Comorbidities with COVID-19: Harmful Consequences for Patients with SARS-CoV-2 Infection- Related Clinical Manifestations
Human life has been endangered due to the pandemic crisis caused by the emergence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from China. The novel coronavirus known as SARS-CoV-2, or severe acute respiratory disease, poses serious problems for the healthcare system and has caused millions of deaths, which has a significant impact on the mortality rate. The symptoms of COVID-19, referred to as coronavirus disease (2016), is presented with asymptomatic, mild or severe pneumonia- like symptoms. Patients with COVID-19 who have diabetes, HIV, hypertension, cancer, cardiovascular disease, chronic obstructive pulmonary disease (COPD), and other comorbidities increase the risk of developing life-threatening. Most patients with compromised medical histories get a serious COVID-19 complications. It appears that SARS-CoV-2 targets the respiratory system, resulting in pneumonia and acute respiratory distress syndrome. These conditions cause severe systemic inflammation, multi-organ failure, and mortality, particularly in patients with pre-existing comorbidities. SARS-CoV-2 affects host cells by means of ACE-2 receptors that are present on their surface. Strong ACE-2 receptor expression and enhanced pro-protein convertase release, which facilitates viral entrance into host cells, have been associated to specific comorbidities. Comorbid people need careful management and must take preventative measures with awareness. The literature on the correlation between comorbidities and COVID-19 is limited; however, this study demonstrates the wider range of comorbidities associated with COVID-19 patients. For a better understanding of the etiopathogenesis of COVID-19, we included the major comorbidities and a range of clinical complications associated with the virus.
U Bhavana* and Merin Livingston#
Omega College of Pharmacy, India
#Equally contributed towards this article
Introduction
The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection poses a challenge since human’s lack protection and because the receptor binding domain frequently mutates, resulting in the development of novel variations. As of March 7, 2022, 445,096,612 confirmed positive cases and 5,998,301 deaths were documented worldwide, according to the World Health Organisation (WHO). Patients with COVID-19 who also have other medical conditions, or comorbidities, require extra care and counselling to manage their conditions. According to earlier meta-analyses, COVID-19 patients with concomitant conditions such as diabetes, obesity, hypertension, acute renal failure, and respiratory issues presented with severe consequences. Due mostly to the existence of age-related co-existing clinical problems, the elderly group is believed to be at increased risk of severe sequelae and death from SARS-CoV-2. The mortality rate was further elevated in older patients with pre-existing cardiovascular diseases (CVDs), thyroid disorders, diabetes, renal failure, hypertension, cancer, and respiratory diseases, as evidenced by recent studies. These risk factors were also linked to a poor prognosis of the disease. The goal of this thorough analysis is to present a summary of the clinical problems and comorbidities related to the severity of SARS-CoV-2 infection. Additionally, the viral genome, morbidity, mortality, and treatment of COVID-19 patients related to comorbidity variables have been briefly reviewed [1].
The interaction between COVID-19 and comorbidities involves complex mechanisms. Common comorbidities like diabetes, hypertension, and cardiovascular disease can exacerbate the harmful effects of SARS-CoV-2. COVID-19 can lead to a systemic inflammatory response, affecting various organs.
Immune Response: Individuals with comorbidities may have weakened immune responses, making them more susceptible to severe COVID-19. The virus can trigger an overactive immune response, leading to cytokine storms and widespread inflammation. Respiratory System: COVID-19 primarily affects the respiratory system. Comorbidities such as chronic respiratory conditions can impair lung function, increasing the risk of respiratory failure. The virus may cause acute respiratory distress syndrome (ARDS) in severe cases. Cardiovascular System: Pre-existing cardiovascular conditions elevate the risk of complications. COVID-19 can directly impact the heart, causing myocarditis or exacerbating existing cardiac issues. Blood clot formation is another concern, leading to complications like strokes. Metabolic Impact: Diabetes and obesity are associated with worse outcomes. The virus may disrupt glucose metabolism, worsening control in diabetic patients. Obesity-related inflammation can contribute to the overall inflammatory response.
Renal Complications: Kidney damage can occur due to direct viral invasion or as a result of the body’s inflammatory response. Individuals with pre-existing kidney conditions face an increased risk of renal failure. Neurological Effects: COVID-19 may have neurological manifestations. Patients with comorbidities like dementia or neurodegenerative disorders may experience worsened cognitive function, and in severe cases, there could be an increased risk of strokes. Thrombosis and Coagulopathy: COVID-19 can lead to abnormal blood clotting, contributing to complications like deep vein thrombosis (DVT) or pulmonary embolism. Individuals with pre-existing clotting disorders are at higher risk.
Understanding these interactions is crucial for monitoring treatment strategies and identifying individuals at higher risk for severe outcomes. It emphasizes the importance of vaccination and managing comorbidities to reduce the overall impact of COVID-19 [2].
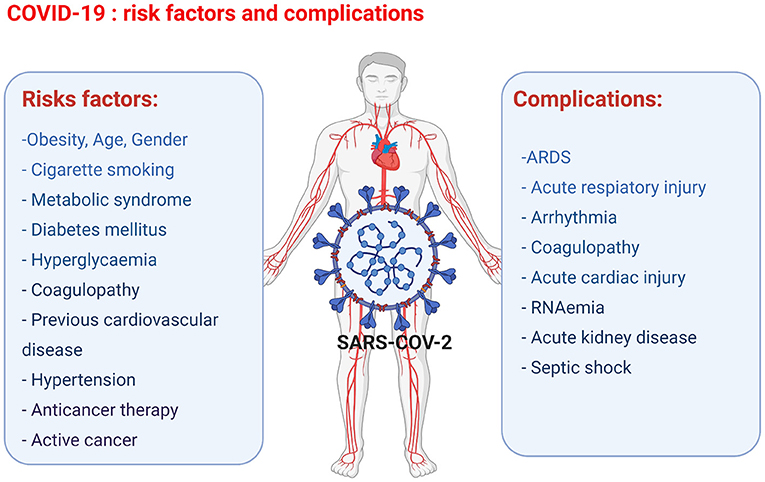
Risks of and Pathogenesis of Covid- 19
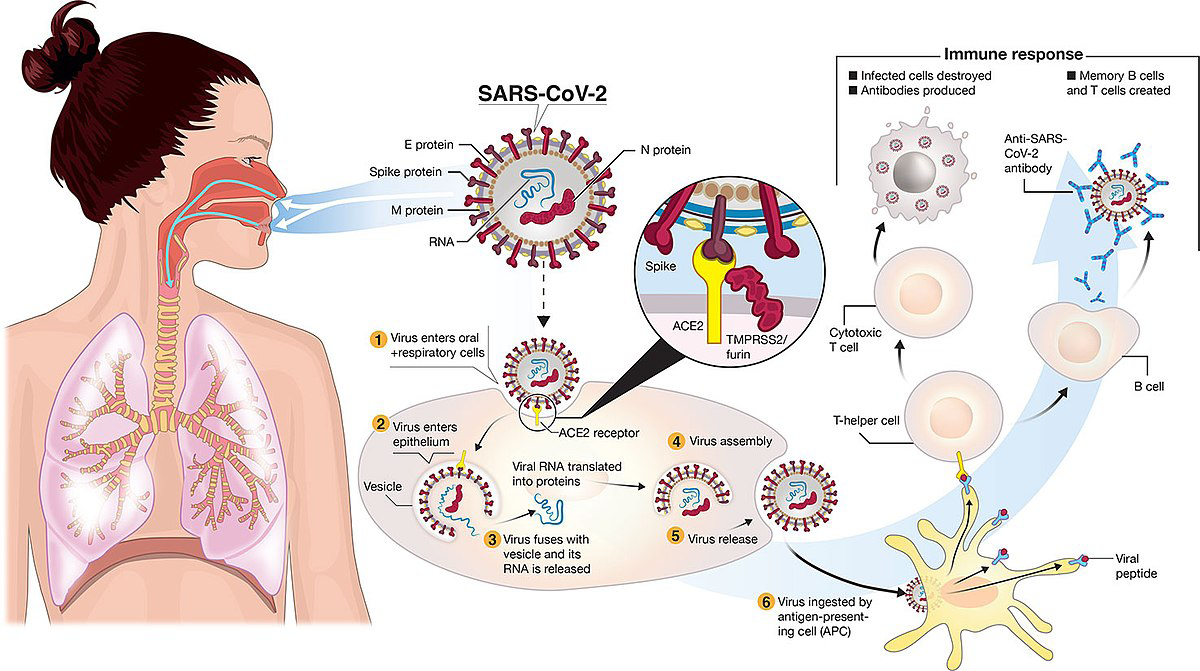
Individuals with comorbidities such diabetes, chronic respiratory disorders, and cardiovascular diseases, as well as those over 60, are more susceptible to contracting SARS- CoV-2 infection. Although the fundamental mechanism of SARS-CoV-2 is still unknown, it is known that the virus enters host cells via binding to ACE-2 receptors on their surface. Patients with COVID-19 who have a high-grade fever and breathing difficulties also have lymphopenia, unusual respiratory symptoms, and high-plasma pro-inflammatory cytokines.
Impact of Comorbidity Factors on Covid-19 Severity
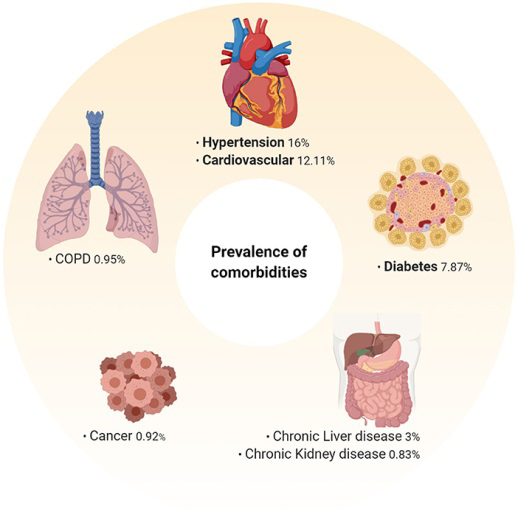
Since the global pandemic has spread, numerous study papers have linked a number of risk factors to the severity of the disease, including higher COVID-19 severity, which is primarily observed in the senior population. Numerous investigations on the comorbidities connected to COVID-19 infection have been reported to date. Comorbidities have been associated to the severity of COVID-19 infection; the most prevalent ones are diabetes, cardiovascular disease, hypertension, cancer, and kidney disease.
Immune Response with Covid 19
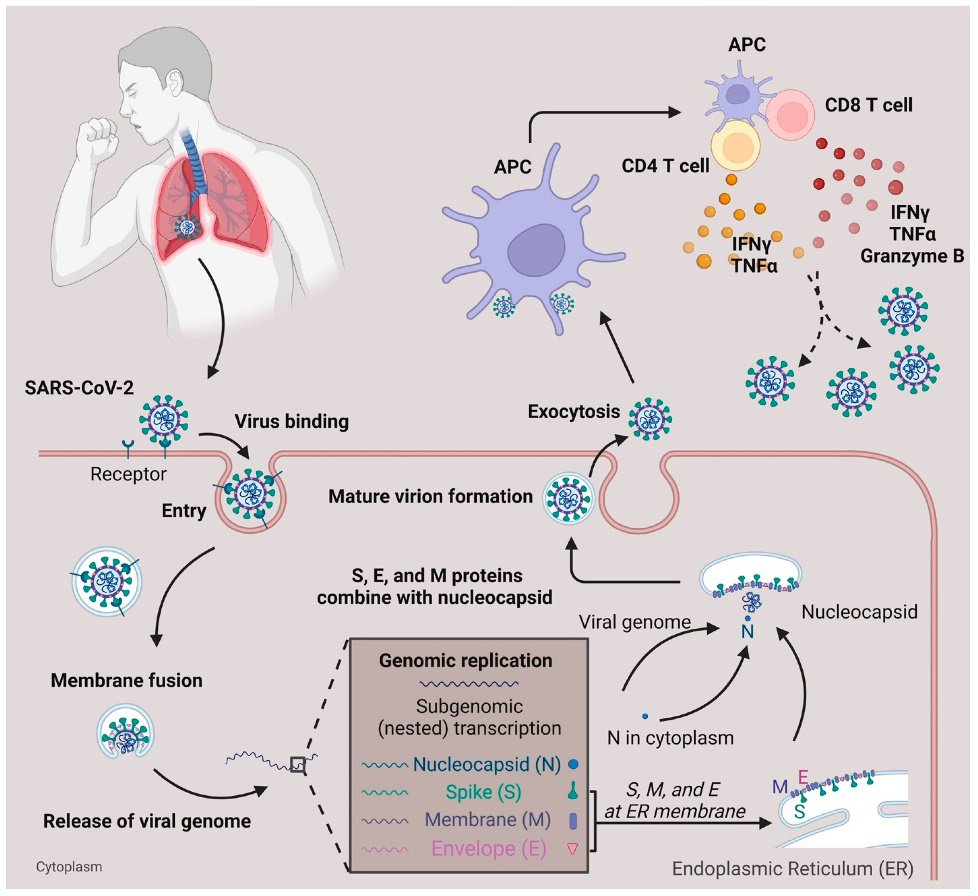
The human body’s first line of defence against the foreign invader is the immune system. Viral proteins cause the host to mount an immunological response upon invasion, which is carried out by host B and T cells and results in the production of antibodies. As a result, the bodies of the hosts release more cytokines. After interacting with the patient’s immune system to induce a range of clinical symptoms, the SARS-CoV-2 virus triggers the inflammatory tissue repair response. As previously mentioned, these reactions may also cause cytokine storms that seriously harm host organs, exacerbating clinical manifestations. The SARS-CoV-2 infection has been associated with various immunological responses, some of which are described below.
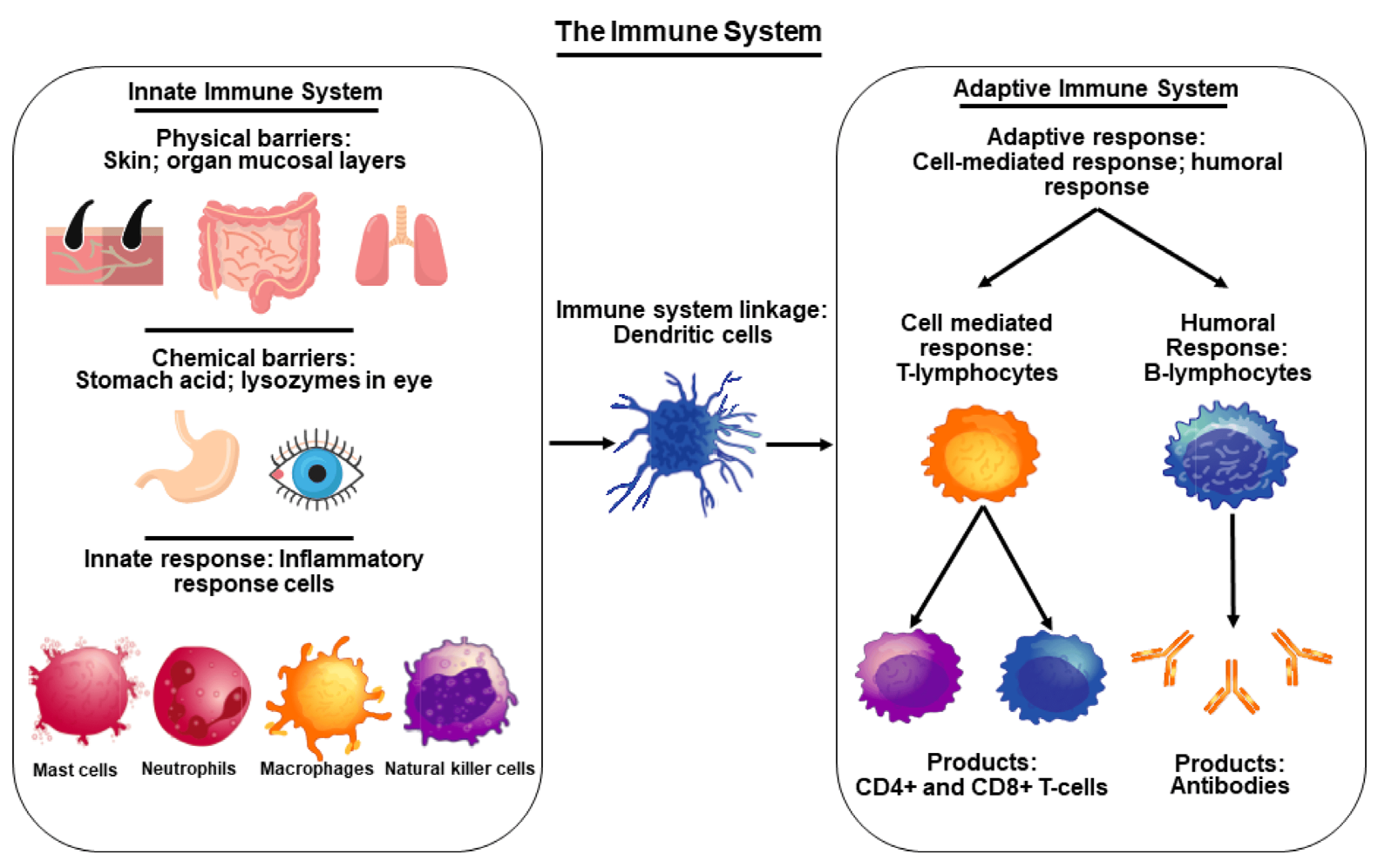
Innate Immune Response
Physical, chemical, and cellular defences against infections are all part of an individual’s innate immune response, which is a type of non-specific immune response that happens naturally. Macrop_h_ages recognise viral invasion through pattern recognition receptors (PRRs), pathogen- associated molecular patterns (PAMPs), or damage- associated molecular patterns (DAMPs), which include node- like receptor (NLR), toll-like receptor 7 (TLR7), and TLR8. The interaction of PRRs with the viral particle activates many cells such as polymorph nuclear leukocytes (PMNs), monocytes, natural killer (NK), and dendritic cells (DC), as well as interferon regulatory factor (IRF), NF-κB, and AP- 1. The subsequent consequences of viral infection on the immune system are reported in a comparison of SARS-CoV-1 and SARS-CoV-2.
It has been shown that both viruses affect the levels of IL- 6, MCP1, CXCL1, CXCL5, and CXCL10/IP10 cytokines in type I and type II pneumocytes that cover air sacs. Moreover, IL-1β, IL-6, TNF, and IL1RA are proinflammatory chemokines that have been shown to be induced in human lung infections.
Respiratory tracts, a mucosa-associated lymphoid tissue (MALT) that serves as a physical barrier to prevent foreign entrance, are where SARS-CoV-2 enters the body. During the first week of SARS-CoV-2 infection, there is a rise in the level of immunoglobulin A (IgA), an antibody produced by the mucosa. According to autopsy data from virus-infected patients, there was a large macrophage infiltration in hemopoietic organs where ACE2 receptor was expressed, such as the spleen and lymph nodes. This resulted in dramatically elevated levels of IL-6, which exacerbated inflammation [3].
Adaptive Immune Response
The adaptive immune system, which is made up of T cells, B lymphocytes, and blood antibodies, takes over if the innate immune system is unable to destroy the foreign organism. The COVID-19 is linked to both humoral immunity and cell-mediated responses. Specifically, viral infection is known to reduce the number of CD8 + T cells, memory CD4 + T cells, and T regulatory cells in the spleen and lymph nodes. Similarly, research has shown that patients infected with the SARS-CoV-2 virus had higher expression of CD94/ NK group 2 member A (NKG2A) on their natural killer (NK) and cytotoxic T lymphocyte (CTL) cells; this expression was subsequently decreased in those who recovered.
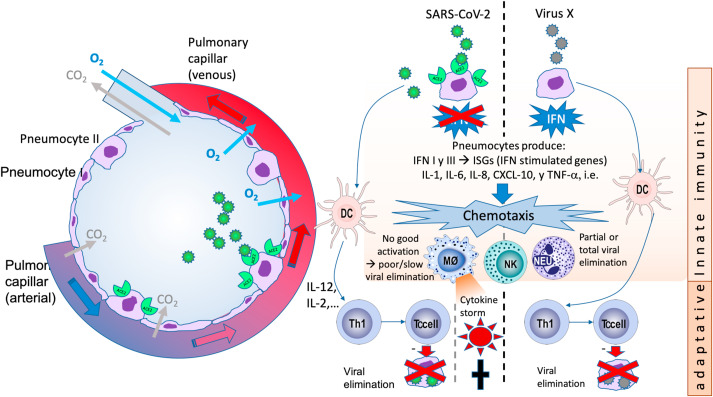
Low levels of cytokines like CD107a, IFN-γ, IL-2, granzyme B, and TNF-α were observed in infected patients. T cells’ memorization of the functional activities following the infection is hence reasonable. Memory T cells stimulate B cells and other immune cells, which then destroy the infected cells. NK-like T cells exhibit the markers CD57 and killer like receptor G1 (KLRG1), which triggers the production of inflammatory cytokines like IFN-γ and subsequently regulates the T cell receptor (TCR) signalling cascade. These results demonstrated that older COVID-19 patients produce aberrant levels of antibodies. According to a study, human CD26 attaches to the S protein of SARS-CoV-2 and produces T cells that are ineffective. T cell activation is facilitated by the CD147 protein, which binds to the S protein’s S1 domain to allow access into the host cell. Abnormal T cell function may result from activation-induced cell death (AICD), which is caused by the binding of SARS-CoV-2 proteins to CD147 and CD26. Nevertheless, a related study notes that MERS-CoV causes T cell death, and COVID-19 patients also experienced this. These findings might provide information on unusual T-cell functioning in those infected with SARS-CoV-2.
Respiratory Disease with Covid-19
Cardiovascular problems are directly correlated with respiratory problems, which turn into a lifelong source of morbidity. Chronic airway inflammation is the hallmark of asthma, the most prevalent respiratory illness. Co-occurring respiratory conditions such as cystic fibrosis, pulmonary hypertension, chronic obstructive pulmonary disease (COPD), asthma, etc. raise the chance of COVID-19 severity. According to other systemic reviews and meta-analyses, COPD raises the risk of COVID-19 individuals by four times, and bronchial asthma enhances the severity of the disease by the same amount. Many patients with chronic SARS-CoV-2 infection have post-COVID respiratory complications; therefore, the National Health Service (NHS) released guidelines for COVID-19 patients who have recovered to identify respiratory symptoms and complications, such as persistent cough, pulmonary oedema, and pulmonary fibrosis. Individuals who are predisposed to asthma are more vulnerable to viral infections.
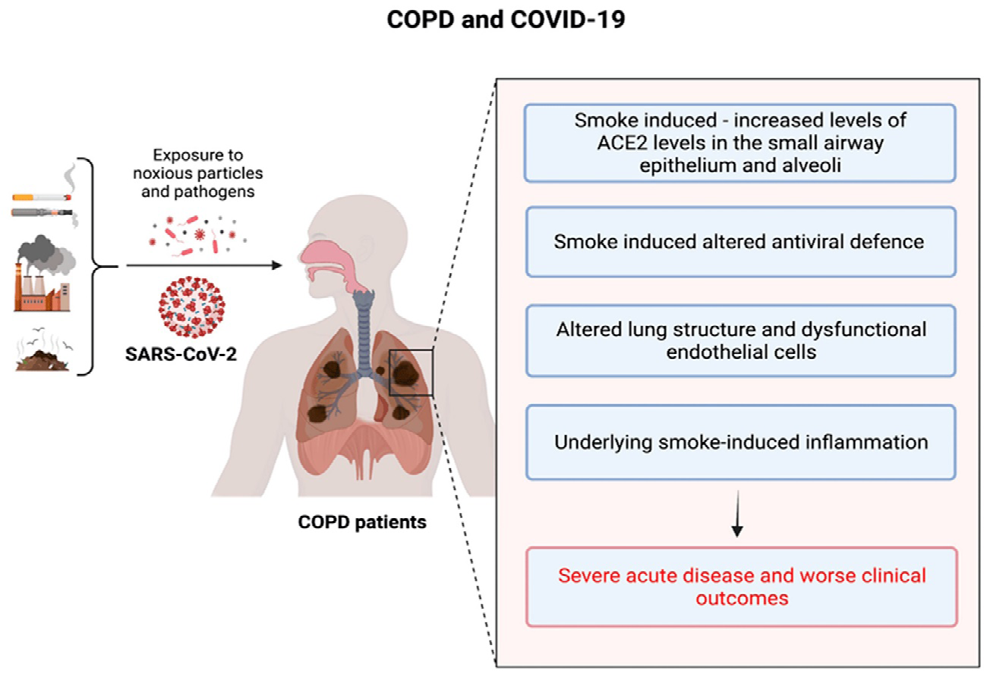
Due to their increased susceptibility to viral infections, individuals with asthma are ultimately more likely to experience a worsening of their condition by impeding IFN-λ release and delaying the antiviral immune response. Simultaneously, an extensive analysis found that older smokers with asthma have a higher chance of having a severe COVID-19. Asthma is not directly related to COVID-19, although it is more likely to be associated with many other diseases and respiratory difficulties. A ventilator is needed for hypoxia in 15–20% of COVID-19 patients. Inhaling corticosteroids, producing a productive cough, weak immunity, cytokine storm, and structural damage to the lung tissues lead to the development of COPD. COPD problems are probably increased when the target protein of the SARS-CoV-2 virus, the ACE2 receptor, is present on pneumocytes [4, 5, 6].
COPD and Covid-19
15% to 20% of patients with COVID-19 disease may develop hypoxemia, which requires ventilator support in challenging circumstances. The development of COPD involves a shift in the inflammatory response, an imbalance in the microbiome, weakened immunity, persistent mucus formation, the use of respiratory corticosteroids, and structural damage. SARS (1.4%) and MERS (13%) infections were also linked to COPD and other chronic illnesses. The expression of ACE-2 receptors is elevated in COPD, despite the fact that previous studies did not report a high number of COVID-19 cases with COPD. This disease may contribute to the development of severe symptoms in COVID-19 individuals, such as lung structural damage, weakened immunity, and excessive mucus production. A significant death rate among these patients is caused by increased mucus production and airway blockage, which were reported in 50–52.3% of all COVID-19 cases admitted to the ICU.
Asthma and Covid-19
The increased risk of viral infections in individuals with asthma has been recognised for about 18 years. These viral infections might manifest serious symptoms if left untreated. Severe problems are more likely to occur in asthmatic patients due to their delayed innate antiviral immune response and reduced IFN-λ secretion. Asthma and other chronic lung problems were linked to MERS (13%), which caused severe symptoms, and SARS (1.4%). Presumably, asthma is one of the major risk factors for COVID-19 based on past records; however, we did not identify any particular SARS-CoV-2 in asthmatic patients. Comparative study of Wuhan’s critical and non-critical COVID-19 patients showed no evidence of a significant correlation between SARS-CoV-2 and self- reported allergies, including food allergies, atopic dermatitis, and allergic rhinitis, as well as asthma. However, smokers who have asthma are more likely to develop serious illness in COVID-19 patients, especially those who are elderly. People with various problems and respiratory disorders are more prone to become entangled during asthma, even though there is no clear correlation between asthma and COVID-19 infections [7].
| Comorbidities | SARS-CoV2 Targets | Symptoms |
|---|---|---|
| Asthma | IFN-λ secretion and the innate antiviral immune response is delayed. | Chronic Respiratory Diseases. |
| COPD | Targets and increases ACE-2 Expression | Severe hypoxemia |
Table 1: SARS-COV2 Targets.
Hypertension and Covid-19
High case fatality rate (CFR) and COVID-19 infection are linked to uncontrolled blood pressure. Because of pandemic fear, 23% of hypertensive COVID-19 cases in China were reported to have 6% CFR. The number of cases also continued to decline. Angiotensin receptor blockers (ARBs) and ACE-2 inhibitors are commonly used as treatments for hypertension in patients. Increased susceptibility to SARS- CoV-2 infection results from the high-dose use of these inhibitors, which upregulate the expression of the ACE-2 receptor. Increased susceptibility to infection, risk of serious lung damage, and the possibility of respiratory failure are all attributed to higher expression of receptor cells on the lungs [8].
However, evidence from preclinical research indicates that ACE-2 is a significant anti-inflammatory and guards against severe COVID-19 consequences such as renal damage, lung injury, and respiratory distress syndrome. Angiotensin II’s inflammatory effect decreased when ACE inhibitors and ARBs are used together. Although it is unclear if using ACE inhibitors or ARBs is beneficial or harmful, using these medications is advised to keep blood pressure within normal ranges. Maintaining blood pressure control should continue to be the primary concern for COVID-19 patients in order to reduce the burden of the disease.
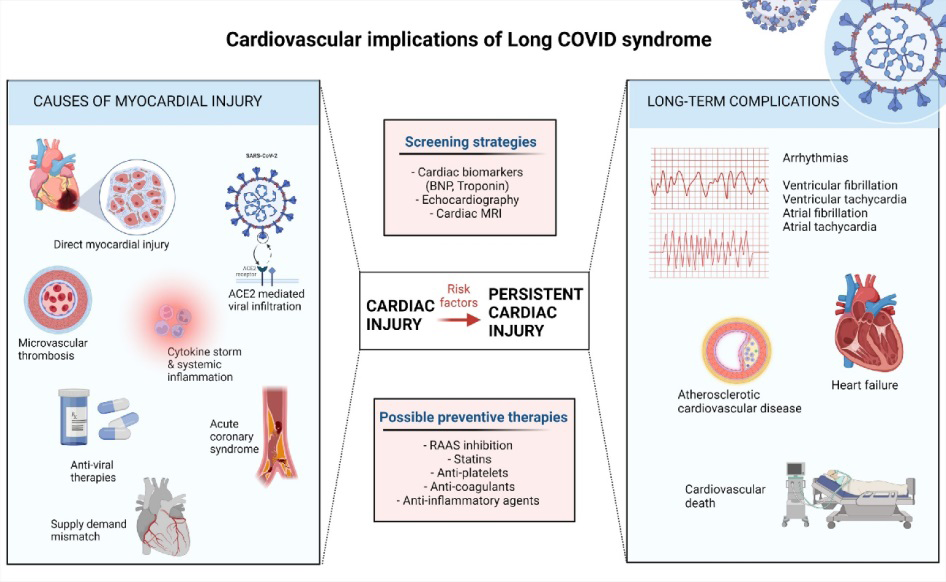
Cardiovascular Disease with Covid 19 and its Complications
Cardiovascular comorbidities such as hypertension and coronary artery disease are linked to increased mortality in individuals with coronavirus disease 2019 (COVID-19). ACE- 2 is a receptor that promotes cardiovascular health. ACE-2 levels in fibroblasts are lower in cardiac patients than in the healthy control group, but they are higher in endothelial cells and cardio myocytes and same increase is seen in the patients with heart failure and aortic stenosis. Viral infection can produce endothelial cell dysfunction, which can lead to microvascular dysfunction and pericyte damage. ACE-2 is downregulated during COVID-19, potentially worsening atherosclerosis and inducing heart dysfunction. Due to the downregulation, angiotensin II accumulates, oxidative stress rises, and NADPH oxidase 2 (Nox2) is activated. Nox2 levels have been linked to troponin increase and occurrences of heart failure which shows a relationship between Nox2 activation and cardiovascular difficulties caused by COVID-19.ACE-2 is similarly downregulated in older adults, exacerbating the severity of their COVID- 19 infection.
Furthermore, COVID-19 infection causes endothelial and vascular damage, which increases the risk of acute coronary syndrome (ACS) and thrombus development in cardiovascular disease patients. In case of hypertension, the vascular endothelium activates monocytes, resulting in practically uncontrollable cytokine release, which has a possible link to COVID-19 and SARS-CoV-2. Fulminant myocarditis can cause over activation of the host’s immunological response, resulting in increased inflammation and impaired heart function. As a result, hypertensive people are more susceptible to serious infections like COVID-19.ACE- 2 is a powerful anti-inflammatory medication that protects against COVID-19’s most prevalent severe consequences, including lung injury, kidney injury, and respiratory distress syndrome. The use of ACE inhibitors and ARBs increases ACE 2, which lowers the inflammatory impact of angiotensin II. It is unclear if the use of ACE inhibitors or ARBs is detrimental or beneficial [9].
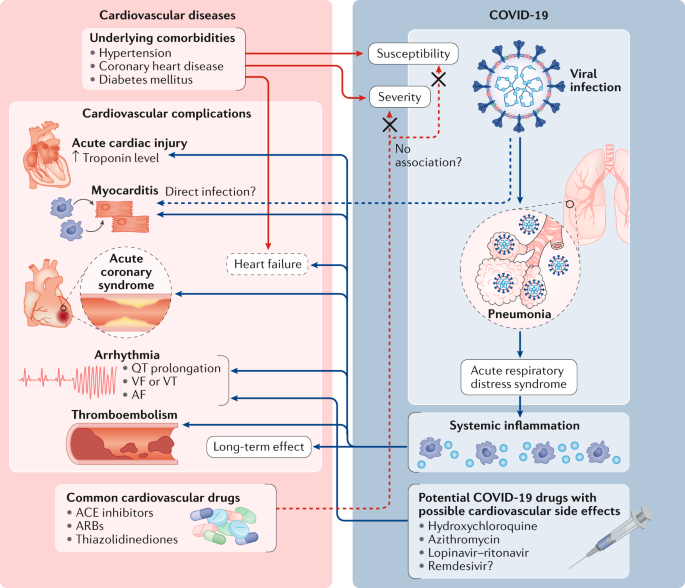
Complications Include Majorly Cardiomyopathy Myocardial infarction Arrhythmias Heart Failure Deep venous thrombosis
| Comorbidities | SARS-CoV2 Targets | Symptoms |
|---|---|---|
| Hypertension | Targets and increases ACE 2 Expression | Elevated Blood Pressure associated with Pneumonia |
| CVD | Compromised Immune response | Myocardial Injury, Heart Attack |
Table 2: SARS-CoV2 Targets.
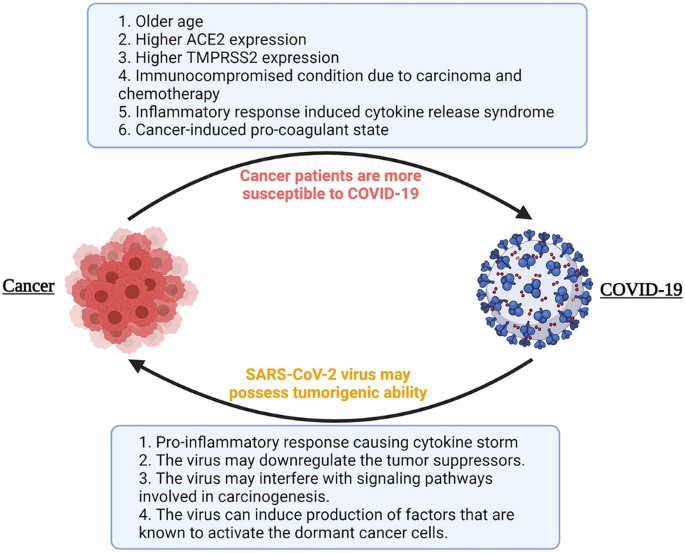
Cancer with Covid 19 and its Complications
Cancer is one of the most well-known and common illnesses that weaken the immune system. Chronic inflammation may be one of the risk factors linked to a higher incidence of COVID-19 in cancer patients. As the tumor grows, it can create obstruction and damage natural innate barriers such as mucosal tissue and the skin, thus increasing the risk of COVID 19 in these people. Prolonged use of corticosteroids, which are given as supportive therapy, can damage adaptive immunity and neutrophil function, increasing the likelihood of COVID- 19 infection.
Cancer patients infected with SARS-CoV-2 may have an increased chance of experiencing myocardial infarctions, septic shock, and ARDS.COVID-19 has been linked to cardiovascular problems in cancer patients include diseases such as embolism, stroke, cardiac damage, and arrhythmias. People with blood cancers may be at higher risk of prolonged infection and death from COVID-19 than people with solid tumors. That is because patients with blood cancers often have abnormal or depleted levels of immune cells that produce antibodies against viruses.
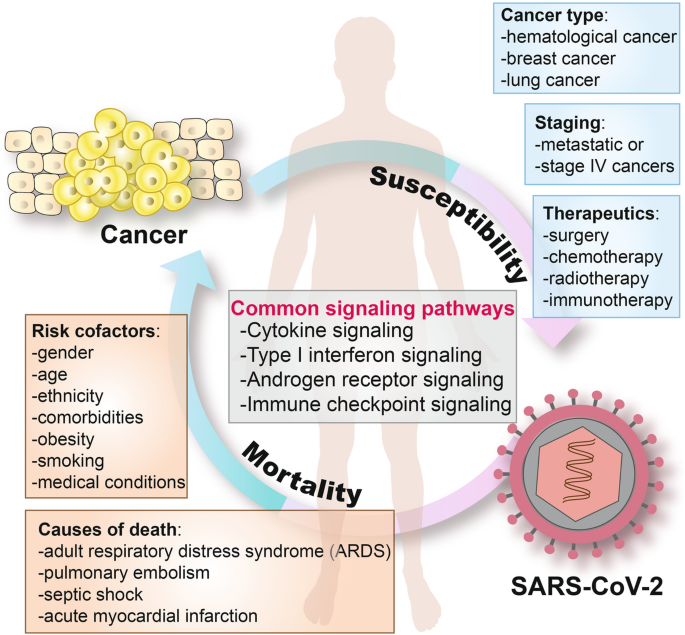
Key Biomarker
C- reactive protein (CRP) is an essential measure of endothelial dysfunction in response to infection and chronic cardiovascular disease. Multiple studies have shown that CRP levels can be utilized to predict the severity of a COVID- 19 infection. These levels may be particularly relevant in the prognosis for COVID-positive cancer patients. CRP should thus be considered as a predictive sign in cancer patients undergoing COVID-19 treatment. Interleukin -6 (IL-6) is a proinflammatory cytokine that regulates fever and acute immunological response, as well as the generation of CRP from the liver. IL-6 has been found to play an important role in severe COVID-19 infection and to have a reliable prognosis. Blocking IL-6 in cancer patients has been shown to be effective when paired with other standard treatments. Tocilizumab, an antibody that has been found to reduce inflammation and mortality rates in COVID-19 patients, can be used to block IL-6. However, inhibiting this pathway may worsen the immunocompromised state and raise the risk of subsequent infection or it may have other unintended consequences.
| SARS-CoV2 Targets | Symptoms | |
|---|---|---|
| Cancer | Compromised Immune System | Respiratory distress syndrome in Adults |
Table 3: SARS-CoV2 Targets.
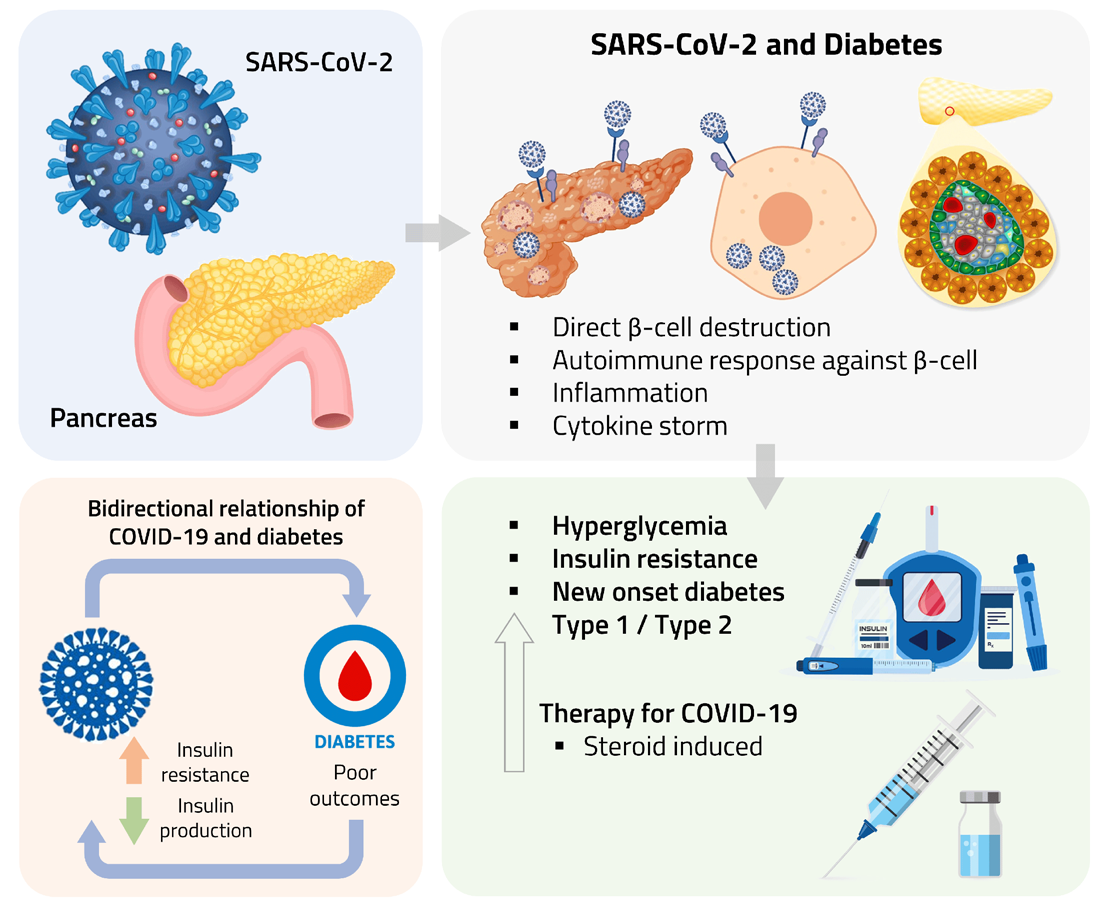
Diabetes Mellitus with Covid19 and its Complications
Diabetes mellitus is a condition defined by glucose dysregulation induced by a lack of insulin. It is classified into several kinds, the most common of which are type 1 diabetes (T1D) and type 2 diabetes. T1D is defined by autoimmune destruction of insulin-producing pancreatic β-cells, while T2D is a mix of β-cell secretory dysfunction and insulin resistance. On basis of Clinical reports from all over the world it is found that diabetes mellitus to be one of the most prevalent comorbidities present in individuals with COVID-19. Diabetes and its related comorbidities raise the probability of a more severe course of COVID-19 and higher mortality rate. COVID-19 is known to worsen glycaemic control in persons with diabetes mellitus. Ketoacidosis is a Complication of type 1 diabetes mellitus (T1DM), it can also occur in persons with T2DM who are suffering with COVID-19. Comorbidities in insulin-resistant individuals, such as hypertension, hyperglycaemia, and diabetes mellitus, contribute to the severity and mortality of COVID-19. Furin is a type 1 membrane bound protease found in high concentrations in diabetic people. This pro protease convertase enzyme helps the virus enter the host cell by reducing SARS-Cov2’s reliance on human proteases. The SARS-Cov2 Spike (S) protein, which attaches to ACE2 receptors, is activated by high amounts of furin. This preactivation of the S protein allows the virus to enter the cell. Increased ACE-2 receptor and furin expression may cause more lung inflammation and lower insulin levels. The ease with which viruses enter the body puts diabetic people at risk of death. Furin is a type 1 membrane bound protease found in high concentrations in diabetic people. This pro protease convertase enzyme helps the virus enter the host cell by reducing SARS-Cov2’s reliance on human proteases. The SARS-Cov2 Spike (S) protein, which attaches to ACE2 receptors, is activated by high amounts of furin. This preactivation of the S protein allows the virus to enter the cell. Increased ACE-2 receptor and furin expression may cause more lung inflammation and lower insulin levels. The ease with which viruses enter the body puts diabetic people at risk of death.
| SARS-CoV2 Targets | Symptoms | |
|---|---|---|
| Diabetes Mellitus | Targets and increases ACE-2 Expression and Interleukin-6 ( IL-6) | Symptoms similar to Pneumonia like Shortness of Breath, Cough |
Table 4: SARS-CoV2 Targets.
HIV with Covid-19
HIV-positive individuals have a heightened susceptibility to COVID-19 infection due to their weakened immune systems. Following the initial documentation of an HIV- affected patient who tested positive for SARS-CoV-2, it was assumed that HIV infection was a susceptible co-occurring condition with COVID- 19. Antiretroviral medications were previously thought to have strong anti- SARS-CoV-2 efficacy, which may account for the decline in SARS-CoV-2 cases among HIV patients [10].
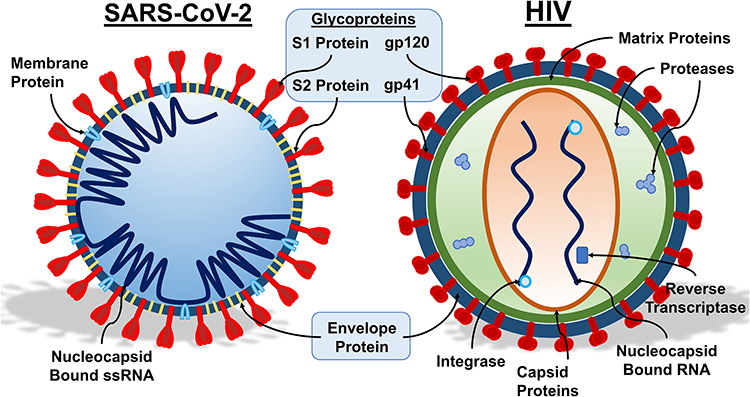
| SARS-CoV2 Targets | Symptoms | |
|---|---|---|
| HIV | Antiretroviral therapy (ART) in combination with a compromised immune system and lung ACE-2 receptor | Pneumonia like Symptoms associated with Jaundice. |
Table 5: SARS-CoV2 Targets.
Impact of Immune Suppression: Research has shown that individuals with HIV, especially those with low CD4 cell counts or not on antiretroviral therapy (ART), may experience more severe COVID-19 outcomes due to compromised immune function. For instance, a study conducted in South Africa found that HIV-positive individuals with low CD4 counts had a higher risk of severe COVID-19 illness and mortality compared to those with higher CD4 counts or HIV-negative individuals [11]. Potential Drug Interactions: Individuals with HIV often take antiretroviral medications, some of which may interact with drugs used to treat COVID-19. For example, there have been concerns about potential interactions between certain protease inhibitors used in HIV treatment and drugs like remdesivir or dexamethasone used in COVID-19 management. Case studies highlighting such interactions and their clinical implications are essential for optimizing treatment regimens in patients with both HIV and COVID-19. Healthcare Access and Disparities: HIV-positive individuals, particularly those from marginalized communities, may face barriers to accessing healthcare services during the COVID-19 pandemic, leading to delays in diagnosis and treatment. Case studies documenting challenges in accessing care and strategies to overcome these barriers can inform interventions to improve healthcare access and outcomes for this population. Vaccine Responses: Studies have shown that HIV infection may impact vaccine responses, raising questions about the effectiveness of COVID-19 vaccines in individuals with HIV. Case studies assessing vaccine efficacy and immune responses in HIV-positive individuals following COVID-19 vaccination can provide valuable insights into vaccine effectiveness and inform vaccination strategies for this population. Long-Term Health Outcomes: Longitudinal studies following HIV-positive individuals who have recovered from COVID-19 can shed light on the long-term health consequences of COVID-19 in this population. Case studies examining post-COVID-19 sequelae, such as persistent respiratory symptoms or organ damage, in individuals with HIV can help identify unique challenges and inform post- acute care strategies.
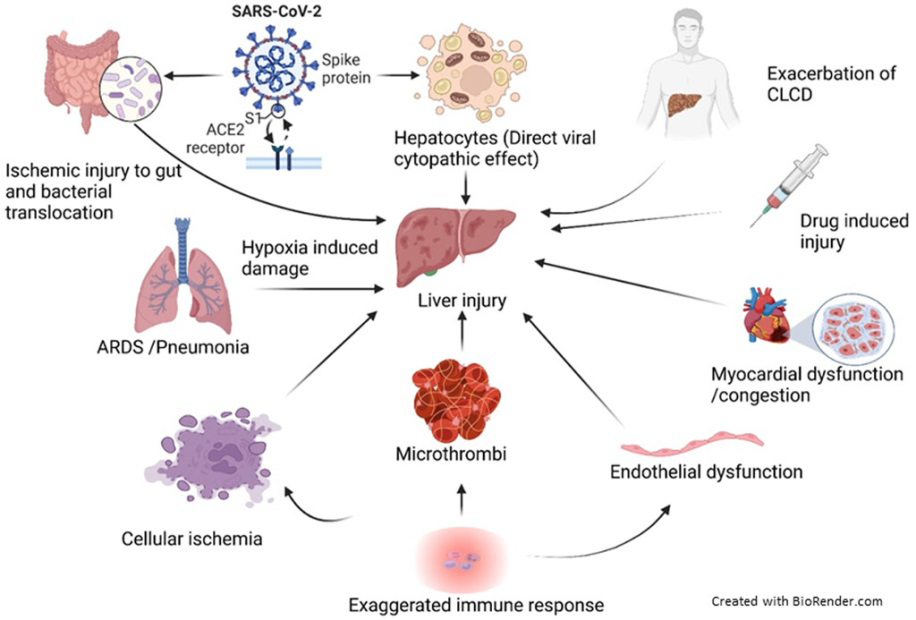
Hepatic Disorders and COVID-19
Atypical liver biochemistry and liver damage have been linked to SARS, MERS, and now COVID-19 infections. It suggests that aberrant liver enzyme release and coronavirus infection are related. SARS-CoV-2 enters the liver cells through ACE-2 receptors that are found on the liver cells. Alanine aminotransferase (ALT), lactic dehydrogenase (LDH), and aspartate aminotransferase (AST) aberrant secretion were linked to 43.4% of COVID-19 patients. However, no patient exhibiting the typical hepatic failure or intrahepatic cholestasis was seen. According to a different study, 6% of COVID-19 patients have elevated bilirubin levels and 39.1% have elevated ALT and AST levels. Approximately 29% of COVID-19 patients show signs of liver damage and experience serious problems as their infections progress. In COVID-19, increased enzymes may be secreted from the body’s muscles and heart in addition to abnormal liver function tests. Blood chemistry alterations typically revert to normal without causing appreciable liver morbidity. In most patients, liver damage manifests as transiently elevated ALT and AST levels without hepatic failure; however, in severe COVID-19 cases, this may be harmful. The underlying mechanisms of liver damage in SARS-CoV-2 infection may include psychological stress, systemic inflammatory response, medication toxicity, and prior hepatic disorders. The pathogenesis of intrahepatic cholestasis or hepatocellular injury is not yet clearly linked to SARS-CoV-2 [12, 13, 14].
Conclusion
In conclusion, comorbidities significantly exacerbate the severity and prognosis of COVID-19, resulting in harmful consequences for infected individuals. Patients with pre-existing conditions such as diabetes, hypertension, cardiovascular diseases, chronic respiratory illnesses, hepatic disorders and immunocompromised states are at heightened risk of developing severe complications from SARS-CoV-2 infection. These comorbidities not only increase susceptibility to the virus but also contribute to a higher likelihood of respiratory failure, multi-organ dysfunction, and mortality.
Furthermore, the conclusion highlights the intricate interplay between comorbidities and the immune response to SARS-CoV-2 infection. Certain comorbidities, particularly those associated with immunosuppression or dysregulation, can compromise the body’s ability to mount an effective immune response against the virus, thereby exacerbating disease progression and increasing susceptibility to complications.
Understanding the interplay between COVID-19 and comorbidities is crucial for healthcare professionals in optimizing patient care strategies, risk assessment, and treatment planning. Comprehensive management approaches should include meticulous monitoring, early intervention, and monitoring therapies to mitigate adverse outcomes in vulnerable populations. Moreover, public health efforts should prioritize preventive measures, including vaccination campaigns and targeted health education initiatives aimed at high-risk individuals, to reduce the burden of comorbidity-related complications associated with COVID-19. By addressing these issues holistically, we can strive towards better outcomes and improved resilience in the face of the ongoing pandemic.
Future research on COVID-19 and comorbidities should focus on:
Future research on COVID-19 and comorbidities should focus on: 1. Long-term health outcomes post-COVID-19. 2. Understanding immune responses in individuals with comorbidities. 3. Exploring genetic predispositions to both COVID-19 and comorbidities. 4. Investigating the impact of medications used for comorbidities on COVID-19 outcomes. 5. Assessing the role of social determinants and behavioral factors. 6. Evaluating the effectiveness of interventions, including vaccines, in high-risk groups. 7. Understanding healthcare system capacity and disparities in outcomes. 8. Adopting a One Health approach to consider interconnected health factors.
In summary, the conclusion underscores the complex relationship between comorbidities and COVID-19, emphasizing the imperative of comprehensive clinical management strategies that address both viral infection and pre-existing health conditions. By recognizing and addressing comorbidities effectively, healthcare providers can improve patient outcomes and mitigate the impact of the COVID-19 pandemic on vulnerable populations.
References
-
Beatty AL, Peyser ND, Butcher XE, Cocohoba JM, Lin F, et al. (2021) Analysis of COVID-19 vaccine type and adverse effects following vaccination. JAMA network open 4(12): e2140364.
-
Hervé C, Laupèze B, Del Giudice G, Didierlaurent AM, Tavares Da Silva F (2019) The how’s and what’s of vaccine reactogenicity. npj Vaccines 4: 39.
-
Ramasamy MN, Minassian AM, Ewer KJ, Flaxman AL, Folegatti PM, et al. (2020) Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime- boost regimen in young and old adults (COV002): a single-blind, randomised, controlled, phase 2/3trial. The Lancet 396(10267): 1979-1993.
-
Jamdade PG, Jamdade SG (2022) Side effects of Covishield vaccine on COVID-positive history family in India. World Journal of Surgical Infection 1(1): 40.
-
Shrisha S Raj, Bhuvana D, Don Selvin (2024) A Novel Face Masks and it’s Utility during COVID-19 Pandemic: A Comprehensive Review. Journal of Quality in Health care & Economics 7(1): 1-7.
-
Dhamanti I, Suwantika AA, Adlia A, Yamani LN, Yakub F (2023) Adverse Reactions of COVID-19 Vaccines: A Scoping Review of Observational Studies. International journal of general medicine 16: 609-618.
-
Hosseini R, Askari NA (2023) review of neurological side effects of COVID-19 vaccination. Eur J Med Res 28(1): 102.
-
Zhao Q, Meng M, Kumar R, Wu Y, Huang J, et al. (2020) The impact of COPD and smoking history on the severity of COVID‐19: A systemic review and meta‐analysis. Journal of Medical Virology 92(10): 1915-1921.
-
Yang J, Zheng Y, Gou X, Pu K, Chen Z, et al. (2020) Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta- analysis. International Journal of Infectious Diseases 94: 91-95.
-
Christensen D, Strange J, Gislason G, Torp‐Pedersen C, Gerds T, et al. (2020) Charlson Comorbidity Index Score and Risk of Severe Outcome and Death in Danish COVID-19 Patients. Journal of General Internal Medicine 35(9): 2801-2803.
-
Krishnasamy N, Natarajan M, Ramachandran A, Thangaraj J, Etherajan T, et al. (2020) Clinical Outcomes among Asymptomatic or Mildly Symptomatic COVID-19 Patients in an Isolation Facility in Chennai, India. The American Journal of Tropical Medicine and Hygiene 104(1): 85-90.
-
Borgoyakova MB, Karpenko L, Rudometov A, Volosnikova E, Merkuleva I, et al. (2022) Self-Assembled Particles Combining SARS-CoV-2 RBD Protein and RBD DNA Vaccine Induce Synergistic Enhancement of the Humoral Response in Mice. International Journal of Molecular Sciences 23(4): 2188.
-
Zhang L, Sun Y, Zeng H, Wang Q, Jiang X, et al. (2020) Calcium channel blocker amlodipine besylate therapy is associated with reduced case fatality rate of COVID-19 patients with hypertension. Cell Discovery 6(1): 96.
-
Guan W, Liang W, Zhao Y, Liang H, Chen Z, et al. (2020) Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. The European Respiratory Journal 55(5): 2000547.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet