Ripened and Revamped-Adult T Cell Leukaemia/ Lymphoma
Adult T cell leukaemia/ lymphoma is an aggressive T cell malignant disorder comprised of significantly pleomorphic, miniature to intermediate, mature CD4+ T cells. Factors such as demographic distribution within HTLV1 endemic zones, hypercalcemia, cutaneous lesions and a leukemic phase contribute to disease emergence. Adult T cell leukaemia/ lymphoma incriminates peripheral blood, lymph nodes, spleen, cutaneous surfaces, pulmonary or hepatic parenchyma, gastrointestinal tract and central nervous system. Bone marrow may demonstrate diffuse, interstitial or sinusoidal pattern of neoplastic occurrence. Generally, tumour cells are permeated with basophilic cytoplasm, absent intracytoplasmic granules, irregular or poly-lobulated nuclei with homogeneous, condensed nuclear chromatin and miniature nucleoli.
Editorial
Adult T cell leukaemia/ lymphoma is an aggressive T cell malignant disorder preponderantly comprised of widely disseminated, significantly pleomorphic, miniature to intermediate, mature CD4+ T cells. Cogent histological features as a pleomorphic T cell lymphoma, leukemic phase, CD4+ T cells with alpha/beta (αβ) subtype, T regulatory immuno-phenotype and CD25 expression appear indicative of adult T cell leukaemia/lymphoma.
The lymphoma exhibits a causal association with human T lymphotropic virus 1 (HTLV1) or human T cell leukaemia virus and may arise within endemic zones of HTLV1 wherein incriminated subjects are exposed to HTLV1 within early life and around ~ 2.5% individuals emerge as HTLV1 carriers.
The aggressive lymphoma requires segregation from a variety of HTLV1 associated neoplastic and non neoplastic disorders. T cell lymphoma occurring within endemic zones of HTLV1 may require distinction from acute T cell leukaemia/ lymphoma, irrespective of concordant histopathological features and outcomes of anti HTLV1 serological assay.
Additionally designated as adult T cell leukaemia, adult T cell lymphoma or adult T cell leukaemia / lymphoma (HTLV1+), neoplastic T lymphocytes enunciate monoclonal integration of HTLV1. As the lymphoma occurs within significant duration following infection and demonstrates an extended latent period, disease emergence is encountered within adults [1, 2].
As adult T cell leukaemia/ lymphoma demonstrates viral integration into neoplastic cells, factors such as appropriate demographic distribution within HTLV1 endemic zones, hypercalcemia, cutaneous lesions and a leukemic phase appear contributory to disease occurrence.
Adult T cell leukaemia/ lymphoma commonly emerges within third decade to ninth decade with mean age of disease emergence at 58 years. A male preponderance is observed with male to female proportion of ~1.5:1 [1, 2].
Cogent disease transmission mandates the presence of viable, HTLV1 infected T cells. The condition may be transmitted from mother to infant, preponderantly through lymphocytes amalgamated within breast milk. Besides, blood or blood products, except fresh frozen plasma and vaginal, prostatic or seminal secretions may transmit the disease.
Adult T cell leukaemia/ lymphoma preponderantly exemplifies disseminated lymph node involvement. Systemic organs as spleen or extra-nodal sites as cutaneous surfaces, pulmonary or hepatic parenchyma, gastrointestinal tract and central nervous system may be implicated. Generally, extra- nodal sites as cutaneous surfaces(> 50%) and peripheral blood are principally incriminated [1, 2].
Adult T cell leukaemia / lymphoma demonstrates cellular origin of peripheral CD4+ T regulatory alpha/beta (αβ) T cells wherein CD4+ CD25+ FoxP3+ T regulatory cells configure as the normal counterpart. Incriminated subjects manifest with profound immunodeficiency as the T regulatory T cell of origin is contemplated to induce disease associated immunodeficiency [1, 2].
Generally, adult T cell leukaemia/ lymphoma exhibits causal, infective association with human T lymphotropic virus (HTLV1), a type C human retrovirus of delta- retrovirus genus. The monoclonal, single stranded, RNA virus configures double stranded DNA through reverse transcriptase enzyme and randomly integrates into host cell genome. Nevertheless, singular viral infection is inadequate for neoplastic transformation.
HTLV1 infects immature thymocytes and mature CD4+ T cells, invades through cell to cell contact in concurrence with cellular molecules as neuropilin1, heparan sulfate proteoglycan (HSPG) and glucose transporter 1(GLUT1) [1, 2].
Tax protein and HTLV1 basic leucine zipper factor (HBZ) are preponderant oncoproteins which induce adult T cell leukaemia/ lymphoma in subjects with chronic infection. TAX (p40) activates viral promoter and configures cyclic AMP response element binding transcription factor (CREB) along with nuclear factor kappa B(NFκβ) pathways. HBZ is consistently exemplified in adult T cell leukaemia/ lymphoma and contributes to cellular proliferation with survival of neoplastic clone of cells. Besides, epigenetic alterations and hyper-methylation contribute to disease emergence and progression [1, 2]. As per established Shimoyama classification, adult T cell leukaemia/ lymphoma manifests with distinct clinical variants denominated as • Acute variant which configures ~55% to 60% instances and enunciates ~leucocytosis ≥100 x 109/litre ~peripheral blood involvement with dissemination of innumerable ‘flower cells’ ~cutaneous rash and lymphadenopathy ~hepatosplenomegaly ~hypercalcemia ~elevated levels of serum lactate dehydrogenase (LDH) ~rapidly progressive clinical course, frequently associated opportunistic infections and inferior prognostic outcomes with overall survival < 1 year [2, 3].
- Lymphomatous variant represents ~ 20% instances and demonstrates ~lymph node enlargement ~cutaneous lesions ~absent or minimal incrimination of peripheral blood ~hypercalcemia is infrequent, in contrast to adult variant ~overall survival < 1 year [2, 3].
- Chronic variant represents ~ 15% to 20% instances and enunciates ~lymphocytosis ~lymphocyte count is decimated, in contrast to acute variant ~exfoliative cutaneous lesions ~few atypical lymphocytes discernible within peripheral blood smear ~mild hepatosplenomegaly ~mild regional lymph node enlargement ~absence of hypercalcemia ~disease progression towards adult or lymphomatous stage with overall survival > 2 years and < 5 years [2, 3].
- Smouldering variant configures ~ 5% instances and manifests ~disease progression towards adult T cell leukaemia/ lymphoma or infectious complications with overall survival > 2 years and < 10 years ~cutaneous lesions or lesions confined to pulmonary parenchyma ~>5% circulating atypical lymphocytes in the absence of leucocytosis ~absence of hepatosplenomegaly, hypercalcemia or lymph node enlargement [2, 3].
- Primary cutaneous tumoral subtype lacks a distinct leukemic phase, lymphadenopathy, hepatosplenomegaly or hypercalcemia.
- Non neoplastic human T lymphotropic virus 1(HTLV1) associated disease is contemplated as an additional variant and is comprised of ~tropical spastic paraparesis (TSP) or HTLV1 associated myelopathy (HAM) ~HTLV1 associated infective dermatitis ~uveitis ~thyroiditis ~pneumonitis ~myositis[2, 3].
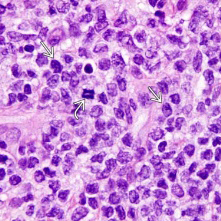
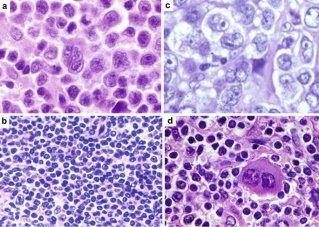
Cytological examination demonstrates a variable countenance of neoplastic cells wherein tumour cells are permeated with basophilic cytoplasm devoid of intracytoplasmic granules, irregular or poly-lobulated nuclei with homogeneous, condensed nuclear chromatin and miniature nucleoli. Neoplastic cells invading regional lymph nodes are frequently pleomorphic and the infiltrate may be comprised of an admixture of miniature to enlarged, pleomorphic cells [2, 3].
Peripheral blood smear exhibits medium to enlarged neoplastic lymphocytes pervaded with multi-lobulated nuclei, configuring ‘flower cells’ which characteristically circulate within leukemic phase of adult T cell leukaemia/ lymphoma. In contrast to peripheral blood lymphocytes, neoplastic lymphocytes are mildly enlarged and imbued with scant, basophilic cytoplasm, moderately condensed nuclear chromatin and absent or miniature nucleoli. Chronic instances of adult T cell leukaemia /lymphoma may demonstrate neoplastic cells pervaded with multi-lobulated nuclei [2, 3].
Upon gross examination, cutaneous lesions are categorized as erythema, papules or nodules. Tumour- like lesions or erythroderma simulating mycosis fungoides / Sézary syndrome is exceptionally discerned. Regional lymph nodes appear enlarged and demonstrate complete effacement of lymph node architecture [2, 3].
• Upon microscopy Bone marrow demonstrates minimal proportionate bone marrow infiltration, in concurrence with discernible significant lymphocytosis. Incrimination of bone marrow may be diffuse, interstitial or sinusoidal. Neoplastic infiltration is frequently associated with resorption of adjacent bone, prominent osteoclastic activity and remodelled bone trabeculae. Lytic bone lesions may appear in the absence of neoplastic bone infiltration.
• Regional lymph nodes display incrimination of paracortical T cell zones [2, 3]. Lymph node architecture is diffusely effaced. Tumour occurrence within regional lymph nodes is categorized pertaining to infiltrative pattern and cellular subtype into ~pleomorphic small cell ~pleomorphic medium and enlarged cell, is commonly discerned ~anaplastic large cell-like, simulating anaplastic large cell lymphoma (ALCL) ~angioimmunoblastic T cell lymphoma- like (AITL) configuration ~Hodgkin’s lymphoma-like articulation is encountered within preliminary phase of certain adult T cell lymphomas ~leukemic pattern of infiltration enunciates preservation or distention of lymph node sinuses imbued with malignant cells [2, 3].
However, clinical course remains impervious to factors such as tumour cell magnitude and outline or precise identification and classification of aforesaid neoplastic configurations.
Cutaneous lesions manifest with neoplastic lymphocytes invading superimposed epidermis with frequent configuration of Pautrier-like micro-abscesses. Infiltration of superimposed epidermis is predominantly perivascular although tumour nodules may extend into subcutaneous adipose tissue. Besides, superimposed epidermis delineates variable hyperkeratosis and parakeratosis. ~erythematous lesions appear configured of miniature cells and delineate a perivascular pattern of tumour dissemination confined to subjacent dermis.
~papules and nodules are pervaded with enlarged cells which invade subjacent dermis •central nervous system, spleen or hepatic and pulmonary parenchyma are frequent and additional sites incriminated with adult T cell leukaemia/ lymphoma [2, 3].
Adult T cell leukaemia/ lymphoma is devoid of precise grading system[2, 4] (Figures 1 & 2). Ultrastructural examination delineates intracytoplasmic and extracellular viral particles of 80 nanometres to 120 nanometres magnitude [2, 4] (Table 1).
| Clinical manifestation | Acute | Lymphomatous | Smouldering | Chronic |
|---|---|---|---|---|
| Lymphocytosis | Increased | Normal | Normal | Mildly increased |
| Aberrant circulating lymphocytes | Increased | May be absent or delayed | >5% | Mildly increased |
| Increased LDH | Present | Absent | Absent | Minimal |
| Hypercalcemia | Present | Variable | Absent | Absent |
| Skin rash | Variable>50% | Variable> 50% | Erythematous rash | Rash, papules |
| Lymphadenopathy | Present | Present | Absent | Mild |
| Hepatosplenomegaly | Present | Present | Absent | Mild |
| Bone marrow infiltration | May appear | Absent | Absent | Absent |
| Median survival | <1 year | <1 year | >2 years | >2 years |
Table 1: Clinical variants of adult T cell leukaemia/lymphoma [3,4].
LDH: lactate dehydrogenase. Table 1: Clinical variants of adult T cell leukaemia/lymphoma [3, 4].
Adult T cell leukaemia/lymphoma appears immune reactive to CD2, CD3, CD4, CD5, CD25(IL-2R), T cell receptor alpha/beta(TCR-αβ), CD45RO, HLA-DR, FOXP3, CD52, CD62 / selectin L and CCR4. Besides, IRF4 / MUM1 is frequently expressed. Enlarged, transformed neoplastic cells appear intensely and diffusely immune reactive to CD30. Epstein Barr virus (EBV+) expressing reactive B lymphocytes or immunoblasts may appear commingled with the neoplastic infiltrate [4, 5]. Adult T cell leukaemia/lymphoma appears immune non reactive to CD7, CD8, terminal deoxynucleotidyl transferase(TdT), T cell leukaemia/lymphoma protein 1 (TCL1), anaplastic lymphoma kinase 1 (ALK1), B cell antigens as surface immunoglobulin with heavy chains and light chains as kappa or lambda with associated CD79a / CD79b complex , cytotoxic molecules or myeloid associated antigens [4, 5].
Upon flow cytometry, adult T cell leukaemia/lymphoma is contemplated to emerge from mature T cells delineating CD2+, CD3+, CD5+, CD45RO+, T cell receptor alpha/beta(TCR αβ+), CD1a-, CD7-, CD10- or PD-1- immuno-phenotype.
Majority (~ 90%) of instances delineate CD4+/ CD8- immuno-phenotype. Exceptional instances may enunciate CD4-/CD8+ or CD4+/CD8+ immuno-phenotype [4, 5]. Cytogenetic evaluation exhibits clonal integration of HTLV1 genome within host cell genome. Polymerase chain reaction (PCR) enunciates clonal T cell receptor genetic rearrangements. Upon quantitative assessment, HTLV1 levels appear elevated. Genetic mutations of CCR4 gene (25%) and RHOA gene (~15%) are encountered.
Tumour suppressor genes appear inactivated due to chromosomal mutation or epigenetic silencing. Several complex chromosomal anomalies are frequent, especially within acute and lymphomatous variants. Also, non specific clonal chromosomal anomalies may frequently appear [4, 5]. Adult T cell leukaemia/ lymphoma requires segregation from neoplasms such as peripheral T cell lymphoma not otherwise specified(NOS), angioimmunoblastic T cell lymphoma, anaplastic large cell lymphoma, classic Hodgkin’s lymphoma, cutaneous T cell lymphoma, mycosis fungoides, T cell prolymphocytic leukaemia, T cell lymphoblastic leukaemia/ lymphoma or T cell large granular lymphocytic leukaemia [4, 5].
Molecular assessment exhibits evident HTLV1 or HTLV2 genomic sequences. Anti-HTLV1 antibody may be employed as a surrogate for demonstration of monoclonal integration of viral particles. Aforesaid assay is beneficial in evaluating HTLV1 infection within zones of minimal prevalence. Besides, disease emergence within endemic areas expressing elevated HTLV1 prevalence necessitate demonstrable evidence of viral integration. Neoplastic T cell express CD25 [4, 5].
Additionally, parameters such as ~complete blood count exemplifies elevated leukocyte count and circulating neoplastic lymphocytes within the leukemic phase ~elevated serum lactate dehydrogenase (LDH) levels appear indicative of tumour burden or disease activity ~hypercalcemia is commonly discerned within acute variant and is variably accompanied by lytic bone lesions ~eosinophilia and neutrophilia appear frequently ~elevated soluble interleukin 2 (IL2) receptor α chain levels ensue within aggressive adult T cell leukaemia/lymphoma [4, 5].
Radiographic examination delineates lytic bone lesions preponderantly confined to cranium, pelvis, spine and long bones wherein ‘punched out’ lesions, akin to plasma cell myeloma can be discerned. ¹⁸F- fluoro-deoxy-glucose positron emission computerized tomography (¹⁸F-FDG/ PET/ CT) aids in discerning sites of disease activity. Computerized tomography (CT) is optimal for localizing nodal or extra-nodal disease [4, 5]. Asymptomatic instances of chronic or smouldering adult T cell leukaemia/ lymphoma may be managed with simple observation.
Adult T cell leukaemia/ lymphoma appears resistant to majority of chemotherapeutic agents and standardized, recommended chemotherapy regimen are absent. Nevertheless, intensive combination chemotherapy and bone marrow transplantation may be beneficially employed.
Monoclonal, antibody based therapies against molecules such as interleukin 2R (IL-2R or anti-Tac), mogamulizumab (CCR4) and alemtuzumab (CD52) may be adopted to treat adult T cell leukaemia/lymphoma.
Contemporary clinical trials with arsenic trioxide, interferon α and zidovudine may provide advantageous outcomes [4, 5]. Prognostic outcomes of adult T cell leukaemia/ lymphoma appear contingent to diverse, preponderant contributory factors as clinical variant, age of incriminated subject, performance status as per Eastern Cooperative Oncology Group (ECOG) scale and serum calcium or lactate dehydrogenase (LDH) levels. Disease associated mortality ensues due to occurrence of opportunistic infections. Acute and lymphomatous variants delineate an aggressive clinical course with reoccurring viral or parasitic infections as with Strongyloides stercoralis [4, 5].
Leukaemia/lymphomas demonstrating p16 genetic deletion or p53 genomic mutation enunciate an aggressive clinical course. Chronic and smouldering variants exhibit a protracted clinical course with disease progression into acute phase and an aggressive clinical course within ~25% instances. The variants are associated with p16 genetic deletion and various chromosomal deletions. Aforesaid genomic deletions occurring within chronic variant may be discerned through comparative genomic hybridization (CGH) and configures as an inferior prognostic factor [4, 5].
Conclusion
Adult T cell leukaemia/lymphoma appears immune reactive to CD2, CD3, CD4, CD5, CD25(IL-2R), T cell receptor alpha/beta(TCR-αβ), CD45RO, HLA-DR, FOXP3, CD52, CD62 / selectin L, CCR4 and IRF4 / MUM1. Neoplastic cells appear immune non reactive to CD7, CD8, terminal deoxynucleotidyl transferase(TdT), T cell leukaemia/lymphoma protein 1 (TCL1), anaplastic lymphoma kinase 1 (ALK1), B cell antigens as surface immunoglobulin with heavy chains and light chains as kappa or lambda with associated CD79a / CD79b complex , cytotoxic molecules or myeloid associated antigens. Adult T cell leukaemia/ lymphoma requires segregation from neoplasms such as peripheral T cell lymphoma not otherwise specified(NOS), angioimmunoblastic T cell lymphoma, anaplastic large cell lymphoma, classic Hodgkin’s lymphoma, cutaneous T cell lymphoma, mycosis fungoides, T cell prolymphocytic leukaemia, T cell lymphoblastic leukaemia/ lymphoma or T cell large granular lymphocytic leukaemia. Radiographic examination delineates ‘punched out’ lytic bone lesions preponderantly confined to cranium, pelvis, spine and long bones. Monoclonal, antibody based therapies against molecules such as interleukin 2R (IL-2R or anti-Tac), mogamulizumab (CCR4) and alemtuzumab (CD52) may be beneficially adopted to treat adult T cell leukaemia/ lymphoma.
References
-
Wolf S, Vercruyssen M, Cook L (2022) HTLV-1-related adult T-cell leukemia/lymphoma: insights in early detection and management. Curr Opin Oncol 34(5): 446- 453.
-
Durer C, Babiker HM (2022) Adult T Cell Leukemia. Stat Pearls International Treasure Island Florida.
-
Shimoyama M (1984) Diagnostic criteria and classification of clinical subtypes of adult T-cell leukaemia-lymphoma A report from the Lymphoma Study Group. Br J Haematol 79(3): 428-437.
-
Oliveira PD, Ribeiro GS, Anjos RO, Maria Almeida Dias, Lourdes Farre, et al. (2022) The importance of the clinical classification of adult T-cell leukemia/lymphoma (ATLL) in the prognosis. PLoS Negl Trop Dis 16(10): e0010807.
-
Kogure Y, Kameda T, Koya J, Yoshimitsu M, Nosaka K, et al. (2022) Whole-genome landscape of adult T-cell leukemia/lymphoma. Blood 139(7): 967-982.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet