Mesenteric Mesothelial Cyst Presented as Acute Abdominal Pain
Mesenteric cysts are rare intra-abdominal tumors. The preoperative diagnosis of mesenteric cysts is challenging due to its rarity. We present a case of 65 -years-old female with history of progressive increasing abdominal discomfort and swelling she presented with sudden acute abdominal pain of 5 days. Physical examination revealed a mildly tender, palpable abdominal swelling occupying right iliac fossa measuring 10x8x3 cm. Plain and contrast computed tomography scan abdomen and pelvis showed an intra-abdominal well defined, thin walled cystic lesion in right iliac fossa and extending upto right hypochondriac region. It showed multiple thin internal septae and low level mobile internal echoes. On radio imaging suggestive of a mesenteric cyst was given and histopathological correlation was advised. The exploratory laprotomy with complete surgical excisions of cystic mass was done. The histopathological diagnosis of benign mesothelial cyst of mesentry was given. We are presenting rare case of simple mesenteric cyst for its clinical, radio imaging and histomorphological features.
Introduction
The mesenteric mesothelial cyst is defined as any cyst located in the mesentery lined by mesothelial cell with thin walls, may with focal calcifications. It may extend into the retroperitoneum [1]. The mesenteric cysts are benign lesions. There is no solid nodules or any atypia. It is considered that mesothelial cysts are caused by incomplete fusion of mesothelial layers. The preoperative diagnosis of mesenteric cysts is challenging due to rarity, lack of specific clinical symptoms and variability in location and size.
The mesenteric cysts are rare benign intra- abdominal tumours with an incidence of 1 case per 250,000 hospital admission [2].
Mesenteric cysts should properly assessed with a complete medical history, clinical examination, radiological investigations and confirmatory pathological diagnosis. We present herewith a case of large mesothelial cyst for its clinical, radio imaging and histomorphological features.
We present a case of 65-years-female with history of progressive increasing abdominal discomfort and swelling of 2 months duration. She presented with acute abdominal pain of 5 days with vomiting. Physical examination revealed a palpable abdominal swelling occupying right iliac fossa measuring 10 x 8 x 3 cm. Other systemic examinations were unremarkable.
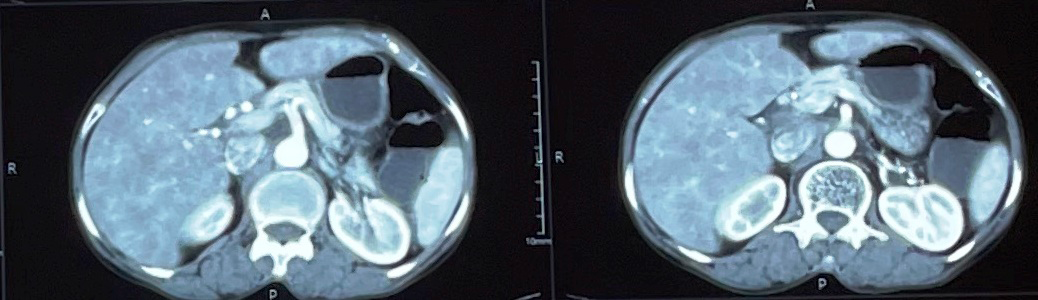
Plain and contrast Computed tomography (CT) scan abdomen and pelvis was done .It showed an intra-abdominal well defined, thin walled cystic lesion in right iliac fossa and extending upto right hypochondriac region (Figure 1). The cyst measuring 13.3 x 9.9.2 x 8.6 cm. It shows multiple thin internal septae and low level mobile internal echoes. It’s approximate volume was 597 ml. Mild overlying probe tenderness was present. No obvious solid mural nodule was seen. No evidence of any calcification. The lesion was seen in the displacing the surrounding small and large bowel loops without any infiltration. There was no surrounding inflammation. There was no significant lymphadenopathy. The right ovary could be seen separately from the mentioned cyst, and the appendix appears normal. Possibility of large mesenteric cyst wasgiven and histopathological correlation was advised. The exploratory laprotomy with complete surgical excisions of cystic mass was done.
Plain and contrast Computed tomography (CT) scan abdomen and pelvis was done .It showed an intra-abdominal well defined, thin walled cystic lesion in right iliac fossa and extending upto right hypochondriac region (Figure 1). The cyst measuring 13.3 x 9.9.2 x 8.6 cm. It shows multiple thin internal septae and low level mobile internal echoes.
It’s approximate volume was 597 ml. Mild overlying probe tenderness was present. No obvious solid mural nodule was seen. No evidence of any calcification. The lesion was seen in the displacing the surrounding small and large bowel loops without any infiltration. There was no surrounding inflammation. There was no significant lymphadenopathy. The right ovary could be seen separately from the mentioned cyst, and the appendix appears normal. Possibility of large mesenteric cyst was given and histopathological correlation was advised. The exploratory laprotomy with complete surgical excisions of cystic mass was done.
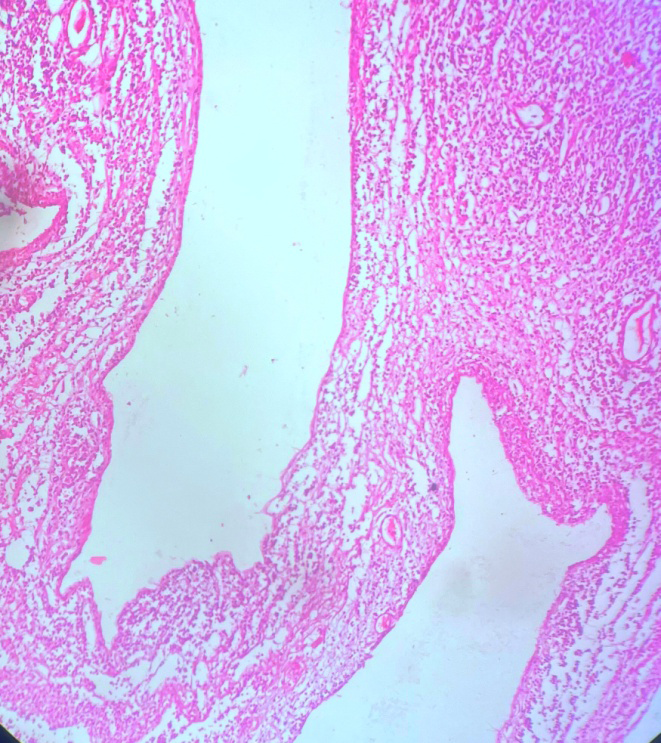
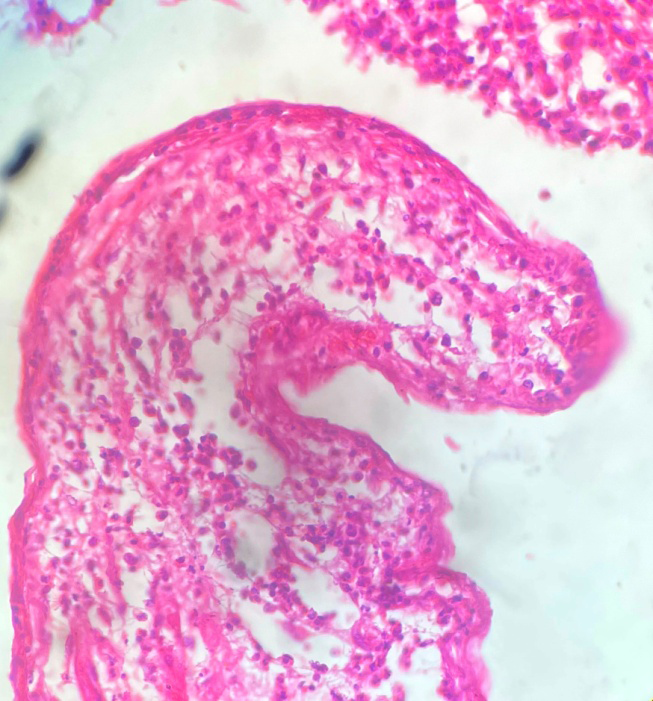
On gross, we received a cyst which was round to ovoid, measuring 12.5 x 9.9 x8.0 cm with smooth external surface. On cut open showed a large cyst with thin wall and multiloculations (Figure 2). It was filled with serous fluid and at places showed fibrinous exudate. On histopatholgy showed a cyst lined with a single layer of cuboidal epithelial cells, The lumen was filled with eosinophilic material with scant inflammatory cells and red blood cells (Figures 3 & 4). The wall lack smooth muscle and lymphatic spaces. The histopathological diagnosis of simple mesothelial cyst of mesentery was given. The patient had an uneventful postoperative recovery.

Mesenteric cyst can occur anywhere in the mesentery of gastrointestinal tract from duodenum to rectum. In a review series of 162 patients, 60% of mesenteric cysts occurred in the small-bowel mesentery, 24% in the large-bowel mesentery, and 14.5% in the retroperitoneum while it was indefinite in 1.5% of cases [3].
The origin of the cyst is related to congenitally malformed or malpositioned lymphatic tissue, secondary to trauma, degenerating lymph nodes or a failure of the mesentery to fuse properly etc [4].
Depending on their size and location, these cysts are often asymptomatic and are incidentally detected during routine imaging. The clinical manifestations are extremely varied. The patient may present clinically with abdominal pain, distention, fever, emesis, etc. The smaller mesenteric cysts are frequently mobile on abdominal palpation. The study by Prakash A, et al observed variable symptoms these are abdominal pain (82%), nausea and vomiting (45%), constipation (27%), and diarrhoea (6%). An abdominal mass may be palpable in up to 61% of patients [5]. In our case patient presented with acute abdomen with palpable mass. The histopathological classification is by the inner cyst wall layer cell and origin. The Perrot classification, which is used to classify cystic derivatives, indicates that the simple mesothelial cyst is a benign mesenteric mesothelial cyst. Perrot and coauthors proposed to classify cysts according to histopathological features and origin into six groups: lymphatic, mesothelial, intestinal, urogenital, dermoid cysts, and nonpancreatic pseudocystic origins. These mesenteric cysts can be walled off infections, neoplastic cells [1].
On gross mesenteric cysts can be simple, single or multiple, unilocular or multilocular, and they may contain hemorrhagic, serous, chylous, or infected fluid. Mesenteric cysts are most commonly single and multil oculated and contains serous fluid. Mesenteric cysts vary in size from few mm to 25 cm, filling the entire peritoneal cavity [1].
Mesenteric cyst should be evaluated with radiological investigations to reach a provisional diagnosis. The diagnosis is proven on laparotomy and has to be histologically confirmed. The recent imaging studies can determine the origin of cystic lesions within the abdominal cavity related to omental, mesenteric, or organ. Mesenteric cyst on plain radiographs of the abdomen demonstrate a homogeneous, water-density mass that displaces bowel loops. On ultrasound demonstrates an intra-abdominal cystic mass with thin septation, the wall may shows fine calcifications. The Magnetic resonance imaging or Computed tomography scan may define the anatomical margins of the cyst more precisely [6].
Histological classification depeding on the cyst lining are a) mesothelium-lined i.e., simple mesothelial cyst and neoplastic are benign cystic mesothelioma, and malignant cystic mesothelioma, b) endothelium-lined i.e wchylolymphatic mesenteric cyst or cystic lymphangioma c) cuboidal or squamous lined i,e mature cystic teratoma or dermoid cysts d) urogenital- urachal cyst. e) epithelium- lined enteric duplication cyst or enteric cyst and F) fluid collections with no cellular lining, such as infectious cyst, traumatic cysts nonpancreatic pseudocysts.
The differentiation from ovarian cyst, meconium pseudocyst, urachal cyst, and various cystic neoplasms of mesentery peritoneum are required [7, 8, 9]. The differentiation from intestinal duplication cysts from mesenteric cyst is required. The intestinal duplication cysts have a common blood supply and muscular layer with the adjacent bowel and have a well-defined mucosal layer. In our case diagnosis was simple mesothelial cyst lined by cubiodal mesothelium without any atypia. Tan JJY, et al observed various complications of mesenteric cysts are cyst rupture, infection, hemorrhage, intestinal obstruction, volvulus, peritonitis, shock, hemorrhage and death. But these complications are rare [10]. Malignant cysts occur in less than 3% of cases [3].
The complete surgical excisions, by either open or laparoscopic approach ensures the lowest risk of recurrence. In large cysts internal drainage of the cyst into the peritoneal cavity has also been successfully used in the treatment [10].
The prognosis for mesenteric cysts is good because most are benign and the recurrence rate is low with complete excision.
Conclusion
We are presenting rare case of simple mesenteric cyst for its clinical, radio imaging and histomorphological features.
Mesenteric cysts represent a diagnostic challenge. Mesenteric cysts should always be assessed with a proper medical history, clinical examination, radiological investigations and confirmatory pathological diagnosis for better management.
References
-
de Perrot M, Brundler M, Totsch M, Mentha G, Morel P (2000) Mesenteric cysts. Toward less confusion? Digestive Surgery 17(4): 323-328.
-
Pithawa AK, Bansal AS, Kochar SP (2014) “Mesenteric cyst: A rare intra-abdominal tumour”. Med J Armed Forces India 70(1): 79-82.
-
Kurtz RJ, Heimann TM, Holt J, Beck AR (1986) Mesenteric and retroperitoneal cysts. Ann Surg 203(1): 109-112.
-
Grosfeld JL, O Neill JA Jr, Coran AG, Fonkalsrud EW, Richard RR (2006) Mesenteric and omental cysts. editors Pediatric Surgery. In; Philadelphia 6th (Edn), Mosby Elsevier, pp: 1399-1406.
-
Prakash A, Agrawal A, Gupta RK, Sanghvi B, Parelkar S 2010 Early management of mesenteric cyst prevents catastrophes: a single centre analysis of 17 cases. Afr J Paediatr Surg 7(3): 140-143.
-
Yacoub J, Clark J, Paal E, Manning M (2021) Approach to Cystic Lesions in the Abdomen and Pelvis, with Radiologic-Pathologic Correlation. Radiographics 4(5): 1368-86.
-
Jagtap SV, Agarwal G, Gautam A, Jagtap SS (2020) Mucinous cystadenoma of liver with mesenchymal stroma. Clin Pathol 4(1): 00126.
-
Metaxas G, Tangalos A, Pappa P, Papageorgiou I (2009) Mucinous cystic neoplasms of the mesentery: a case report and review of the literature. World J Surg Oncol 7(1): 47.
-
Jagtap SV, Dhawan SD, Jagtap S, Kshirsagar NS (2014) Mucinous cystadenocarcinoma of the ovary presenting as a giant pelvic-abdominal mass. Int J Med Sci Public Health 3(10): 1305-1307.
-
Tan J JY, Tan KK, Chew SP (2009) Mesenteric Cysts: An Institution Experience Over 14 Years and Review of Literature. World J Surg 33(9): 1961-1965.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet