Compartment Syndrome of the Hand after Multiple Fractures of the Metacarpals: A Rare Localization with a Poor Prognosis: Two Case Reports and a Literature Review
Compartment syndrome is a surgical emergency. In fact, it is a “race against the clock” we will discuss our experience with two cases who presented with hand compartment syndrome after suffering numerous metacarpal fractures The treatment included a discharge incisions, metacarpal pinning, and close hand surveillance.
Introduction
Acute limb compartment syndrome is a medical and surgical emergency. The diagnosis is based on different signs and symptoms that occur due to the increased pressure in a muscular compartment that is non-expandable. If left untreated or we had a delay in treatment, it leads to severe consequences starting by functional impairment reaching amputation in late stages. The vital prognosis may be threatened in some cases, particularly those involving crushed limbs. Hand compartment syndrome is a rare but frightening condition, especially when associated with a crushed limb. This is explained by the hand’s anatomical particularity, which is responsible for a significant difference in pressure between the compartments, thus the risk of its delayed diagnosis.
In this article, we describe a compartment syndrome in the hand as part of a crushing trauma with multiple metacarpal fractures in two clinical cases.
Case 1
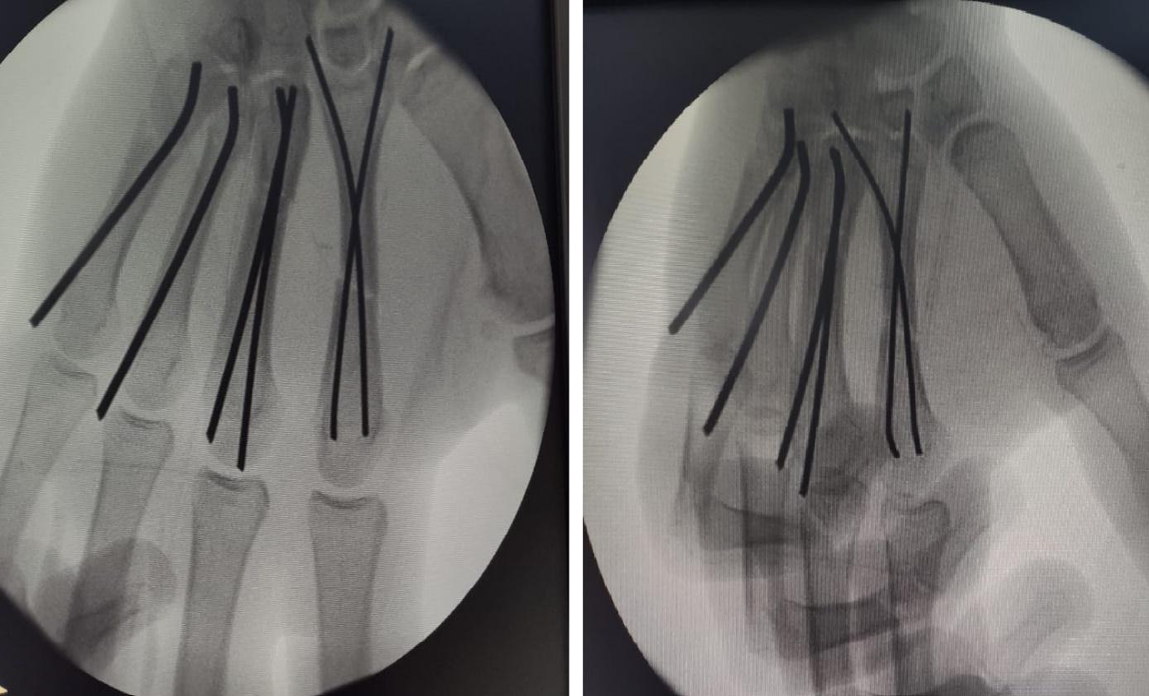
A 31-year-old right-handed laborer who suffered a crush injury to his right hand as a result of a public road accident (a motorcycle being hit by a car), resulting in pain and total functional impotence. The patient presented with an edematous hand in a discrete intrinsic position as well as skin elasticity loss. The diagnosis of compartment syndrome was based on a triad: spontaneous pain that increased during passive extension, refractory to painkillers, allowing us to distinguish it from a simple pain caused by the fractures. A simple palpation of the increased-volume muscular masses accentuates this pain. The appearance of neurological symptoms such as paresthesia in the pulp of the first three fingers indicates median nerve compression at the wrist. The radiological examination Figures 1 & 2 revealed multiple fractures of the right hand’s metacarpals (M2-M3-M4-M5), with no associated dislocation or foreign body.




To avoid complications, including the complete and permanent loss of hand function due to retraction of the intrinsic muscles, emergency surgical management was required.
The patient underwent emergency surgery under general anesthesia, at the 4th post traumatic hour, supine, with his hand on a hand-table. A closed reduction of the metacarpal fractures was done under fluoroscopic control, and a percutaneous intramedullary pinning using two pins was done for M2 and M3 Figure 3 to ensure a good rotational stability.
To treat the compartment syndrome, we performed a dermo fasciectomy (aponeurotomy), which is the only way to reduce pressure inside a compartment. To avoid damaging the median nerve by evacuating the hematoma, we made two dorsal incisions (radial edge of M2 and M4) and an incision directly over the carpal tunnel, with dissection deeply and an incision through the transverse carpal ligament (Figure 4).

All incisions were left open, with the exception of the one over the carpal tunnel. The wrist is then immobilized in a slight extension to prevent flexor tendon dislocation, associated with syndactyly of the concerned fingers to provide good stability for the consolidation to occur. Good reduction and osteosynthesis were confirmed by a post operative radiography, and the hand was kept elevated Figure 5.

The pain was completely resolved after 48 hours and the paresthesia gradually disappeared by 72 hours.
After one week, skin closure was done and the patient was discharged home. He was followed up on regular basis. The pins were removed under local anesthesia after six weeks. In the second month, the patient was able to return to work. At his most recent clinical and radiological check-up at sixth month after the operation, he reported no discomfort with his hand (Figure 6).

Case 2
A 25-year-old right-handed taxi driver with no significant past medical history presented to the emergency department after sustaining a crush injury to the left hand after a car accident. On physical examination he had a very edematous left hand with two superficial wounds on the dorsal side of the ulnar edge and no vascular injury was identified (Figure 7).

The palpation was very painful, and even the slightest movement exacerbated the pain. A transverse fracture of the second and third metacarpal bone shafts was seen on radiography. After two hours, he started feeling tingling in the first three fingers. An emergency dermofasciotomy was done. The incision was centered over the second interdigital space and intramedullary pinning of the second and third metacarpals was done. The postoperative follow-ups were favorable, with a significant improvement in pain and the complete absence of tingling. After 48 hours, the patient was discharged home. The clinical course was favorable, with hand functions recovered after 5 months.
Discussion
The muscles in each limb are grouped in septated muscular compartments, and their organization varies depending on the anatomical location. There are three muscular compartments at the level of the hand: thenar, hypothenar, and interosseous. The latter are the most likely to develop compartment syndrome after trauma. In fact, only the first three dorsal interosseous muscles are completely covered by a solid fascia, as Ling, et al. [1] demonstrated in their anatomical study on cadaveric hands. The thenar muscles are not always fully covered by fascia and the hypothenar are only covered by a loose layer of fascia. This could explain the low incidence of hand compartment syndrome. According to Spinner, et al. [2], this diagnosis was based on a triad of symptoms: spontaneous pain, paralysis, and increased pain during passive extension or stretching. The emergence of intolerable pain that is refractory to painkillers can be a hallmark in the diagnosis [3]. The pain is exacerbated by simple palpation of the enlarged muscular masses. However, because of associated fractures, this pain must be specified according to the cause in some cases [4]. In a study, Gong, et al. [5] found seven cases of compartment syndrome out of 382 multiple metacarpal fractures, a rate of 1.8 percent. Other studies found more atypical compartment syndrome caused by insect stings [6] and heroin injection [7]. An intramuscular pressure measurement allows us to define compartment syndrome objectively. Gong, et al. [5] suggested that a pressure greater than 40 mmHg is an indication for fasciotomy even in the absence of clinical signs. However, the normal value of this pressure, as well as the critical level above which surgical release is required, are still debatable. According to Matsen, et al. [8], the concept of critical pressure is of limited utility. We believe that measuring intramuscular pressure should not delay patient management; it is principally used in debatable cases.
Although, even the slightest suspicion of a compartment syndrome must lead to decompression incisions because, once started, this phenomenon is irreversible. It is then a “race against the clock” to break the vicious circle (case 2). The aponeurotomy should be performed within the first 6 hours to avoid serious complications and sequel like complete and permanent loss of hand function due to retraction of intrinsic muscles, known as Finochietto’s syndrome [9, 10]. Spinner highlighted the importance of early diagnosis in a series of 14 cases [2].
In our cases, we performed neurolysis of the median nerve by section of the transverse carpal ligament, as recommended by Ouellette, et al. [9], due to the presence of paresthesia in the pulp of the first three fingers caused by compression of this nerve. Other teams, such as Gong, et al. [5], do not perform median nerve neurolysis at the wrist even if there were paresthesias over the median nerve sensory territories, and observed a good recovery after 3 months. We recommend leaving the decompression incisions open or only partially closed, and to choose intramedullary osteosynthesis for the metacarpal fractures. Plate osteosynthesis was not possible due to the location of the decompression incisions. We did not find a preferred technique of fixation in the literature. Finally, we think that the crushing injury mechanism and presence of multiple metacarpal fractures can be used as red flags for increasing suspicion of compartment syndrome of the hand.
Conclusion
Hand compartment syndrome is a rare condition that necessitates quick and effective surgical intervention. Once the phenomenon has begun, it is irreversible. Only the discharge incisions have the potential to break the vicious circle.
- Conflicts of Interests The authors have declared no conflicts of interest. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
- Authors’ Contributions All authors contributed to the conduct of this research and read and approved the final version of the manuscript.
- Availability of data and materials Not applicable
- Funding I have not received any funding for this article.
- Ethical approval Not applicable
- Patient Consent Written informed consent was obtained from the patient for publication of this case report and accompanying images.
A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
References
-
Ling MZ, Kumar VP (2009) Myofascial compartments of the hand in relation to compartment syndrome: cadaveric study. Plast Reconstr Surg 123(2): 613-616.
-
Spinner M, Aiache A, Silver L, Barski AJ (1974) Impending ischemic contracture of the hand. Early diagnosis and management. Plast Reconstr Surg 50(4): 341-349.
-
Masquelet AC (2001) Traitement des syndromes des loges et du syndrome de volkmann. Encycl Med Chir Tech Chir Orthop Traumatol 44(078): 18.
-
Del Pinal F, Herrero F, Jado E, Garci-Bernal F, Cerezal L (2002) Acute hand compartment syndromes after closed crush: a reappraisal. Plast Reconstr Surg; 110(5): 1232-1239.
-
Gong X, Lu LJ (2003) Diagnosis and treatment of complications associated with closed multi-fractures in metacarpals. Zhongguo Xiu Fu Chong Jian WaiKe Za Zhi 17(3): 198-200.
-
Sawyer JR, Kellum, Creek AT, Wood GW (2010) Acute compartment syndrome of the hand after a wasp sting: a case report. J Pediatr Orthop B 19(1): 82-85.
-
Ouellette EA (1998) Compartment syndromes in obtunded patients. Hand Clin 14(3): 431-450.
-
Matsen III FA, Winquist RA, Krugmire RB (1980) Diagnosis and management of compartmental syndromes. J Bone Joint Surg (Am) 62(2): 286-291.
-
Ouellette EA, Kelly R (1996) Compartment syndromes of the hand. J Bone Joint Surg (Am) 78(10): 1515-1522.
-
Buck Gramcko D (1995) La rétraction ischémique de la main. In: Tubiana R (Ed.). Traité de chirurgie de la main, Paris, USA, 5.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet