A Rare Torsion Case of Polycystic Ovarian Syndrome: A Natural Course with Laparoscopic, Cytological and Pathological Findings
Polycystic ovary (PCO) syndrome cases with adnexal torsion in a natural cycle without ovarian induction are rare, and many torsion cases in PCOs involve pelvic masses, such as uterine fibroids. A 37-year-old woman, gravida two para two, came in an emergency because of lower abdominal pain for 2 or 3 days. PCO was followed in a previous hospital. At a visit in her Douglas pouch, a 7.3 x 4.5 cm mass that was consistent with the point of tenderness was detected by ultrasonography and magnetic resonance images. The patient underwent a semi-emergent laparoscopic surgery for a diagnosis of torsion of the left adnexa. At an abdominal exploration, the left ovary was swollen to approximate 7 cm in size and twisted 360°clockwise. The intraoperative imprint cytology showed the presence of fibrous cells alone, thus the malignancy denied. Histologically, fibrously thickened cortex and multiple follicular cysts due to atretic follicles were found, compatible with PCO. As the patient did not desire to have children and less likely to twist the right ovary, she wanted having low dose pills.
Introduction
Adnexal torsion has been thought to be caused by an ovarian tumor and been considered an important acute abdominal gynecological disease. Polycystic ovary (PCO) syndrome causes ovulation disorders and the syndrome is frequently encountered in fertility practices. Torsion of the appendage pedicle occurs in approximate 7% of ovarian hyper stimulation syndrome induction in normal ovaries [1]. Although the PCO is non-neoplastic, the approximate 20% was reported to show enlarged ovaries [2]. Among PCO cases, however, reports of the torsion of the appendage pedicle during a natural cycle have been rare [3]. Here, we report a PCO torsion case with a natural course without a pelvic mass. In addition to diagnostic imaging, intraoperative cytology was useful for the diagnosis of PCO pedicle torsion.
Case Report
A 37-year-old woman, gravida two Para two, came in an emergency to Gujo City Hospital because of lower abdominal pain for 2 or 3 days. Her menstrual history was a 90-120 days cycle. We heard that she had received a loop electro-
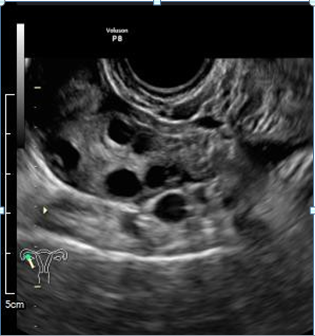
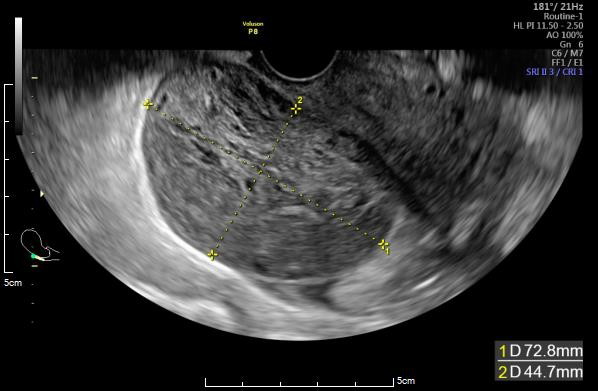
surgical excision proceeding conization due to cervical carcinoma in situ in 24 y. o. and PCO syndrome has been followed in a previous hospital. She was diagnosed with PCO after taking a hormone test at a previous hospital, but we didn’t have the data. She had no family medical history. At a visit in her Douglas’ pouch, a 72.8 x 42.8 mm mass that was consistent with the point of tenderness, was detected by ultra-sonography (Figure 1B), although the right ovary showed a typical PCO image (Figure 1A).
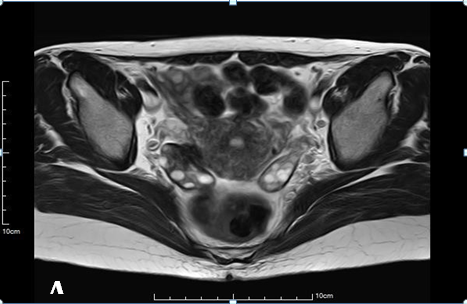
Her previous MRI was obtained postoperatively, and showed typical PCO findings recognized in bilateral normal sized ovaries (Figure 2A). At an emergent visit, the left ovary exhibited edematous swelling change in MRI (Figure 2B).
Some ascites was detected, but no other tumors like as uterine myoma could not be detected. Since it was an emergency, no hormone tests were performed. Her white blood cell count was 5930 (4000- 9000) /µL and C reactive protein (CRP) was high as 5.82 (-0.30) mg/dL. Once the

leukocyte count rose, it thought to be decreased. Meanwhile, CRP might remain high. Other no abnormal peripheral hematology or blood chemistry results were detected. Tumor markers were as follows: CA125 19.3 (~35) U/ml, CA19-9 13.0 (~37) U/ml, CA72-4 ~1.0 (~2.5) ng/ml. The
patient underwent a semi-emergent laparoscopic surgery for a diagnosis of torsion of the left adnexa on the next day after she came by ambulance.
At an abdominal exploration, the left ovary was swollen to approximate 7 cm in size and twisted 360°clockwise (Figure 3A). The right ovary was not twisted nor swollen. The swollen left ovary was edematous and white in color. It seemed that the blood flow was maintained with one torsion and the edema worsened. Although the blood flow was thought to be preserved and the left ovary might be preserved by untwisting, the patient’s pre-operative plan was to remove swollen ovary be reluctant to rekindle the pain. Thus, a left adenectomy was performed. After aspirating as much liquid as possible from the ovary in the Endpouch○r , the left ovary and tube was removed from the body (Figure 3B). The intraoperative crash cytology was performed to deny malignancy.
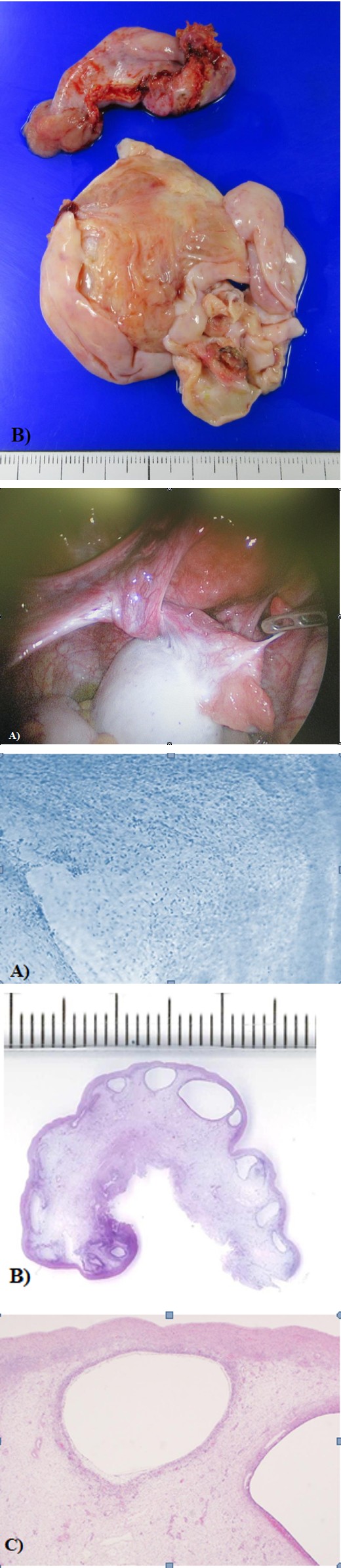
Figure 3-A: Image of the abdominal cavity. The left ovary was enlarged at approximate 7 cm in size and was twisted 360 °clockwise. B: The resected left tube (upper), and resected left ovary (under) was taken out after sucking water in the Endpouch○R .
Figure 4-A: The fibrous cells likely derived from thickened cortex and the cells thought to be capsular theca cells with edema were found (Papanicolaou stain, x 50). B: Histopathological image (H & E staining). Many ovarian follicles measured 1-5 mm in size. C: Thickening of the cortex and follicular cysts due to atretic follicles were found in edematous background. Congestion was observed near cysts (H & E staining, x 10).
As the fibrous cells likely derived from thickened cortex and the cells thought to be capsular theca cells with edema were found, the cytologic findings consistent with PCO (Figure A) and malignancy of the left ovary was denied. The
surgical duration was 42 minutes and the amount of bleeding was immeasurably small. Histopathologically, multiple variably sized cysts and cystic follicles were found (Figure 4B). Thickening of the cortex and multiple follicular cysts due to atretic follicles were found (Figure 4C), compatible with PCO. There were no necrotic changes. The patient’s postoperative process was uneventful, and discharged day 3 postoperatively. As the patient not desiring to have children wanted to prevent ovulation and to reduce the possibility of the right ovarian torsion, low dose pills have been prescribed [13]. In fact, no further torsion occurred in this case for over one year.
Discussion
PCO syndrome is a common reproductive and endocrine disorder found in 6-10% of the female population [4]. The three main characteristics are hyperandrogenism, polycystic ovaries and ovulatory dysfunction [5]. The syndrome may also be associated with metabolic issues including obesity, insulin resistance, hyperinsulinemia and type 2 diabetes mellites [2]. Fortunately, she showed no above metabolic issues. Although this patient did not receive a hormone test in our hospital, the patient clinically diagnosed with PCO from her story of being diagnosed with PCO at a previous hospital and from the oligomenorrhea and multiple ovarian follicles in her previous MRI.
Adnexal torsion represents a gynecological acute abdomen. Tenderness around the adnexal lesion during pelvic examination and ultrasonographic findings of ovarian swelling may be important to a diagnosis [3]. The differential diagnosis of adnexal torsion is considered be important from ectopic pregnancy, tubo-ovarian abscess, appendicitis, mesothelial cyst, etc [6]. In torsion cases, both MRI [7] and ultrasound [8] have been reported to show a variety of images, like as tumor. To rule out neoplastic changes, the intraoperative imprint/crash cytology was performed. As only the fibrous cells were found and neoplastic cells could not be observed, the malignancy denied in the present case. Ovarian tumors without adhesion tend to induce torsion of the pedicle on reaching a size of ≥5 cm [9]. In PCO cases, torsion of the pedicle is rare during a natural cycle without ovulation induction [3, 10]. Many normal sized ovarian torsion cases were reported to be related to enlarged uterus due to pregnancy [11, 12] or multiple myomas [13]. The present case could not involve a tumor, nor enlarged uterus. Occasionally, one ovary might be enlarged due to PCO before torsion occurred. Blood flow might not be completely blocked with only one torsion, resulting in increased edema swollen to approximate 7 cm at the surgery. Therefore, ovarian swelling due to PCOS might be one of the causes of adnexal torsion.
Low dose pills have been the first line of treatment for women with PCOS not seeking pregnancy [14], to prevent occasional ovulation and ovarian enlargement. In fact, no further torsion occurred in this case for over one year.
Conclusion
PCOS cases with adnexal torsion in a natural course are rare, and many of those have been associated with pregnancy or pelvic masses. The diagnosis of ovarian torsion remains challenging. Clinical characteristics lack sensitivity and specificity and ultrasound diagnosis is not definitive. Laparoscopy remains the investigation of choice, with Histopathological findings.
Acknowledgement
We thank the editor and reviewers for the constructive comments, which helped us to improve the manuscript. The written consent was approved by the patient before writing this case report.
Competing Interests
The authors declare that they have no competing interests.
Ethical Approval
The ethical approval of our hospital was obtained the ethical committee before writing this case report (ethical approval no. 23030601).
References
-
Abdusamad K, Hamoudi R, Maiti S (2013) Simultaneous bilateral torsion of the adnexae in an adult female without any history of ovarian stimulation. BMJ Case Rep. bcv- 2012-007909.
-
Barthelmess EK, Naz RK (2014) Polycystic ovary syndrome: current status and future perspective. Front Biosci (Elite Ed) 6(1): 104-119.
-
Matsuoka S, Kobayashi T, Kusunoki S, Ogishima D (2017) Polycystic ovary syndrome with asynchronous bilateral adnexal torsion in a natural cycle. BMJ Case Rep 2016218880.
-
Norman RJ, Dewailly D, Legro RS, Hickey TE (2007) Polycystic ovary syndrome. Lancet 370(9588): 685-697.
-
Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group (2004) Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod 19(1): 41-47.
-
Jagtap SV, Janugade H, Jagtap SS, Singh R, Chavan VV, et al. (2023) Mesenteric mesothelial cyst presented as acute abdominal pain. Clin Pathol Res J 7(1): 000154.
-
Asch E, Wei J, Mortele KJ, Humm K, Thornton K, et al. (2017) Magnetic resonance imaging performance for diagnosis of ovarian torsion in pregnant women with stimulated ovaries. Fertil Res Pract 3(1): 13-22.
-
Moro F, Bolomini G, Sibal M, Vijayaraghavan SB, Venkatesh P, et al. (2020) Imaging in gynecological disease (20): clinical and ultrasound characteristics of adnexal torsion. Ultrasound Obstet Gynecol 56(6): 934- 943.
-
Rapkin AJ (2012) Leena N Dysmenorrhea, Berek & Novac’s Gynecology. 15th ed Philadelphia, pp: 475.
-
Spitzer D, Wirleitner B, Steiner H, Zech NH (2012) Adnexal torsion in pregnancy after assisted reproduction - case study and review of the literature. Gebultsshilfe Frauenheilkd 72(8): 7126-7120.
-
Yen CF, Lin S, Murk W, Wang CJ, Lee CL, et al. (2009) Risk analysis of torsion and malignancy for adnexal masses during pregnancy. Fertil Steril 91(5): 1895-1902.
-
Ferrari F, Tisi G, Forte S, Sartori E, Odicino F (2019) Adnexal torsion with normal ovary in the third trimester of a twin pregnancy: case report and literature review. J Obstet Gynaecol Res 45(1): 226-229.
-
White M, Stella J (2005) Ovarian torsion: 10-year perspective. Emerg Med Australas 17(3): 231-237.
-
Ehrmann D A, Kasza K, Azziz R, Legro R S, Ghazzi M N; PCOS/troglitazone study group (2005) Effects of race and family history of type 2 diabetes on metabolic status of women with polycystic ovary syndrome. J Clin Endocrinol Metab 90(1): 66-71.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet