8] compared cytogenetics and FISH in patients with MDS and concluded the two had similar sensitivity for this population. Of 48 samples, karyotype and FISH identified abnormalities in 18 and 17 cases, respectively. An occult -11 was identified by FISH in one case. FISH may detect abnormalities occurring at a small percentage as well as in cells with low mitotic activity that may not culture well or at all, while karyotyping can identify abnormalities for which FISH probes aren’t available [8]. Cantú, et al. examined 32 cases for possible causes of discordant karyotype and FISH results. Excluding laboratory error, their discordances were categorized as normal karyotype with abnormal interphase FISH (i-FISH), abnormal karyotype with normal i-FISH, and abnormal karyotype with abnormal i-FISH but differing results. Discordant results were attributed as often being due to the intrinsic nature of malignant cells. This fact accounted for 34.4% of their observed discordant results. Culture condition and choice of mitogens and mitosis arresting agents may alter yields of cells of interest. They further elaborated that mitotically active and inactive populations are effectively separate populations with possibly different abnormalities, such that metaphase FISH (m-FISH) is needed to resolve discordance between karyotype and i-FISH. Biclonality was also a source of discordance wherein m-FISH established presence of a sub-clone when karyotype and i-FISH were both abnormal but different [9].
Wlodarska, et al. [10] reported a case of follicular lymphoma demonstrating a karyotype of 46,XY,t(8;14) (q24;q32),t(9;22)(q34;q11),t(14;18)(q32;q21). FISH for t (9;22) showed rearrangement but no fusion on der(22). RT- PCR and Southern blot were negative for BCR rearrangement. Additional studies identified breaks on chromosomes 9, telomeric to NOTCH 1 (and therefore ABL1), and 22 between lambda light chain (IGL) constant and variable region (centromeric to BCR), yielding a fusion signal on der (9) but not on der (22). The unexpected FISH result, with no fusion on der (22), led to further investigation, which showed that although BCR was relocated, it was a bystander to rearrangement of IGL. They commented that FISH as sole assay for BCR::ABL1 may be a diagnostic pitfall, especially when encountered in an entity not associated with the Ph chromosome (follicular lymphoma) [10].
Our two cases exhibited false positive karyotype findings. In the first, FISH analysis both on interphase and metaphase cells confirmed presence of Ph chromosome and absence of EVI1 rearrangement, which were consistent with the patient’s phenotypic CML. In the second, biclonality was present, with 25% of analyzed cells representing a sideline clone with t(9;22), however FISH did not demonstrate BCR::ABL1 rearrangement. Detection of Ph chromosome in this instance would be very unusual [11, 12].
These two cases were similar to the report by Wlodarska, et al. [10] in that chromosomal breakage and rearrangement, as evidenced by karyotype, corresponded to regions not associated with WHO-define recurrent abnormalities, and therefore not resolved by FISH probes specific to those abnormalities. Comparison of metaphase and interphase FISH did not change our results. Unknown breakpoints centromeric to EVI1 probe set and telomeric to probe regions for BCR::ABL1 are possible explanations of the results in case 1 and case 2, respectively; further characterization was not necessary. CGH would not detect the translocations and inversions present but might capture inapparent deletion or duplication, if present.
Neither of these false positive karyotype abnormalities existed as primary alterations. In case 1, inv(3)(q21q26.2) existed concurrently with t(9;22), and in case 2, the t(9;22) existed as a secondary abnormality along with deletions of 11q and 6q. The former case presents an obvious one to interrogate by FISH, as EVI1 rearrangement would confer a worse prognosis, while the latter presents more as a curiosity as t(9;22) yielding BCR::ABL1 in CLL/SLL would be highly unusual. The paucity of published reports of these type of discordances shows them to be uncommon and therefore an algorithm for addressing them is likely to see limited use. However, based on Cantú et al, metaphase (m) FISH may be a useful study when karyotype and interphase (i) FISH are discordant. As presented, i-FISH and m-FISH were useful studies to show that the conventional cytogenetic abnormality did not represent a WHO-defined recurrent abnormality.
Conclusion
Abnormal karyotypes, which may represent WHO- defined recurrent abnormalities with potential diagnostic, prognostic, or predictive implications, should be interrogated by FISH to avoid incorrect diagnoses or prognoses given the potential for false-positive karyotype results. Furthermore, because of the nature of malignant cells, both interphase and metaphase FISH analysis may be necessary to assess for definitional, predictive, or prognostic alterations seen, not seen, or poorly visualized by karyotype. Importantly, as presented here, chromosomal rearrangement involving regions corresponding to recurrent abnormalities with known disease associations need not necessarily involve the same break points with attendant dysregulation or novel fusion protein product. Not every t(9;22) yields the Ph chromosome, and inv(3) and t(3;3) do not invariably lead to EVI1 overexpression. Confirmation of WHO defined recurrent conventional cytogenetic abnormalities by orthogonal methods like FISH is necessary when possible to avoid false negative conventional chromosome rearrangements.
References
-
Smol T (2014) Inv(3)(Q21q26) RPN1/MECOMt(3;3) (Q21;Q26) RPN1/MECOMins(3;3)(Q26;Q21q26) RPN1/ MECOM. Atlas Genet Cytogenet Oncol Haematol.
-
Swerdlow SH (2017) WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. In: Swerdlow SH, et al. (Eds.), 4th (Edn.), International Agency for Research on Cancer.
-
Nikumbh DB, Wader JV, Kshirsagar VY, Desai SR, Jagtap SV, et al. (2012) Adult Type Chronic Myeloid Leukemia in Childhood: A Case Report. JKIMSU 1(1): 113-117.
-
Deininger MW, Shah NP, Altman JK, Berman E, Bhatia R, et al. (2021) Chronic Myeloid Leukemia. National Comprehensive Cancer Network.
-
Wierda WG, Byrd JC, Abramson JS, Bilgrami SF, Bociek G, et al. (2021) Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Version 4.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 18(2): 185-217.
-
He R, Wiktor AE, Hanson CA, Ketterling RP, Kurtin PJ, et al. (2015) Conventional karyotyping and fluorescence in situ hybridization: an effective utilization strategy in diagnostic adult acute myeloid leukemia. Am J Clin Pathol 143(6): 873-878.
-
Wheeler FC, Kim AS, Mosse CA, Shaver AC, Yenamandra A, et al. (2018) Limited Utility of Fluorescence in Situ Hybridization for Recurrent Abnormalities in Acute Myeloid Leukemia at Diagnosis and Follow-Up. Am J Clin Pathol (5): 418-424.
-
Cherry AM, Brockman SR, Paternoster SF, Hicks GA, Neuberg D (2003) Comparison of Interphase FISH and Metaphase Cytogenetics to Study Myelodysplastic Syndrome: An Eastern Cooperative Oncology Group (ECOG) Study. Leukemia Res 27(12): 1085-1090.
-
Cantú ES, Dong H, Forsyth DR, Espinoza FP, Papenhausen PR (2018) Discrepant Cytogenetic and Interphase Fluorescence In Sity (I-FISH) Results from Bone Marrow Specimens of Patients with Hematologic Neoplasms. Ann Clin Lab Sci 48(3): 264-272.
-
Wlodarska I, Pittaluga S, Stul M, Martiat P, Dierlamm J, et al. (1997) Philadelphia-like Translocation T(9;22) (Q34;Q11) Found in a Follicular Lymphoma Involving NotBCR And ABL ButIGL-Mediated Rearrangement of an Unknown Gene on 9q34. Genes Chromosomes Cancer 20(2): 113-119.
-
Jordan JMG, Hastings RJ, Moore S, International Standing Committee on Human Cytogenomic Nomenclature; S. Karger GmbH (2020) ISCN 2020 an International System for Human Cytogenomic Nomenclature (2020): Recommendations of the International Standing Committee on Human Cytogenomic Nomenclature Including Revised Sequence-Based Cytogenomic Nomenclature Developed in Collaboration with the Human Genome Variation Society (HGVS) Sequence Variant Description Working Group. Basel Freiburg Karger 2020.
-
Wieser R (2015) MECOM (Ecotropic Viral Integration Site 1 (EVI1) and Myelodysplastic Syndrome 1 (MDS1- EVI1). Atlas Genet Cytogenet Oncol Haematol.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet