A Rare Case of Endometriosis in Urinary Bladder
Endometriosis with involvement of urinary tract is a rare occurrence. It is a chronic condition with presence of endometrial tissue outside uterine cavity. Most likely location is peritoneal surface of pelvis. We present a case of 32 year old female presenting with pelvic pain. On sonography bladder mass was detected. Transurethral resection of bladder mass revealed foci of endometriosis with mild inflammation in stroma. The diagnosis relies on identification of atleast two of the three components: endometrial glands, endometrial stromal cells or recent or old haemorrhage. Endometriosis with minimal stroma should be differentiated from invasive adenocarcinoma of the bladder. This case reports demonstrates that endometriosis in bladder although rare should always be ruled out by proper histological examination and save patient from unnecessary overtreatment.
Kundu (Acharya) S* and Choudhury A Introduction
Endometriosis is a chronic mullerian lesion characterised by presence of functional endometrial glands and stroma outside uterine cavity [1]. The disease has ability to invade surrounding structures causing painful symptoms although it’s a benign condition. The common locations for endometriosis are ovaries, broad ligament, uterosacral ligaments, and posterior cul de sac [2]. Urinary tract endometriosis is a rare occurrence, in approximately 1% cases of endometriosis. We report a case of a woman in her mid-30s who presented with pelvic pain and was found to have a bladder mass on sonographic evaluation. Transurethral resection of bladder mass was done to rule out malignancy.
A 32 year old female presented to hospital with chronic pelvic pain. The pain was dull to severe, recurrent in nature. It was not related to exercise. Patient could not correlate pain with onset of menses. It mildly subsided with NSAIDS medication. Dysuria or haematuria was not present. There was no significant family or social history of similar complains. Her vitals were normal. Routine blood and urine examination were done which were within the normal parameters. She could not provide past history of any surgical interventions. On sonography a nodular mass measuring 2 cm was noticed in bladder. The patient was subjected to cystoscopy that revealed nodular lesion in the posterior wall of the bladder. She underwent transurethral resection of bladder mass and the sample was sent for histopathological examination to rule out malignancy.
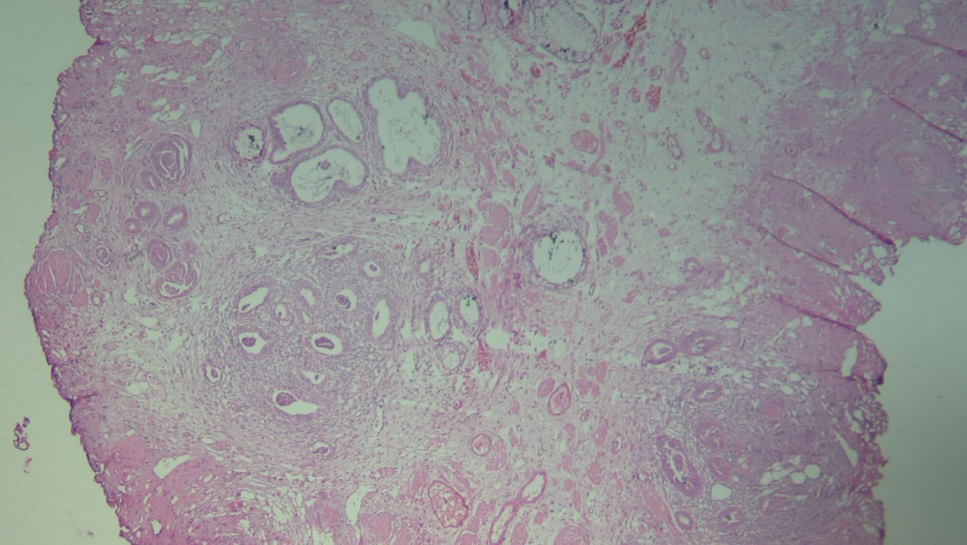
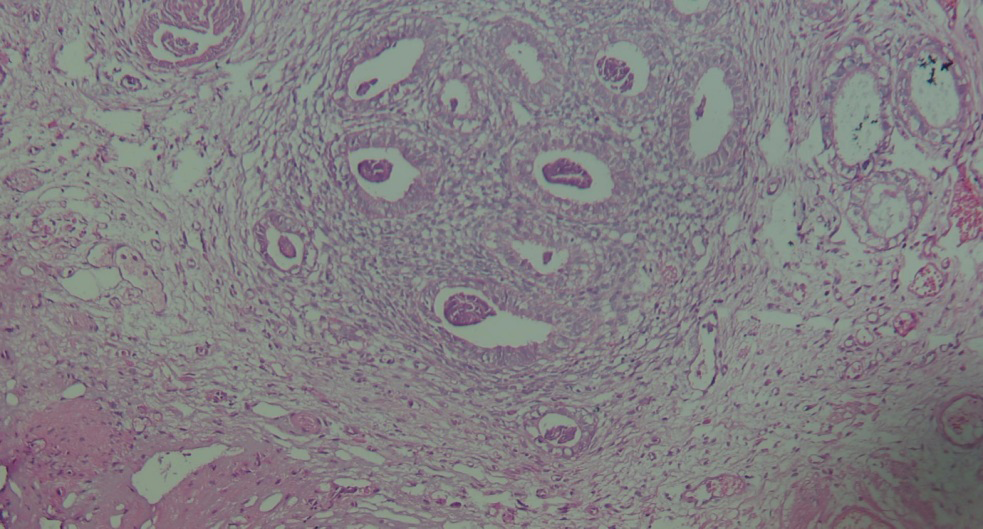
Histopathological examination revealed urothelium with reactive proliferative changes in form of cystitis - cystica amidst mixed inflammation. Numerous foci of proliferative endometrial glands and endometrial stroma was seen along with occasional areas of haemorrhage. Granuloma or invasive malignancy was not detected. Endometriosis in bladder tissue was reported See Figure 1 and 2.
Discussion
Endometriosis can occur in number of locations most likely ovaries, uterine ligaments, within rectovaginal septum and cul de sac [3, 4, 5]. Involvement of bladder is extremely rare and has been reported in roughly 1% patients with endometriosis [4]. Patients with bladder involvement usually present with urinary tract symptoms, pelvic pain and is likely cyclic in nature [2]. Bladder endometriosis can also be asymptomatic and incidentally diagnosed at the time of a cystoscopic or intraabdominal procedure.
There are three theories explaining endometriosis [1]. The first is retrograde menstruation where tiny pieces of the endometrium are carried through the fallopian tubes at the time of menstruation and implant outside of the uterus. The second theory is mullerian metaplasia, caused by metaplastic transformation of peritoneal mesothelium into endometrium under the influence of some unidentified stimulant. The third theory is through lymphatic spread.
Histological identification relies on identification of at least two of the three components: endometrial glands, endometrial stroma, or recent or old haemorrhage. Endometriosis with minimal stroma should be differentiated from invasive adenocarcinoma of the bladder. Adenocarcinoma invariably has obvious nuclear atypia.
Bladder involvement is sometimes accompanied by disease in other locations [5]. The most common place of bladder endometriosis is in posterior wall and presents as polypoid nodule or mass [6, 7].
Treatment of patient relies on multiple factors including severity of symptoms and confirmed histological diagnosis. Females who are asymptomatic, desire fertility and don’t have hydronephrosis may opt for conservative approach with periodic ultrasound exams. Medical treatment is based on progesterone, combined estrogen –progesterone therapy and GnRH analogues.
Surgical treatment is done through laparoscopy and superficial lesions are excised combined with detrusor suture. Lesions in the vesicouterine space needs cystotomy. Transurethral resection is not an optimal treatment for bladder endometriosis. Ureteral catheters could be used to reduce inadvertent ureteral damage at surgery.
Surgical management has overall success rate of 90%. Partial cystectomy has success rate around 100%. Among patients with ureteric involvement, success rate of distal ureterectomy and reimplantation is 100%, laparoscopic ureterolysis with Double J stenting followed by injection leuprolide is 75%. Medical or hormone only treatment like Gonadotropin- releasing hormone (GnRh) analogue has successe rate of 67%.
Conclusion
Bladder endometriosis is a rare entity. The diagnosis is often difficult to make because of nonspecific symptoms. Early radiological intervention with correct histopathological diagnosis helps patient in receiving adequate treatment and conserve organ functions.
• Conflict of Interest The author declares no conflict of interest.
• Acknowlegements None.
• Fundings The author (s) declared no potential conflicts of interest with respect to the authorship and /or publication of the article.
References
-
Hacker NF, Moore JG, Gambone JC (2004) Essentials of Obstetrics and Gynecology. 4th (Edn.), Elsevier Saunders, Philadelphia.
-
Perez MP, Bazan AA, Dorrego JMA, Hernández A, Francisco MG, et al. (2008) Urinary tract endometriosis: clinical, diagnostic, and therapeutic aspects. J Urol 2009 73(1): 47-51.
-
Callen PW (2000) Ultrasonography in Obstetrics and Gynecology. 4th (Edn.), W. B. Saunders, Philadelphia.
-
Rumack CW, Wilson SR, Charboneau JW (2005) Diagnostic Ultrasound. 3rd (Edn.), Elsevier Mosby, St. Louis, MO, US, 1: 1035.
-
Park SB, Kim JK, Cho KS (2008) Sonography of endometriosis in infrequent sites. J Clin Ultrasound 36(2): 91-97.
-
Pastor-Navarro H, Giménez-Bachs JM, Donate-Moreno MJ, Pastor-Guzman JM, Ruíz-Mondéjar R, et al. (2007) Update on the diagnosis and treatment of bladder endometriosis. Int Urogynecol J 18(8): 949-954.
-
Wong-You-Cheong JJ, Woodward PJ, Manning MA, Davis CJ, et al. (2006) Inflammatory and nonneoplastic bladder masses: radiologic-pathologic correlation. Radiographics 26(6): 1847-1868.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet