Serpentine Aneurysm of the Placenta with Good Fetal Outcome
We report an exceedingly rare case of placental serpentine aneurysm. A 21-year-old gravida 3 para 1-0-1-1 with the history of a prior C-section presented at 35 weeks of gestation with the complaint of decreasing or absent fetal movements, previously there were no complications during her pregnancy. She underwent an emergent C-section due to non-reassuring fetal heart tones and delivered a female infant weighing 2145 grams without malformation and Apgar scores of 6 and 8 at 1 and 5 minutes. The premature neonate was admitted to the neonatal intensive care unit (NICU) and was discharged a few days later in good health and has done well since. The placenta weighed 768 grams with a three-vessel umbilical cord. The fetal surface was blue-gray and had multiple markedly dilated tortuous vessels (ranging in diameter from 0.5-1.4 cm) which were attached to a single area on the fetal surface. A Verhoeff-Van Gieson stain was negative for elastic fibers. The placental disc had a 7.1 cm peripheral infarct involving approximately 10% of the disc. There have been 3 cases reported previously in which two were associated with intrauterine growth restriction and one with molar transformation. In conclusion, placental serpentine aneurysm is a rare finding and unlike prior cases was associated with prematurity, decreased fetal movements, and nonreassuring fetal heart tones; a good outcome occurred because of prompt medical intervention.
Introduction
The successful development of placental vasculature plays a critical role in fetal development and growth and any abnormality in the umbilical or chorionic vasculature may significantly affect fetal development [1, 2]. Despite the many differences in the structure of placental and umbilical cord vessels aneurysms are very uncommon and may cause critical complications. We report a case of serpentine aneurysms of placental surface vessels associated with prematurity and decreased fetal movement in an otherwise normally developed neonate.
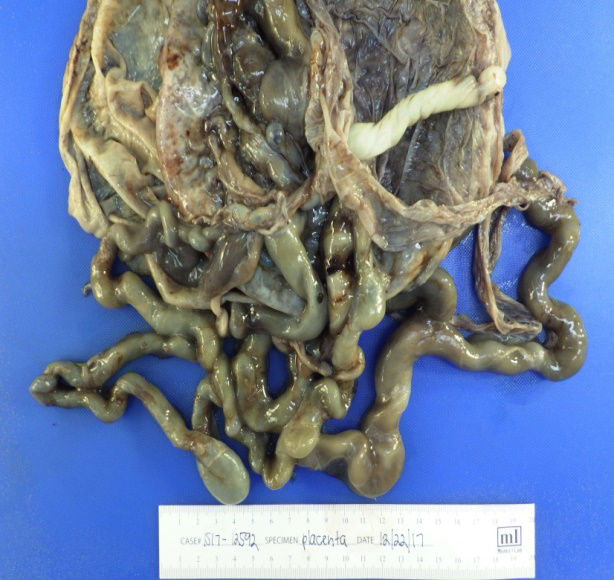
A 21-year-old gravida 3, para 1-0-1-1, with a history of a prior C-section presented to the emergency department at 35 weeks of gestation with the complaint of decreased to absent fetal movement. She subsequently underwent an emergent low transverse C section due to non-reassuring fetal heart tones. The placenta weighed 768 grams with a normal three-vessel umbilical cord. The fetal surface was blue-gray and had multiple markedly dilated tortuous vessels (ranging in diameter from 0.5-1.4 cm) which were attached to a single area on the fetal surface. A Verhoeff-Van Gieson
stain was negative for elastic fibers. The placental disc had a 7.1 cm peripheral infarct involving approximately 10% of the disc. The premature female neonate weighed 2145 grams with Apgar scores of 6 and 8 at 1 and 5 minutes and was admitted to the neonatal intensive care unit for a few days. No congenital abnormalities were found and she was discharged in good health and has done well since (Figure 1).
Discussion
Similarly, to the umbilical cord, aneurysms may occur in chorionic vessels. Dilation of vessels has been previously reported; Lee, Chi, and Cha reported a case with dilation of the chorionic vessels arising from the umbilical vein with an otherwise normal umbilical cord which was accompanied by placentomegaly. They described growth restriction and anemia in the neonate because of membranous insertion of the cord2. Also, Kaido, et al. [3].
Reported a case with placentomegaly and markedly dilated chorionic vessels with an infant with no abnormalities; however, the mother developed hypotension, anemia, and DIC requiring blood transfusion3. Lemtis presented the most extensive study of placental aneurysms, finding them in as often as 2.5% of placentas, and reported serpentine as the least frequent type of placental aneurysms. Lemtis also reported intrauterine growth restriction as the most common fetal consequence of placental aneurysms [4]. Zhang and Benirschke presented two cases of placental aneurysms, one associated with severe intrauterine growth restriction and fetal thrombocytopenia and the other case was associated with molar transformation of placental villous tissue. Which was similar to the case reported by Lemtis [5]. Whereas in our case the premature neonate was discharged a few days after admission to the NICU without any complications. McDermott and Gillan showed that reduced fetal blood flow may lead to placental infarction and showed it as the mechanism of infarction in the placenta [6], however, in our case while placental infarction was present, we can only speculate on its cause.
Conclusion
In conclusion, placental serpentine aneurysm is a very rare pathologic finding and has previously been reported as being associated with fetal and infant consequences including intrauterine growth restriction, and thrombocytopenia; our case demonstrated the adverse consequences of fetal distress which if promptly recognized may result in a good outcome.
References
-
Benirschke K, Burton G, Baergen RN (2012) Pathology of Human Placenta. 7th (Edn.), Springer 351-354.
-
Lee GK, Chi JG, Cha KS (1991) An unusual venous anomaly of the placenta. Am J Clin Pathol Jan 95(1): 48-51.
-
Kaido Y, Sugiyama T (2014) Unusual markedly-dilated chorionic vessels with placentomegaly. Springerplus 3: 146.
-
Lemtis H (1969) The disturbance of the feto-placental blood circulation and its significance. Arch Gynecol 207: 59-60.
-
Zhang P, Benirschke K (2000) Placental pathology casebook. Serpentine aneurysms of the placenta with fetal consequences J Perinatol 20(1): 63-65.
-
McDermott M, Gillan JE (1995) Chronic reduction in fetal blood flow is associated with placental infarction. Placenta 16(2): 165-170.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet