Pulmonary Carcinosarcoma with Rhabdoid Differentiation and Widespread Dissemination in a Cat
We report a pulmonary carcinosarcoma with metastasis and severe hydrothorax in a 20-year-old, neutered male, Domestic Shorthair cat (Felis catus). The cat was found dead without previous clinical signs. The pulmonary tumor displayed malignant epithelial acinar and papillary patterns, as well as sarcomatous features with rhabdoid and spindle-shaped differentiation. Distinct components of the neoplasm showed immunohistochemical staining for cytokeratin, desmin, and vimentin. The pulmonary neoplasm disseminated to the heart, colon, mesenteric lymph node, pancreas, omentum, and mediastinum. Most metastases primarily displayed rhabdoid features; however, the tumor cells also formed epithelial acini in the myocardium. The cause of death was likely associated with impairment of the cardiorespiratory function from the pulmonary lesions, metastasis to the heart, and severe hydrothorax. Carcinosarcomas have been rarely reported in domestic animals and are more thoroughly described in humans.
Introduction
Feline primary lung tumors are uncommon and represent approximately 0.7% of all neoplasms [1]. These tumors are more commonly diagnosed in older cats at an average of 12 years old [1]. Pulmonary adenocarcinomas are the most frequent tumors, followed by squamous or adenosquamous carcinomas; lung tumors have a high rate of metastasis in cats [1, 2]. By contrast, sarcomas arising from the lung are rare [2].
Pulmonary carcinosarcomas are exceedingly rare in cats and other domestic species. These biphasic neoplasms contain both malignant epithelial and mesenchymal features. Carcinosarcomas have been reported in other tissues of cats, originating from the pancreas [3], biliary system [4], mammary gland [5], thyroid gland [6], mouth [7], and uterus [8]. Here, we describe a primary pulmonary carcinosarcoma in a cat with features of a pulmonary adenocarcinoma, rhabdomyosarcoma, and non-rhabdoid mesenchymal type with metastasis to multiple distant sites.
A 20-year-old, neutered male, orange, and white Domestic Shorthair cat (Felis catus) was presented dead at the Veterinary Medical Centre in Saskatoon, Canada. The owners reported that this outdoor cat was doing well just prior to being found deceased the next morning.
A necropsy was performed at Prairie Diagnostic Services (Saskatoon, Canada). The cat was in good body condition and weighed 5.8 kg. The entire length of the tracheal lumen had white foam in the lumen and the thoracic cavity contained
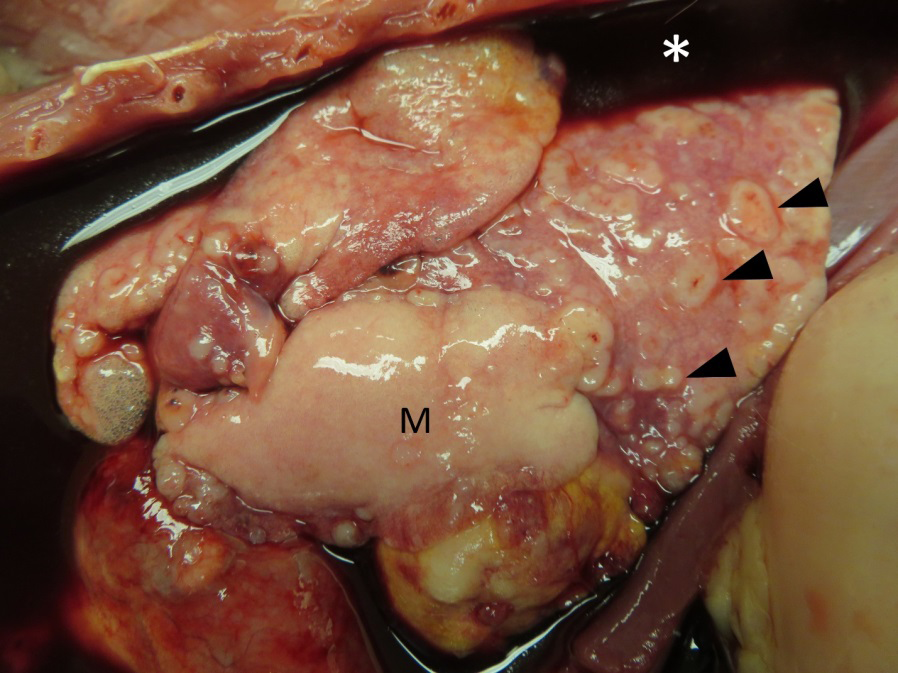
100 mL of red-tinged, watery fluid. In the left caudal lung lobe, there was a firm, white nodular mass measuring 3 x 3 x 3 cm (Figure 1). The other lung lobes had numerous umbilicated, white nodules ranging from 0.1-0.5 cm in diameter. The ventral and caudal mediastinum displayed confluent red tissue masses with crepitant texture. In the left ventricular wall of the heart, the myocardium was partially replaced by a 2 cm in diameter, white, firm mass. The left auricle showed a 0.5 cm, white, firm nodule. The wall of the descending colon was focally replaced by a 0.5 x 0.3 x 0.5 cm, raised, white, firm, nodular mass.
Affected tissues were fixed in 10% neutral-buffered formalin for 24 hours, paraffin embedded, sectioned at 5 µm, and then stained with hematoxylin and eosin. Immunohistochemistry was performed using antibodies against cytokeratin (AE1/AE3), vimentin, and desmin intermediate filaments.
Histologically, approximately 60-70% of the pulmonary parenchyma was effaced by multiple, variably sized, unencapsulated, poorly demarcated, densely cellular areas of neoplastic tissue displaying biphasic morphology. The neoplasm was composed of acinar and papillary structures lined by single to multiple layers of neoplastic epithelial cells; these structures were interspersed in some areas with solid sheets or interlacing bundles of neoplastic mesenchymal cells with round to polygonal, or spindle shapes, respectively (Figure 2). The epithelial cells were cuboidal to columnar with abundant, well-defined, eosinophilic cytoplasm; their nuclei were central with finely stippled chromatin, usually with a single prominent magenta nucleolus. There was moderate to marked anisocytosis and anisokaryosis. A total of 3 mitotic figures were counted in 10 high-power fields (2.37 mm2) within the neoplastic epithelial component. Frequently, the alveolar-like structures contained sloughed neoplastic cells with marked atypia. The neoplastic spindle-shaped cells had indistinct borders and moderate amounts of fibrillar eosinophilic cytoplasm; their nuclei were oval to elongated with finely stippled chromatin and variably distinct nucleoli. In some areas, these cells contained elongated hypereosinophilic cytoplasm and multiple nuclei arranged in rows (rhabdoid appearance). The round to polygonal neoplastic cells often contained eccentric nuclei and moderate amounts of deeply eosinophilic stringy cytoplasm (also interpreted as rhabdoid appearance). The mitotic count was markedly higher than the one in the epithelial component. Extensive areas of coagulative necrosis, mineralization, and rare acicular spaces (cholesterol clefts) were present within the neoplasm. Several blood vessels were occluded by tumor cell emboli.
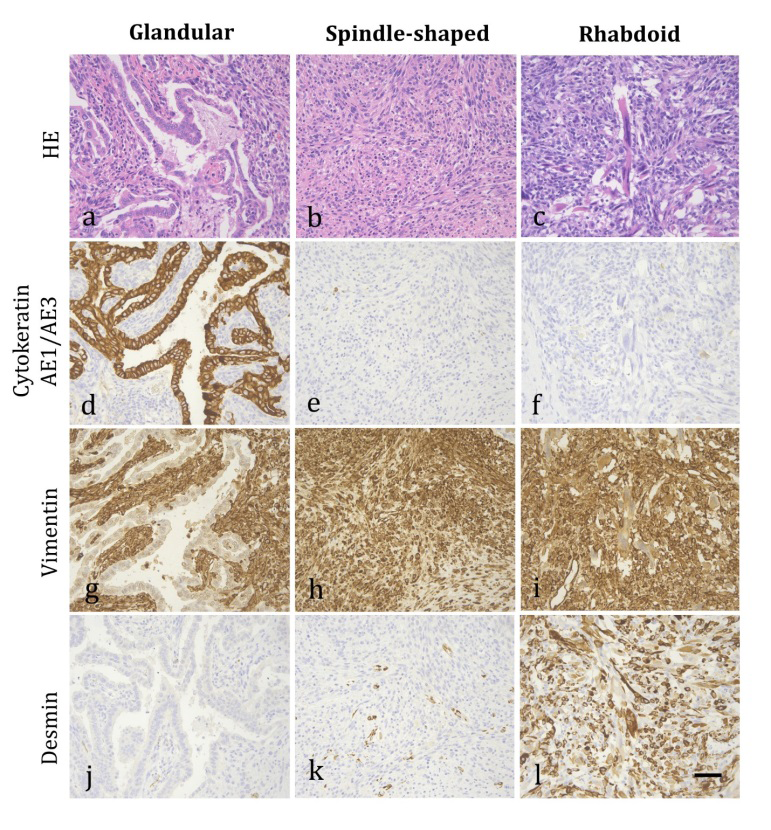
Figure 2: Pulmonary carcinosarcoma in a cat. Multifocal regions within the lung tumor display distinct morphologies: (a, d, g, j) glandular patterns, adjacent to spindle-shaped neoplastic cells; (b, e, h, k) spindle-shaped neoplastic cells forming interlacing bundles and streams; and (c, f, i, l) rhabdoid differentiation with elongated, brightly eosinophilic cytoplasm and rows of nuclei. Immunohistochemistry was performed to highlight these different morphologies, using the following antibodies: (d, e, f) anti-cytokeratin AE1/AE3; (g, h, i) anti-vimentin; and (j, k, l) anti-desmin. HE = hematoxylin and eosin. Scale bar = 50 µm.
The colon, mesenteric lymph node, pancreas, omentum, and mediastinal lesions were metastases with similar rhabdoid features as those described in the lung tumor (Figure 3). A total of 44 mitotic figures were counted in 10 high-power fields in the colonic tumor. In the heart, 30% of the left ventricular myocardium was effaced by neoplastic tissue with similar mesenchymal (rhabdoid and spindloid) characteristics as described in the lung. Scattered throughout the sheets of mesenchymal tumor cells, there was a moderate number of acinar structures lined by neoplastic epithelial cells (Figure 4). A similar infiltrative tumor partially effaced the wall of the left auricle and extended into the chamber lumen.
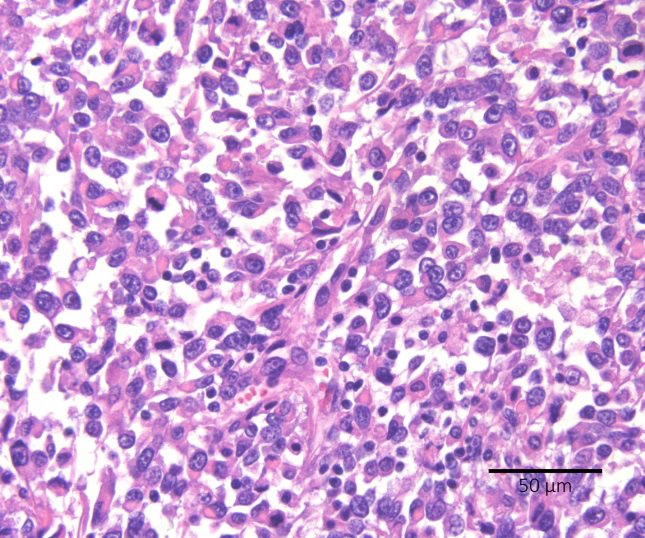
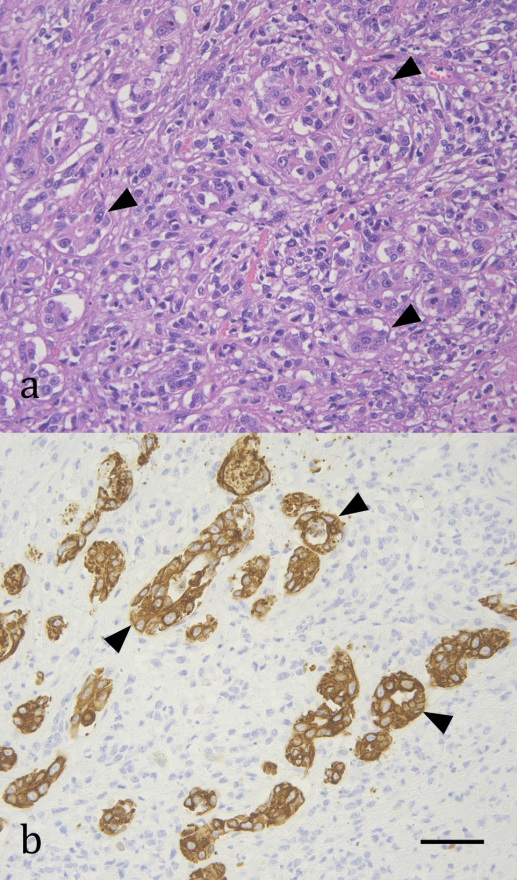
Figure 4: Carcinosarcoma metastasis to the left ventricular myocardium in the heart of a cat. (a) Epithelial components form acinar-like structures (arrowheads). Hematoxylin & eosin. (b) The epithelial cells that form the acini (arrowheads) are strongly positive for a broad keratin marker. Immunohistochemical antibody anti-cytokeratin AE1/AE3. Scale bar = 50 μm.
The neoplastic epithelial, rhabdoid, and spindle-shaped cells in the lung displayed different immunohistochemical marker expressions. The neoplastic epithelial cells showed strong intensity staining to a broad cytokeratin marker and were negative for desmin and vimentin (Figure 2). By contrast, cells with rhabdoid appearance exhibited strong intensity staining to desmin and vimentin; spindle-shaped cells in other areas of mesenchymal differentiation were negative for desmin. Overall, the mesenchymal (rhabdoid and spindle-shaped) cells were negative for cytokeratin AE1/AE3.
Based on the biphasic histomorphology of the large pulmonary neoplasm, characterized by the presence of malignant epithelial and sarcomatous components confirmed by immunohistochemistry, the diagnosis of pulmonary carcinosarcoma was made in this cat. The pulmonary neoplasm was widely disseminated, involving multiple tissues and organs within the thoracic and abdominal cavities.
Discussion
This case report describes the postmortem, histologic, and immunohistochemical features of a pulmonary carcinosarcoma with widespread dissemination in a cat. The cause of death in this animal was attributed to severe impairment of the cardiorespiratory function caused by extensive replacement of the pulmonary parenchyma and left ventricular myocardium; a significant accumulation of fluid in the thoracic cavity may have also contributed to the cardiorespiratory failure. Carcinomas have been identified to cause approximately 40% of cases of pleural effusion associated with neoplasia in cats [9]. Surprisingly, no signs of respiratory distress were reported prior to death in this cat; in addition, the animal was in good body condition despite the widespread neoplastic dissemination, hydrothorax, and advanced age. Cats with primary lung tumors have been reported to display highly variable respiratory signs, with almost 40% having no clinical signs [2]. Affected cats, typically exhibit nonspecific clinical signs such as weight loss, dyspnea, and lethargy [2].
To the authors’ knowledge, only a single case of pulmonary carcinosarcoma has been previously reported in a cat [10]. Our case differs in that the sarcomatous component displayed skeletal muscle differentiation (rhabdomyosarcoma). Heterologous elements are considered a key feature distinguishing carcinosarcomas from sarcomatoid or spindle cell carcinomas according to the WHO classification of mixed pulmonary tumors [11]. In our case, there were intrapulmonary, intrathoracic (cardiac and mediastinal), and extrathoracic metastases that primarily displayed sarcomatous (rhabdoid) features. The cardiac metastasis in this cat also exhibited a carcinomatous component. By contrast, the previous report described only intrapulmonary metastasis with an undifferentiated spindle- cell population [10].
There is one report of pulmonary carcinosarcoma in dogs that displayed additional heterologous elements including a sarcomatous component with osteoid and chondroid metaplasia, and a carcinomatous component with squamous and acinar differentiation [12].
Hypotheses for the Histogenesis of Carcinosarcomas Include: (1) the collision of two independent tumors forming a single neoplasm; (2) the sarcomatous component of these tumors originate from the carcinomatous component (i.e., epithelial-to-mesenchymal transition); (3) a common stem cell showing differentiation into epithelial and mesenchymal cells early in the development of the tumor; and (4) a carcinoma with pseudosarcomatous stromal reaction [10, 13]. The different morphologic components of the tumor had separate immunohistochemical staining in our case; therefore, we can speculate that the epithelial and mesenchymal components may have derived from a single pluripotential stem cell. Given that the occurrence of primary pulmonary sarcomas is extremely rare in cats, the possibility of a collision tumor is unlikely in our case; however, the chance of an extrapulmonary sarcoma with metastasis to the lungs, forming a collision tumor with a preexisting pulmonary carcinoma cannot be ruled out (i.e., tumor-to- tumor metastasis). Tumor-to-tumor metastasis has been rarely described in people [14] and once in a dog [15]. The hypothesis of a carcinoma with pseudosarcomatous stromal reaction can be ruled out in our cat, considering the presence of metastases of the sarcomatous component at multiple sites. In addition, the probability of a pleomorphic carcinoma was initially considered; however, this differential diagnosis was excluded due to the presence of heterologous elements within the mesenchymal component.
In people, pulmonary carcinosarcomas are also considered rare and comprise <1% of all lung tumor diagnoses [16]. In contrast to the histologic features in this case, the epithelial component in humans most frequently exhibits squamous differentiation, followed by a glandular pattern (adenocarcinoma), and the sarcomatous elements tend to show chondrogenic or osteogenic differentiation [16]. Human patients had a median survival time of 9 months [16]. Prognosis is considered poor due to a high tendency to metastasize and locally recur; in one case series, metastases only contained the sarcomatous component of the neoplasm [17]. Given the paucity of pulmonary carcinosarcomas cases reported in veterinary literature, little is known about the clinical, epidemiologic, and prognostic factors in cats or other domestic animals.
Conclusion
Pulmonary carcinosarcomas, which are rare malignant neoplasms in cats and other domestic animals, display biphasic differentiation towards carcinomatous and sarcomatous (often heterologous) elements. Histopathology and immunohistochemistry tests with differential expression of markers on the different tissue components are necessary to confirm the diagnosis. This report highlights the rhabdoid differentiation of the sarcomatous component and glandular patterns of the epithelial element in a feline pulmonary carcinosarcoma with widespread metastases. Pulmonary carcinosarcoma should be considered in the differential diagnosis of malignant pulmonary neoplasms with metastatic potential in cats.
Acknowledgments
We kindly thank Jayme Bratsberg and Avery Chora for their assistance in the necropsy of this cat. We also thank the necropsy, histology, and immunohistochemistry technicians at Prairie Diagnostic Services, and the Department of Veterinary Pathology at the Western College of Veterinary Medicine, University of Saskatchewan, Canada.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Costa SD, Yoon BI, Kim DY, Motsinger-Reif AA, Williams M, et al. (2012) Morphologic and Molecular Analysis of 39 Spontaneous Feline Pulmonary Carcinomas. Vet Pathol 49(6): 971-978.
-
Hahn KA, McEntee MF (1979) Primary lung tumors in cats: 86 cases (1979-1994). J Am Vet Med Assoc 211(10): 1257-1260.
-
Yamamoto R, Suzuki K, Uchida K, Onda N, Shibutani M, et al. (2012) Pancreatic Carcinosarcoma in a Cat. J Comp Pathol 147(2–3): 223-226.
-
Laura C, Silvia F, Carolina C, Edoardo A, Zini Eric, et al. (2013) Carcinosarcoma of the biliary system in a cat. Journal of Veterinary Diagnostic Investigation 25(5): 562-565.
-
Sammarco A, Finesso G, Zanetti R, Ferro S, Rasotto R, et al. (2020) Biphasic Feline Mammary Carcinomas Including Carcinoma and Malignant Myoepithelioma. Vet Pathol 57(3): 377-387.
-
Rich AF, Piviani M, Swales H, Finotello R, Blundell R (2019) Bilateral Thyroid Carcinosarcoma in a Cat. J Comp Pathol 171: 24-29.
-
Malatesta D, Defourny SVP, eodoro GD, Seca F, Guardiani P, et al. (2022) Morphological and Immunohistochemical Characterization of an Oral Metastatic Carcinosarcoma in a Cat. J Comp Pathol 199: 17-22.
-
Murakami M, Yonemaru K, Goto M, Owaki K, Hirata A, et al, (2022) Feline uterine carcinosarcoma infiltrated with osteoclast-like giant cells. Journal of Veterinary Medical Science 84(12): 1579-1584.
-
Ruiz MD, Vessières F, Ragetly GR, Hernandez JL (2018) Characterization of and factors associated with causes of pleural effusion in cats. JAVMA 253(2): 181-187.
-
Ghisleni G, Grieco V, Mazzotti M, Caniatti M, Roccabianca P, et al. (2003) Pulmonary carcinosarcoma in a cat. J Vet Diagn Invest 15(2): 170-173.
-
Guarino AL, Jeon AB, Abbott JR, Hill RC (2021) Pulmonary Sarcomatoid Carcinoma Associated with Arterial Thromboembolism in a Cat. Case Rep Vet Med.
-
Salas G, Román O, Díaz-Ceballos MEG, Constantino F (2002) Lung carcinosarcoma in a dog: Gross and microscopic examination. Veterinary Journal 163(3): 331-334.
-
McCluggage WG (2002) Malignant biphasic uterine tumours: carcinosarcomas or metaplastic carcinomas?. J Clin Pathol 55(5): 321-325.
-
Lee T, Cha YJ, Ahn S, Han J, Shim YM (2015) A rare case of tumor-to-tumor metastasis of thyroid papillary carcinoma within a pulmonary adenocarcinoma. J Pathol Transl Med 49(1): 78-80.
-
Hilbe M, Hauser B, Zlinszky K, Ehrensperger F (2002) Haemangiosarcoma with a metastasis of a malignant mixed mammary gland tumour in a dog. J Vet Med A Physiol Pathol Clin Med 49(8): 443-444.
-
Sökücü SN, Kocatürk C, Urer N, Sönmezoğlu Y, Dalar L, et al. (2012) Evaluation of six patients with pulmonary carcinosarcoma with a literature review. The Scientific World Journal.
-
Huwer H, Kalweit G, Straub U, Feindt P, Volkmer I, et al. (1996) Pulmonary carcinosarcoma: diagnostic problems and determinants of the prognosis. Eur J Cardio-thorac Surg 10(6): 403-407.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet