Neuroendocrine Tumor of Cecum-Well Differentiated Intermediate Grade: G2 Presented with Aggressive Biologic Behavior: Case Report with Review
Neuroendocrine tumors (NETs) are relatively rare neoplasms of the gastrointestinal tract with variable clinical presentations. A 53 year old female presented with a chief complaint of intermittent right-sided abdominal pain, nausea, loose stools of and on of 8 month duration. The computed tomography of abdomen and pelvis, both plain and with contrast revealed the presence of a large well defined homogenously enhancing polypoidal mass lesion noted in the caecum measuring 2.8 X 2.6 X 2.8 cm in size. On colonoscopy revealed the presence of a polypiodal mass in the cecum measuring 3 cm with mucosal ulceration. The biopsy reported as suggestive of neuroendocrine tumor. The wide surgical resection of cecal mass with lymph node dissection was done. On histopatholgy reported as well differentiated neuroendocrine tumor, intermediate grade G2 of cecum with mesenteric lymph node metastasis. On clinical of stage III. The tumor was strong and diffusely positive for expression of synaptophysin and chromogranin A. The expression of the cell-cycle-associated Ki-67 antigen by MIB-1 monoclonal antibody was 3%. Herewith we are presenting rare case of well differentiated neuroendocrine tumor with intermediate grade or grade 2 of cecum with aggressive biologic behavior.
Jagtap Sunil V*, Jagtap Swati S , Mishra Shefali , Desai Neha , Shah Pranjal and Gaur Shuchita
Introduction
Neuroendocrine tumors are rare and can occur anywhere in the body. Most NETs occur in the lungs, appendix, small intestine, rectum, pancreas, breast, adrenal glands [1, 2]. Gastrointestinal NETs arise from neuroendocrine cells that are Kulchitsky cells or enterochromaffin cells distributed in the mucosa and submucosa of the gastrointestinal tract. The term NETs comprises WHO G1, G2 and rare G3 lesions [3]. This grading system is done on the proliferation rate, histologic features and the clinical behavior of the tumor. It is observed that the incidence of colorectal NETs has been continuously increasing over the past few decades. The pathologic diagnosis of NETs is important for patient further management. The biologic behavior of most functioning NETs is defined by the grade and stage of the tumor. The serum chromogranin A is the most common biomarker used to assess the disease and monitor treatment. Herewith
we reported a well differentiated neuroendocrine tumor, intermediate grade G2 of cecum with mesenteric lymph node metastasis.
Case Report
A 53 year old female presented to with a chief complaint of intermittent right-sided abdominal pain, nausea, vomiting, loose stools off and on of 8 month duration. She had anorexia and weight loss of 5 kg over the previous 6 month. She had history of altered bowel habit with occasional bloody diarrhea. Her medical history was not relevant. The systemic examination was normal. The computed tomography of abdomen and pelvis, both plain and with contrast revealed the presence of a large well defined homogenously enhancing polypoidal mass lesion noted in the caecum measuring 2.8 X 2.6 X 2.8 cm .The appendix was normal. The mild ascitis was noted. There was mild associated periserosal fat stranding nodularity with few enlarged lymph nodes in the right iliac fossa, largest measuring 1.8 x 1.1cm most likely suggestive of neoplastic lesion with metastatic lymph nodes. The radio imaging examination chest showed no evidence of any primary or metastatic pulmonary lesion. The patient was advised colonic biopsy and followed by histopathology examination.
Liver was mildly enlarged in size, no evidence of any metastasis. Hepatic and portal veins, gall bladder appear were normal. Pancreas, spleen, kidneys were normal in size, shape, attenuation and enhancement. On colonoscopy revealed the presence of a polypiodal mass in the cecum measuring 3 cm with mucosal ulceration. The exophytic mass extending from the cecum and occupying approximately 60% of the luminal circumference with wall thickening. The biopsy reported as suggestive of neuroendocrine tumor. The patient underwent a right hemicolectomy with local lymph node resection.
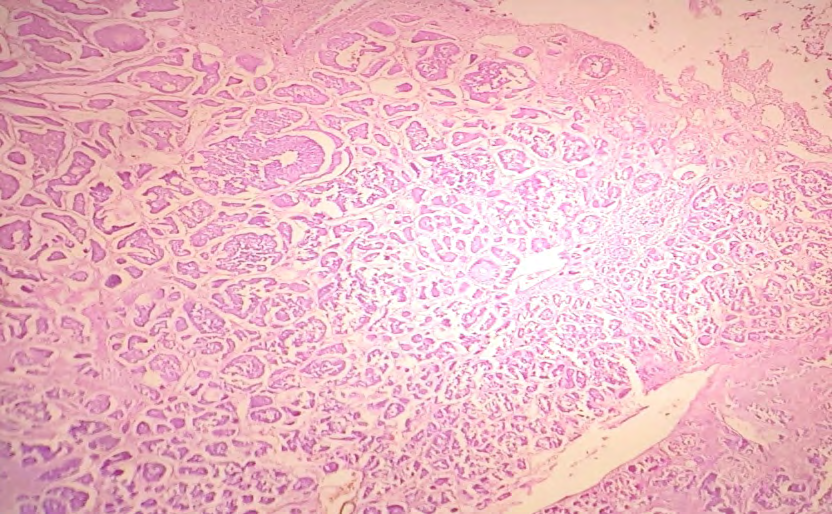
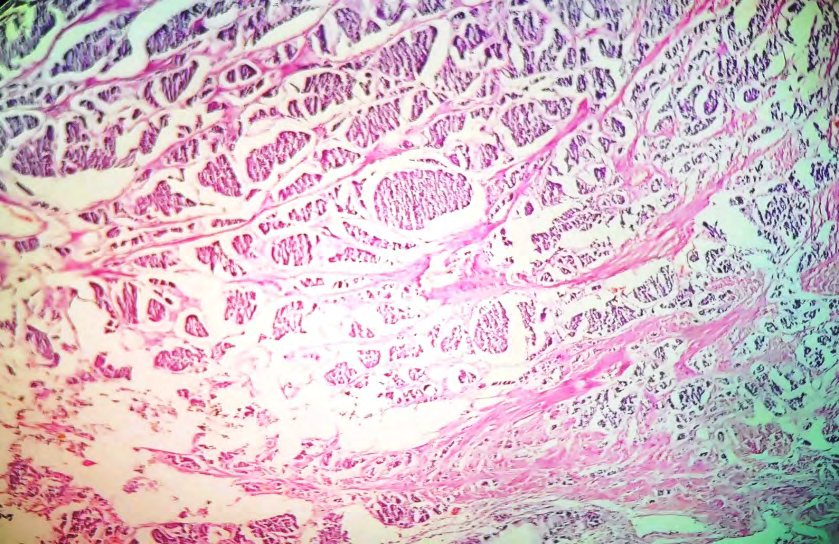
We received a hemicolectomy specimen totally measuring 32 cm in length. Ileum measured 16 cm in length and cut section appeared unremarkable. The cecum measured 11 x 8 x 3 cm. External surface showed thickening and adhesions. On cut open cecum showed a single circumscribed, polypoidal nodular submucosal tumor extending upto serosa measuring 3 cm in diameter. Cut section of tumor was tan yellow, fleshy and firm with focal area of hemorrhage (Figures 1 & 2). Tumor was 16 cm away from proximal margin (ileum) and 5 cm away from distal surgical margin (ascending colon). The ascending colon measures 5 cm in length and cut section of which appeared unremarkable. Attached appendix measures 5.2 cm in length and cut section of which appeared unremarkable. External surface at the level of tumor showed 2 lymph nodes. The cut section was grey white, firm.
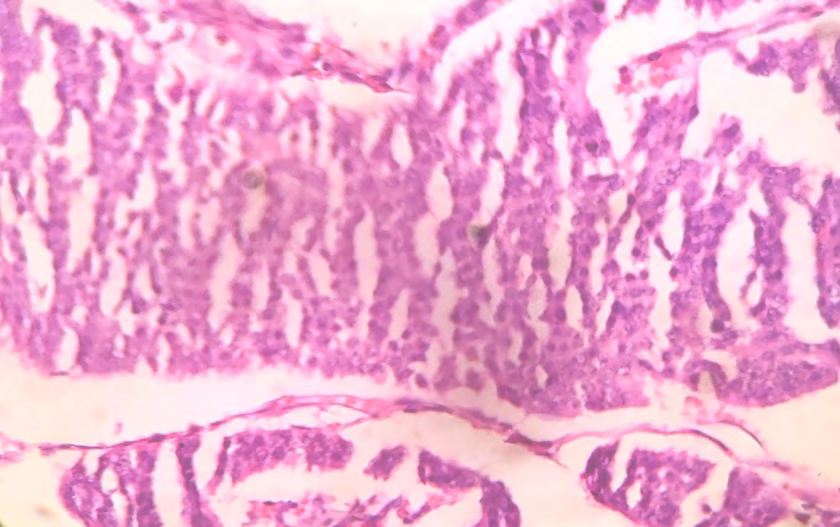
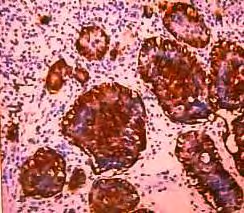
On microscopic showed wall of cecum, the submucosal tissue showed neoplastic cells arranged in various pattern organoid, solid growth, nests, trabecular and insular. Individual neoplastic cells were small, monotonous, regular cells with round or oval nuclei having salt and pepper chromatin and moderate eosinophilic granular cytoplasm (Figures 3 & 4). Tumor was located at muscularis mucosa and muscularis propria (Figure 5). The mesenteric lymph node showed evidence of metastesis. On histopathology reported as well differentiated neuroendocrine tumor of cecum with intermediate grade or grade 2 (G2): mitoses 4 - 20/2 mm2. The clinically of stage III. The tumor was strong and diffusely positive for expression of synaptophysin and chromogranin A (Figure 6). The expression of the cell-cycle-associated Ki- 67 antigen by MIB-1 monoclonal antibody was 3%.


Discussion
Neuroendocrine tumors were first described by Langhans T [4]. In 1907, Oberndofer first described these tumors arising from the epithelial cells in small intestine as “carcinoid”. Neuroendocrine tumors previously called carcinoid tumors are neoplasms of enterochromaffin or neuroendocrine cell origin. In 2000, the World Health Organization classification replaced “carcinoid” with the terms neuroendocrine tumors and neuroendocrine carcinomas to describe gastrointestinal neoplasms originating from the diffuse system of neuroendocrine cells [5]. The recently proposed consensus statement by the WHO and International Agency for Research on Cancer (IARC), the term “neuroendocrine neoplasm (NEN)” was adopted to provide a uniform classification. NENs consist of well differentiated NETs corresponding to Grade 1 (carcinoid- like) and Grade 2 (atypical carcinoid-like) tumors (regarded as carcinomas in the breast) and poorly differentiated NECs, represented by small-cell and large-cell carcinoma [6, 7].
The NETs incidence ranges from 2.5- 8.4 cases per lakh population [6]. The majority of NETs are nonfunctioning clinically and may remain asymptomatic or undetected. The age for colonic NETs mostly at 60 years [8]. In relation to increased awareness, improved diagnostic tools, early-stage detection, a specified definition of tumor histopathology, tumor biomarkers, and molecular markers, in the last decades the incidence has been rising. The functional hormone secreting neuroendocrine tumors are rare. They display neurosecretory capacity that may result in the carcinoid syndrome. MA Maggard, et al. [9], noted the most frequent locations of NETs in the gastrointestinal tract were the small bowel (44.7%) and the rectum (19.6%), and they account for only 10.6% in the colon [9]. The other study showed the most common site for NETs was stomach 27.5%, followed by duodenum 25%, colon 20%, esophagus 12.5%, appendix 10% ,ileum and rectum comprised 2.5% of the cases [10, 11]. The most common locations for NETs in the large intestine are rectum and cecum. The size of tumor is variable and usually larger tumors are seen in the proximal colon. In our case tumor was located in cecum having a size of 2.8 x 2.6 cm. NETs clinically presents with abdominal pain, anorexia, weight loss gastrointestinal bleeding, altered bowel habits, intestinal obstruction etc. Associated mesenteric fibrosis, nodal metastases, and desmoplastic reactions involving mesenteric vessels may lead to nonspecific abdominal pain, gastrointestinal bleeding, intermittent ischemia, or bowel obstruction [12]. A majority of NETs follows a benign course. In our case patient present intermittent right-sided abdominal pain, altered bowel habit with occasional bloody diarrhea, with regional metastases and mild acitis. Also in our case the tumor behavior was aggressive.
It is observed that the neuroendocrine carcinomas of the colon and rectum are very aggressive clinical course with poor prognosis as, by the time diagnosis is made distant metastases are often present. On histopathological examination tumor cells are arranged in nests, ribbons, trabecular, gyriform, and solid growth patterns. The tumor grows in submucosal site of intestine and gradually invades the overlying mucosa with ulceration formation. The tumor necrosis, angiolymphatic invasion, increased mitosis are noted. On microscopy the mitotic rates are expressed as the number of mitoses/2 mm² (the equivalent of 10 high power fields with ×40 magnification and a field of view of 0.5 mm.And tumor proliferation capacity is measured by Ki-67 staining with Ki-67 Index < 2% seen in grade -I tumors, 2%- 20% in grade II tumors, and > 20% tumor cell involvement in grade III GEP-NET [13]. Lymphatic invasion and WHO grade are independent predictive factors of lymph node metastasis.
The immunohistochemical study is required for confirmatory diagnosis and its behavior. The cells originating from the diffuse system of neuroendocrine cells within the gastrointestinal tract share phenotypic similarities with neural cells in their expression of synaptophysin, NSE, and chromogranin A. The laboratory values associated with neuroendocrine tumors shows raised chromogranin, serotonin, and its end product 5-HIAA. In our case synaptophysin, chromogranin A were positive. The expression of the cell-cycle-associated Ki-67 antigen by MIB- 1 monoclonal antibody was 3% in our case. The index might be useful for determining the prognosis for an individual because of the significant decrease in survival when the index is higher than 4%.
The treatment recommended for NETs are wide surgical resection with lymph node dissection. Srirajaskanthan R, et al. [14] stated that the therapies for management of metastatic patients with symptomatic functional NETs should be considered for somatostatin analog (short- or long-acting octreotide) or interferon- α therapy alone or in combination [14].
For colonic NETs staging is important to treat the patients. Modlin IM et al observed that the most ceacal NE tumors are > 2 cm in size with invasion into the muscularis propria at the time of diagnosis and overall prognosis is poor with 5-year survival rates of only 33%-42% [15]. In our case tumor was more than 2 cm and showed regional node metastesis. There is relationship between the size and the presence of metastasis, 85% of tumors of more than 2 cm metastasize [16]. The morbidity, and mortality dependent on tumor location, metastatic potential, and functional biologic status. The various treatment modalities include endoscopic resection, surgical resection, somatostatin analog therapy etc., Molecular targeted therapy with verolimus for the metastatic progressive NET of gastrointestinal tract is to be consider [17]. Immunotherapy will serve as a future treatment modality.
Conclusion
NETs are rare entities in the lower gastrointestinal tract. We are presenting rare case of well differentiated neuroendocrine tumor with intermediate grade or grade 2 of cecum with aggressive biologic behavior for its clinical, radiological, histopathological and immunohistochemical findings.
References
-
Kloppel G (2017) Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications. Visc Med 33: 324- 330.
-
Jagtap SV, Aher VC, Bhosale SJ, Hulwan A, Gosavi AN (2017) Primary neuroendocrine carcinoma of breast: An uncommen variant. Ann Pathol Lab Med 4(2): C50-52.
-
Rindi G, Klimstra DS, Ardekani AB, Asa SL, Bosman FT, et al. (2018) A common classification framework for neuroendocrine neoplasms: an International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod Pathol 31: 1770-1786.
-
Langhans T (1867) Ueber einen drusenpolyp im ileum Virchows Arch 38: 559-560.
-
Kloppel G, Perren A, Heitz PU (2004) The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci 1014: 13-27.
-
Dixit N, Trivedi S, Suri M (2021) Fine needle aspiration cytology of primary neuroendocrine tumor of the breast and it’s differential diagnosis. Diagnostic Cytopathology 49(1): 171-175.
-
Modlin IM, Oberg K, Chung DC, Jensen RT, Herder WW, et al. (2008) Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol 9(1): 61-72.
-
Jagtap SV, Khatib W, Hulwan A, Jagtap SS, Kulkarni SR (2016) Colorectal cancer: clinicohistopathological study at tertiary care hospital in Western Maharashtra. Biomed Rev: J Basic Appl Med Sci 3(2): 37-41.
-
Maggard MA, O Connell JB, Ko CY (2004) Updated population-based review of carcinoid tumors. Ann Surg 240(1): 117-122.
-
Abdullah H, Wani Z, Nabi Z, Shah P, Bhat S (2022) Neuroendocrine tumors of gastrointestinal tract with special reference to immunohistochemistry markers at a tertiary care hospital. APIK J Int Med 10(2): 78-85.
-
VD Dafle, A Das, SV Jagtap (2020) Clinico-pathological Study of Appendicectomy Specimens. Indian J Pathol Res Pract 9(1 Part II): 221-227.
-
Daskalakis K, Karakatsanis A, Stålberg P, Norlén O, Hellman P (2017) Clinical signs of fibrosis in small intestinal neuroendocrine tumours. Br J Surg 104(1): 69-75.
-
Oberg K, Jelic S (2009) Neuroendocrine gastroenteropancreatic tumors: ESMO clinical recommendation for diagnosis, treatment and follow- up. Ann Oncol 20 (S4): 150-153.
-
Srirajaskanthan R, Toumpanakis C, Meyer T, Caplin ME (2009) Review article: future therapies for management of metastatic gastroenteropancreatic. Aliment Pharmacol Ther 29(11): 1143-1154.
-
Modlin IM, Kidd M, Latich I, Zikusoka MN, Shapiro MD (2005) Current status of gastrointestinal carcinoids. Gastroenterology 128(6): 1717-1751.
-
Zúñiga D (2013) Tumores neuroendocrinos gastrointestinales. Medicina legal de Costa Rica 30(1): 89-98.
-
Yao JC, Fazio N, Singh S, et al. (2016) Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study. Lancet 387: 968-977.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet