Clinicopathologic Characterization of Double PIK3CA Mutated Advanced Breast Cancer: A Retrospective Cohort Study from a Single Institution
Objectives: We aimed to characterize the clinicopathologic and molecular features of double PIK3CA mutated advanced breast cancer in a retrospective cohort study. Methods: This retrospective study included 196 advanced breast cancer patients who had the Oncomine next generation sequencing analysis. The clinicopathologic parameters were recorded for each individuals including age, tumor type, grade, ER, PR, HER2, and recurrence free survival. Results: PIK3CA mutations were detected in 77.5% (152/196) of advanced breast cancer patients, 129 (84.8%) of which contained single mutations, 20 (13.1%) of which contained double mutations, and 3 (2%) of which contained triple mutations. Double PIK3CA mutated tumors were mostly seen in postmenopausal women, had lower combined histologic grade, and were enriched in hormone receptor positive human epidermal growth factor receptor negative (HR+/HER2-) disease. Double PIK3CA mutations were more frequently associated with concurrent mutations of ESR1 (p=0.017) and ARID1A (p=0.054) compared to single PIK3CA mutations. No significant progression free survival differences were observed between PIK3CA mutated and wild-type groups and between double and single PIK3CA mutated groups when applied to all patients or HR+/ HER2- patients. Conclusion: Double PIK3CA mutated advanced breast cancer have similar clinicopathologic features as single mutated ones but demonstrate unique molecular features.
Key Points
- We further investigate the clinicopathologic significance of double PIK3CA mutations in advanced breast cancer.
- Double PIK3CA mutated tumors have similar clinicopathologic features as the single mutated ones, including tumor grade, type hormone receptors and HER2 status, stage, and clinical prognosis.
- Molecular characterization reveals frequent concurrent ESR1 and ARID1A genetic alteration in double PIK3CA
mutated tumors, which may be implicated in the therapy related resistance mechanism.
Background
Phosphatidylinositide 3-kinases (PI3K) are a family of lipid kinases that participate in a variety of cellular processes, including cell growth, proliferation, differentiation, motility, and survival. PIK3CA encodes one of the α-isoform of the catalytic subunit (p110α) of the PI3K heterodimer. Oncogenic mutations of PIK3CA are present in up to 40% HR+/HER2- breast cancer and are associated with good clinical outcome [1, 2, 3, 4, 5, 6].
The value of PIK3CA as a therapeutic target in breast cancer has been investigated in multiple studies. In the recent SOLAR-1 phase 3 clinical trial, treatment with the PI3Kα-specific inhibitor alpelisib in combination with potent ER signaling inhibitor fulvestrant prolongs progression-free survival over alpelisib monotherapy in PIK3CA mutated, HR+/ HER2-advanced breast cancer patients [7]. However, the resistance remains problematic. Another study shows that double PIK3CA mutations are detected in 8-12% of primary and metastatic breast cancers. In such tumors, the two mutations reside on the same allele. These so-called PIK3CA double mutations induce PI3K hyperactivation by disrupting the p85-p110a interaction and by enhancing p110a binding of membranes. Double PIK3CA mutated tumors show greater PI3K activity and downstream pathway activation as well as enhanced sensitivity to alpelisib when comparing to single PIK3CA mutated or wild type tumors [8].
The clinical significance of double PIK3CA mutated breast cancer has not been well studied. Here we characterized the pathologic features and clinical consequence of double PIK3CA mutated breast cancer from our institution.
Materials and Methods
A total of 196 patients were recruited in this study. All patients were diagnosed as metastatic or recurrent breast cancer and had Oncomine next generation sequencing (NGS) assay performed at the Yale New Haven Hospital from January 2016 to April 2022. The clinical and pathologic findings were retrieved for each individual patient including age, tumor type, grade, ER, PR, HER2, PIK3CA mutation and concurrent molecular alteration. Progression free survival (PFS) was defined as the period from the date of primary pathologic diagnosis to the date of recurrence or distance metastasis (in months).
The Oncomine NGS were performed at the Yale New Haven Hospital molecular diagnostic laboratory. Nucleic acids were extracted using a commercially available kit (Qiagen or Promega) and were quantitated on a Qubit 2.0 fluorometer. Targeted, amplicon-based sequencing was performed using three successive versions of the Oncomine (OCA v3) on an Ion Torrent platform (Thermo Fisher Scientific). The OCA V3 examines tumor DNA for mutations and/or amplifications in 146 cancer-related genes. nd tumor RNA for gene fusions involving 44 oncogenic driver genes, respectively. Sequencing data sets were processed through an internally developed bioinformatic pipeline. Interpretation and clinical reporting of results was performed by molecular pathologists.
Statistical Analysis
Univariate analysis was performed to investigate the clinicopathologic variables among the double PIK3CA mutated, single PIK3CA mutated, and wild type groups using the Fisher exact test. All reported tests were conducted at a normal significance level of 0.05. Statistical analysis was performed using R version 3.5.1 (http://www.r-project.org).
Results
Among 196 advanced breast cancer patients, 152 (77.5%) patients were detected to have PIK3CA mutations which included 129 (84.9%) single mutations, 20 (13.1%) double mutations, and 3 (2%) triple mutations. Similar as single PIK3CA mutated tumor, double PIK3CA mutated tumors were mostly seen in postmenopausal women (mean age of 52.3 year) and were enriched in HR+/HER2- disease (18/20, 90%). The known associated tumor histology included invasive ductal carcinoma (12/20, 60%), invasive lobular carcinoma (3/20, 15%), and mixed invasive ductal and lobular carcinoma (2/20, 10%). Tumors were mostly intermediate grade (12/20, 60%) and low grade (4/20, 20%). No statistically significant differences were observed when comparing tumor histology, grade, and receptor profiles among double PIK3CA mutated, single PIK3CA mutated, and wild type groups (Table 1).
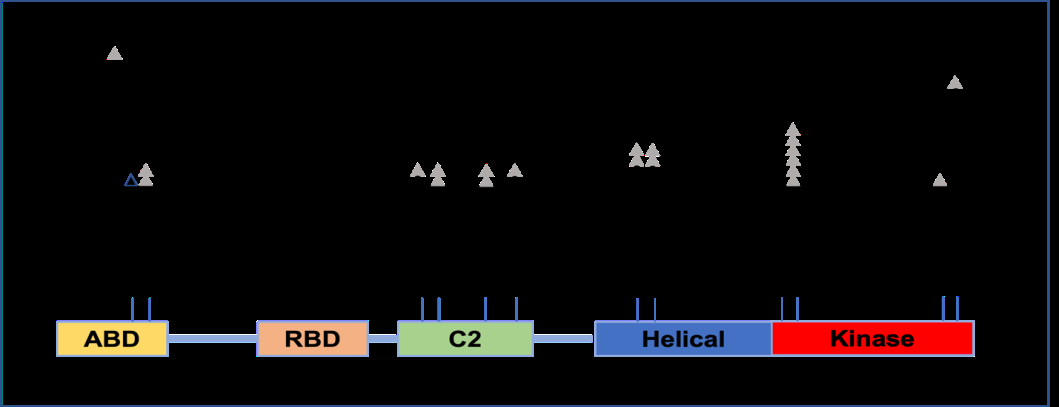
We next examined the molecular characteristics of double PIK3CA mutations in these advanced breast cancers. The major hotspot mutations were mostly located in the helical and kinase domains involving H1047 (55%), E542 (10%), and E545 (10%). The second mutant sites were mostly located in the kinase domain E726 (30%). In addition to these common and typical “major-mutant” hotspots, other “minor-mutant” sites were also detected in our cohort including E542 (10%), E545 (10%), E418 (10%), D350 (10%), M1043 (10%) and H1047L (5%) (Figure 1). Interestingly, double PIK3CA mutations were more frequently associated with concurrent estrogen receptor 1 (ESR1) mutations compared to the single mutated tumors (25% versus 7.7%, p=0.017). The identified ESR1 mutations were all activating mutations including D538G and Y537S. Similarly, ARID1A mutations were more frequently identified in the double PIK3CA mutated tumors (20% versus 7%, p=0.054)) including the inactivating and deleterious mutations Q487Te and Q1200Te. No significant differences were seen in other common gene alterations in breast cancer, including AR variant, NF1, TP53, BRCA, PTEN, CDH1, ERBB2, GATA3, and PIK3R1(Table 2).
| Double mutation | Single mutation (n=129) | Wild type | P value | |
|---|---|---|---|---|
| (n=20) | (n=44) | |||
| Age at primary diagnosis | 52.35,+ 12.81 | 54.23,+ 11.51 | 56.57,+ 10.26 | 0.33 |
| Age at tumor metastasis | 58.4, + 11.46 | 61.52, +9.78 | 61.95, + 9.58 | 0.38 |
| Tumor type | 0.55 | |||
| Invasive ductal carcinoma | 12/20 (60%) | 84/129 (65.11 %) | 37/44 (84.09%) | |
| Invasive lobular carcinoma | 3/20 (15%) | 31/129 (24.03%) | 2/44 (4.55%) | |
| Mixed invasive ductal and lobular carcinoma | 2/20 (10%) | 2/129 (1.55%) | 1/44 (2.27%) | |
| Tumor grade | 0.65 | |||
| G3 | 2/20 (10%) | 31/129 (24.03%) | 7/44 (15.91%) | |
| G2 | 12/20 (60%) | 78/129 (60.47%) | 27/44 (61.36%) | |
| G1 | 4/20 (20%) | 6/129 (4.65%) | 2/44 (4.55%) | |
| TNBC (n/n, %) | 2/20 (10%) | 21/129 (16.28%) | 6/44 (13.64%) | 0.86 |
| HER2+ (n/n, %) | 0/20 (0%) | 8/129 (6.98%) | 4/44 (9.09%) | 0.381 |
Table 1: Clinicopathological features of double PIK3CA mutated breast cancer.
| Concurrent genetic alteration | Double mutations (n=20) | Single mutations (n=129) | P value (Chi2/fisher) |
|---|---|---|---|
| ESR1 | 5 (25%) | 10 (7.75%) | 0.017 |
| ARID1 | 4 (20%) | 9 (7.00%) | 0.054 |
| NF1 | 3 (15%) | 6 (4.65%) | 0.07 |
| PIK3R1 | 1 (5%) | 1 (0.77%) | 0.126 |
| ERBB2 | 0 (0%) | 13 (10.1%) | 0.137 |
| AR variant | 6 (30%) | 21 (16.28%) | 0.138 |
| TP53 | 4 (20%) | 37 (28.68%) | 0.418 |
| GATA3 | 0 (0%) | 4 (3.10%) | 0.424 |
| PTEN | 1 (5%) | 11(8.53%) | 0.589 |
| BRCA | 2 (10%) | 10 (7.75%) | 0.731 |
| CDH1 | 1 (5%) | 5 (3.88%) | 0.819 |
Table 2: Concurrent molecular alterations in the double PIK3CA mutated breast cancer.
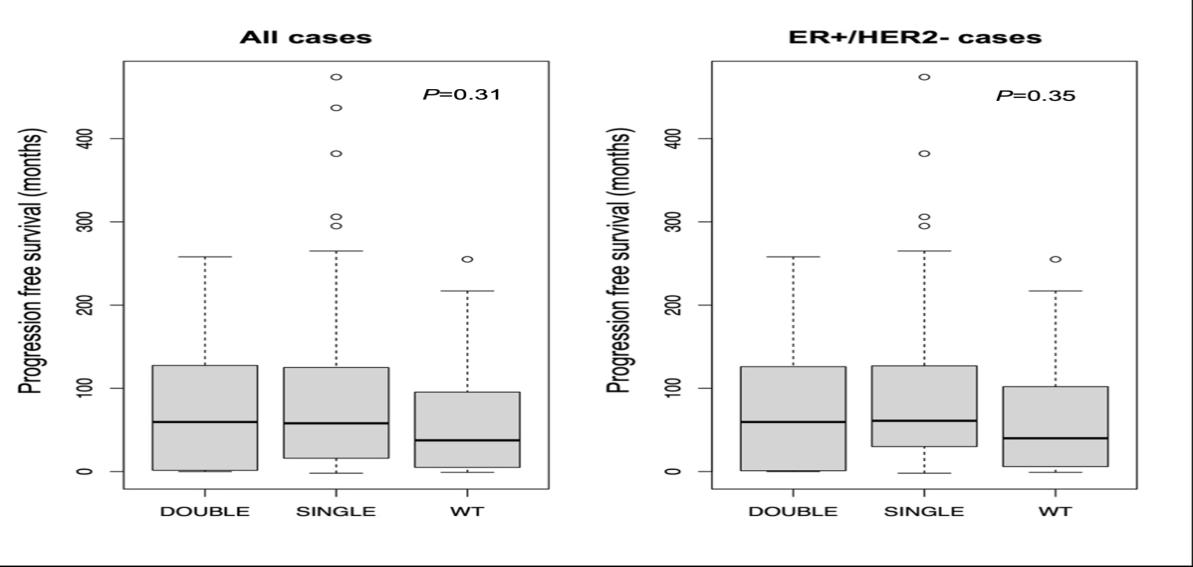
Patients with double and single PIK3CA mutations had comparable PFS when applied to all patients (median of 59.5 versus 61 months, p=0.31) or HR+/HER2- patients (median of 75.1 versus 88.9 months, p=0.35). Though combined double and single PIK3CA mutations appeared to have a prolonged PFS comparing to those with wild type tumors (p=0.12), but the p value did not reach statistical difference in this study (Figure 2).
Discussion
In this study, we performed a comprehensive analysis of PIK3CA mutation in advanced stage of breast cancer. Based on the Oncomine NGS assay results, PIK3CA mutations were detected in 77.5% of advanced breast cancer patients, which was higher than the reported frequency from the Cancer Genomic Atlas (TCGA) breast cancer database (36%) and other studies (66%)9. The assay used in this study not only detected hotspot PIK3CA mutations (H1047R, E545K, E543K, N345K, H1047L) but also included less common mutations E722, E418, E453, E345, E350, R93, R88, and some rare mutations. Additionally, most of patients enrolled in this study had metastatic breast cancer. Among 152 patients with PIK3CA mutations, 105 patients had test on the metastatic tumor, 7 patients had sequencing test on their body fluid, and 40 patients had test on the tumor of primary site. PIK3CA mutations detected in this study may reflex global tumoral heterogeneity compared to those detected from tumor of primary site. This observation also raised another possibility that PIK3CA mutations might be acquired along disease progression and metastasis. Further, we found that 15% of patients had two or more PIK3CA mutations in our study cohort. This data was consistent with previous report [3, 8, 10]. The major mutation site involved H1047, E542, and E545. The second mutation site frequently involved E726 as reported in previous studies but also involved R93, D350, E418, E542, and E545. These major- and minor mutational pattern sites might be specific to breast cancer.
For the first time, our study showed that double PIK3CA mutations were more frequently associated with ESR1 and ARID1A molecular alterations compared to single PIK3CA mutations. ESR1 mutations are a common cause of acquired resistance to endocrine therapy alone or in combination with PI3K inhibition in metastatic HR-positive breast cancer [11, 12]. Target PI3Kα suppression causes upregulation of ER-dependent transcriptional activity as well as expression of ESR1 mRNA and ER protein [13, 14]. The phase III clinical trial of the PI3Kα inhibitor alpelisib with ER signaling inhibitor fulvestrant in patients with ER+ metastatic breast cancer revealed that the overall better response rate in patients with multiple mutations in PIK3CA rather than single hotspot mutations [8]. The more frequent ESR1 activating mutations present in the double PIK3CA mutated advanced breast cancer might explain the underlying mechanisms for the better prognosis in response to alpelisib and fulvestrant.
ARID1A is a tumor suppressor gene which is frequently mutated in ovarian, endometrial, breast, urinary bladder and gastrointestinal cancers [15, 16, 17, 18, 19, 20, 21]. Synergic effects of loss of ARID1A and PI3K-Akt pathway has been implicated in the development of ovarian clear cell carcinoma and resistance to conventional platinum-based chemotherapy [22, 23, 24]. Loss of ARID1A was also associated with resistance to several drugs that inhibit the HER2/PI3K/mTOR signaling cascade in breast cancers including trastuzumab resistance [25]. Here we demonstrated that double PIK3CA mutations in advanced breast cancer was associated with ARID1A inactivating mutation. Our findings may provide another perspective to explain the treatment resistance mechanism in double PIK3CA mutated breast cancer.
Characterization of double PIK3CA mutated tumors revealed an overlapping clinicopathologic features as the single PIK3CA mutated ones, both of which were most seen in postmenopausal women, had lower combined histologic grade, enriched in HR+/HER2- disease, and had comparable PFS. Although the number of double mutated tumors with known histology was small in the present study, we have been able to show double PIK3CA mutations are associated with pathogenesis of both ductal and lobular carcinoma.
There are several limitations in this study. First, most of PIK3CA mutations (>70%) were detected from metastatic tumor sites or body fluid, which may have a different expression pattern from the primary tumor sites. Second, the study included limited patients with double or multiple PIK3CA mutations. This small sample size may preclude a definitive conclusion with statistical significance when comparing clinical consequences among patients with different PIK3CA mutation status.
In summary, we retrospectively studied the clinicopathologic and molecular features of somatic PIK3CA mutations in advanced breast cancer patients. Patients with double PIK3CA mutations had similar clinicopathologic features as those with single PIK3CA mutations. Double PIK3CA mutations were more frequently associated with concurrent ESR1 and ARID1A mutations which might implicate the underlying mechanism for therapy resistance. Our study expanded knowledge of PIK3CA mutations in breast cancer thus better position PI3Kα inhibitors in the treatment landscape.
References
-
Saal LH, Holm K, Maurer M, Memeo L, Wang X, et al. (2005) PIK3CA mutations correlate with hormone receptors, node metastasis, and ERBB2, and are mutually exclusive with PTEN loss in human breast carcinoma. Cancer Res 65(7): 2554-2559.
-
Hale KS, Gonzalez Angulo AM, Lluch A, Neve RM, Kuo WL, et al. (2008) An integrative genomic and proteomic analysis of PIK3CA, PTEN, and AKT mutations in breast cancer. Cancer Res 68(15): 6084-6091.
-
Curtis C, Shah SP, Chin SF, Turashvili G, Rueda OM, et al. (2012) The genomic and transcriptomic architecture of 2,000 breast tumours reveals novel subgroups. Nature 486(7403): 346-352.
-
Maruyama N, Miyoshi Y, Taguchi Y, Tamaki Y, Maruyama N, et al. (2007) Clinicopathologic analysis of breast cancers with PIK3CA mutations in Japanese women. Clin Cancer Res 13(2Pt1): 408-414.
-
Sobhani N, Roviello G, Corona SP, Scaltriti M, Ianza A, et al. (2018) The prognostic value of PI3K mutational status in breast cancer: A meta-analysis. J Cell Biochem 119(6): 4287-4292.
-
Marvelde LT, Milne RL, Fumagalli D, Fountzilas G, Zardavas D, et al. (2018) Tumor PIK3CA Genotype and Prognosis in Early-Stage Breast Cancer: A Pooled Analysis of Individual Patient Data. J Clin Oncol 36(10): 981-990.
-
Ciruelos EM, Juric D, Loibl S, Campone M, Andre F, et al. (2021) Alpelisib plus fulvestrant for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: final overall survival results from SOLAR-1. Ann Oncol 32(2): 208-217.
-
Razavi P, Johnson JL, Shao H, Shah H, Vasan N, et al. (2019) Double PIK3CA mutations in cis increase oncogenicity and sensitivity to PI3Kalpha inhibitors. Science 366(6466): 714-723.
-
Cancer Genome Atlas N (2012) Comprehensive molecular portraits of human breast tumours. Nature 490(7418): 61-70.
-
Zhang G, Chen B, Chen X, Wen L, Xiao W, et al. (2021) Mutational Landscape of PI3K-AKT-mTOR Pathway in Breast Cancer: Implications for Targeted Therapeutics. J Cancer 12(14): 4408-4417.
-
Spring LM, Bardia A, Wander SA, Brett JO (2021) ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer. Breast Cancer Res 23(1): 85.
-
Toi M, Neven P, Sohn J, Grischke EM, Tolaney SM, et al. (2022) Clinical Significance of PIK3CA and ESR1 Mutations in Circulating Tumor DNA: Analysis from the MONARCH 2 Study of Abemaciclib plus Fulvestrant. Clin Cancer Res 28(8): 1500-1506.
-
Li Z, Bergamaschi A, Ellis H, Toska E, Bosch A, et al. (2015) PI3K inhibition results in enhanced estrogen receptor function and dependence in hormone receptor- positive breast cancer. Sci Transl Med 7(283): 283ra51.
-
Hosford SR, Dillon LM, Shee K, Liu SC, Yang W, et al. (2016) Strategically Timing Inhibition of Phosphatidylinositol 3-Kinase to Maximize Therapeutic Index in Estrogen Receptor Alpha-Positive, PIK3CA-Mutant Breast Cancer. Clin Cancer Res 22(9): 2250-2260.
-
Wang TL, Shih IM, Mao TL, Nakayama K, Jones S, et al. (2010) Frequent mutations of chromatin remodeling gene ARID1A in ovarian clear cell carcinoma. Science 330(6001): 228-231.
-
Wiegand , Shah SP, Al Agha OM, Zhao Y, Wiegand KC, et al. (2010) ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med 363(16): 1532-1543.
-
Cavallone L, Tuzmen S, Chabot C, Ferrario C, Mamo A, et al. (2012) An integrated genomic approach identifies ARID1A as a candidate tumor-suppressor gene in breast cancer. Oncogene 31(16): 2090-100.
-
Guo G, Huang Y, Hu X, Tang A, Gui Y, et al. (2011) Frequent mutations of chromatin remodeling genes in transitional cell carcinoma of the bladder. Nat Genet 43(9): 875-878.
-
Lata S, DelaBastide M, Montgomery EA, Wang JS, Streppel MM, et al. (2014) Next-generation sequencing of endoscopic biopsies identifies ARID1A as a tumor- suppressor gene in Barrett’s esophagus. Oncogene 33(3): 347-357.
-
Kan J, Yuen ST, Shi ST, Chu KM, Wang K, et al. (2011) Exome sequencing identifies frequent mutation of ARID1A in molecular subtypes of gastric cancer. Nat Genet 43(12): 1219-1223.
-
Pawlik TM, Anders RA, Selaru FM, Streppel MM, Jiao Y, et al. (2013) Exome sequencing identifies frequent inactivating mutations in BAP1, ARID1A and PBRM1 in intrahepatic cholangiocarcinomas. Nat Genet 45(12): 1470-1473.
-
Tsuda H, Takano M, Tamai S, Matsubara O, Yamamoto S, et al. (2012) PIK3CA mutations and loss of ARID1A protein expression are early events in the development of cystic ovarian clear cell adenocarcinoma. Virchows Arch 460(1): 77-87.
-
T ter Haar N, Seeber LM, v Diest PJ, Hes FJ, Bosse T, et al. (2013) Loss of ARID1A expression and its relationship with PI3K-Akt pathway alterations, TP53 and microsatellite instability in endometrial cancer. Mod Pathol 26(11): 1525-1535.
-
Noske A, Dedes KJ, Fink D, Imesch P, Samartzis EP, et al. (2013) ARID1A mutations and PI3K/AKT pathway alterations in endometriosis and endometriosis- associated ovarian carcinomas. Int J Mol Sci 14(9): 18824-49.
-
Sonnenblick A, Gennissen A, Brohée S, Hijmans EM, Berns K, et al. (2016) Loss of ARID1A Activates ANXA1, which Serves as a Predictive Biomarker for Trastuzumab Resistance. Clin Cancer Res 22(21): 5238-5248.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet