Serum Vitamin D Level in Asthmatic Children and its Impact on Asthma Severity at a Tertiary Care Hospital in Bangladesh
Background: Asthma is a chronic disease that impacts children’s physical, social and emotional health. Over the past few decades, vitamin D deficiency and insufficiency have increased in the general population and have been associated with respiratory illnesses including asthma. This study compared blood vitamin D levels in asthmatic and non-asthmatic children to investigate if vitamin D insufficiency is linked to different asthma subtypes. Methods and Materials: This cross-sectional study was conducted department of paediatrics of Bangabandhu Sheikh Mujib Medical University from october 2020 to october 2021. Based on predetermined inclusion and exclusion criteria, 60 newly diagnosed children with asthma between the ages of 8 and 18 were enrolled as case. Age and sex matched 30 non-asthmatic children were taken as control. All children’s serum 25(OH)D levels were estimated, and the results between the two groups were compared. In children with asthma, the relationship between vitamin D levels and certain clinical forms of asthma was investigated. Results: Asthmatic and non-asthmatic children had mean ages of 11.32±2.007 and 11.07±1.938, respectively. In the asthma group, 26.7% had intermittent asthma, 30.0% had mild asthma, 28.3% had moderate asthma, and 15.0% had severe asthma. Among them, 23.3% were vitamin D deficient, 53.3% were vitamin D insufficient, and 23.3% were vitamin D sufficient. In the group without asthma, 13.3% had vitamin D deficiency and 40.0% had vitamin D insufficiency. 46.7% possessed a sufficient amount. Vitamin D levels were substantially lower in asthmatic children than in non-asthmatic children (24.77.1 vs. 35.97.6). Serum vitamin D levels had no effect on the various clinical categories of asthma. Conclusion: Children with asthma significantly lower mean serum vitamin D levels when compared with their counterparts without asthma.
Introduction
Asthma is a chronic inflammatory airway disorder. Acute attack of these episodes is not same for everyone and can range in intensity and frequency. These episodes are linked to varying degrees of airflow restriction, which typically resolve on their own or with therapy. The involvement of genetic and environmental variables, as well as the activation of cells in the innate and adaptive immune systems, leads to the major pathologic alterations seen in asthma [1].
As a significant global public health issue, around 339 million people are thought to have asthma globally and another 100 million will be impacted by 2025 [2]. The prevalence of asthma in school-aged children varied greatly throughout Southeast Asia, including China (1-2.4%), Hong Kong (7.2-8%), Indonesia (2.3-8.2%), Malaysia (13.8%), and India (7.2%) [3]. In Bangladesh, 7.4 percent of all children (under 15 years of age) and 7 million people (5.2% of the population) currently have asthma [4] (defined as at least three attacks in the previous 12 months).
More than 90% of asthma patients in Bangladesh do not receive current therapy [5]. Asthma control is not optimal in majority due to improper application of treatment recommendations [6]. This can result in episodes of exacerbation and irreversible airway remodeling that makes asthma treatment less effective. Asthma is thought to be responsible for between 250,000 to 345,000 annual deaths worldwide, or over 1000 per day [7].
Asthma imposes burden on healthcare systems and society which in turn responsible for economic losses and barriers to implementing guidelines [8]. Consequently, innovative, practical approaches must be designed and evaluated to ensure asthma patients best possible care [9]. One such area of potential research is the role of vitamin D in asthma control.
Vitamin D deficiency is a significant risk factor for several chronic diseases, including asthma [10, 11, 12, 13]. Low vitamin D levels may reduce the efficacy of steroid by loss of synergistic action on p38 MAPK [14], promotes inflammation, and its supplementation may halt this inflammatory process [1, 13, 15, 16, 17, 18].
Several studies have identified a link between vitamin D deficiency and poor outcome of lung function in a patient with asthma [18, 19, 20]. Even low maternal vitamin D intake during pregnancy leads to an increased possibility of wheezing in children [20, 21]. A Costa Rican study reported that vitamin D level was inversely related to asthma severity [22]. Another study showed that 48% of children with asthma, atopic dermatitis, and food allergy had insufficient vitamin D levels and its supplementation reduces the rate of asthma exacerbation [23].
Vitamin D is a fat-soluble vitamin obtained from skin exposure to ultraviolet B (UVB) light or dietary intake [13, 24]. It is metabolized in the liver to 25-hydroxy-vitamin D [25(OH)D] [10]. Different gene polymorphisms of vitamin D receptor (VDR) and vitamin D binding proteins (VDBPs) were linked to increased susceptibility to asthma [25]. The activation of the vitamin D receptor (VDR) has an immunomodulatory effect on an immune cells including dendritic cells (DCs), macrophages, B and T lymphocytes and structural cells in the airways, preventing airway hyper- responsiveness [1, 16, 17, 26, 27, 28].
Vitamin D is also essential in reducing the risk for respiratory infections, which is a major triggering factor for asthma [29, 30].
There is a lack of data on serum vitamin D levels in Bangladeshi children with asthma. So, this study aimed to assess serum vitamin D levels in children with asthma and the association between vitamin D and different clinical categories of asthma.
Methods
It was a cross-sectional study that took place in the Department of Paediatrics at Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, from October 2020 to October 2021.
This study includes 60 newly diagnosed asthmatic children aged 8–18 year as per GINA guideline as case. Thirty (30) age and sex matched non-asthmatic children was included as control group in this study. Children who got vitamin D supplements in last three months and had any medications in the last 1year that affect vitamin D levels (e.g, systemic steroid, phenytoin, carbamazepine, cyclophosphamide, cotrimazole, rifampicin, nfidipines, diuretics) were excluded from the study. Children with chronic musculoskeletal or endocrine disorder or having known renal, liver or intestinal disease were also excluded from the study.
Informed written consent was taken from the parents or guardians and IRB clearance was taken from institutional review board before conducting the study. Data were collected in predesigned collecting sheet. Information on socio-demographic history, asthma symptoms, atopy, vitamin D supplementation, pharmacological history, and the characteristics of vitamin D deficiency disease had taken. In each case, a complete clinical examination was performed, paying particular attention to any clinical indications of vitamin D insufficiency or asthma. All asthmatic children underwent the bronchodilator reversibility test using a peak flow meter. Spirometry could not be done due to COVID situation. Patient got asthma treatment as per standard protocol according to the disease severity after diagnosis was made.
Using a disposable syringe and all necessary aseptic measures, 2 ml of free flow venous blood was collected from the antecubital vein. Within 30-120 minutes of collection, serum was separated by centrifugation (5 min, 3000 rpm). The Department of Biochemistry and Molecular Biology, BSMMU, used the Chemiluminescence Microparticle Immunoassay (CMIA) approach with the analyzer Architect Abott, Ci 4100, USA2012 to measure serum vitamin D (25 hydroxy vitaminD). SPSS 26.0 was used to perform all statistical computations. For qualitative data, the Chi-square test was utilized and for quantitative data, the unpaired student t-test was applied. P values lower than 0.05 were regarded as significant.
Results
The mean age of both groups was similar. Males were predominant. The difference in age, gender, and residence was not statistically significant (p>0.05) between the two groups (Table 1).
| Demographic Characteristics | Asthmatic Children (n=60) | Non-Asthmatic Child (n=30) | P value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age (Mean±SD) | 11.32±2.007 | 11.07±1.938 | a0.579ns | ||
| Range (min-max) | 8.0-18.0 | 8.0-17.0 | |||
| Sex | |||||
| Male | 43 | 72 | 19 | 63 | b0.421ns |
| Female | 17 | 28 | 11 | 37 | |
| Residence | |||||
| Rural | 39 | 65 | 18 | 60 | b0.643ns |
| Urban | 21 | 35 | 12 | 40 |
Table 1: Demographic Characteristics of the Asthmatic and Non-Asthmatic Children (N=90).
ns= not significant aP value reached from unpaired t-test bP value reached from chi-square test Table 1: Demographic Characteristics of the Asthmatic and Non-Asthmatic Children (N=90).
| Types of Asthma | Number of Patients | Percentage |
|---|---|---|
| Intermittent | 16 | 26.70% |
| Mild persistent | 18 | 30.00% |
| Moderate persistent | 17 | 28.30% |
| Severe persistent | 9 | 15.00% |
Table 2: Types of Asthma in Asthmatic Children (n=60).
The majority (30.0%) of asthmatic children were suffering from mild persistent asthma and 28.3% had moderate persistent asthma, 26.7% had intermittent asthma. Only 15% had severe persistent asthma (Table 2).
| Asthmatic Children (n=60) | Non-Asthmatic Child (n=30) | P value | |
|---|---|---|---|
| (Mean ±SD) | (Mean ±SD) | ||
| Weight (kg) | 31.88± 6.54 | 31.72±6.65 | 0.910ns |
| Height (cm) | 134.9±14.5 | 136±14.8 | 0.618ns |
| BMI (kg/m2) | 17.4±1.7 | 17.1±1.6 | 0.360ns |
Table 3: Comparison of Weight, Height, and BMI among Asthmatic and Non-Asthmatic Children.
ns= not significant P-value reached from unpaired t-test Table 3: Comparison of Weight, Height, and BMI among Asthmatic and Non-Asthmatic Children.
The mean weight of asthmatic and non asthmatic children was 31.88±6.54 kg and 31.72±6.65 kg, respectively. The mean height of asthmatic and non-asthmatic children was 134.9±14.5 cm and 136±14.8 cm, respectively. The mean BMI of asthmatic and non-asthmatic were 17.4±1.7 kg/ m2 and 17.1±1.86 kg/m2, respectively. The children’s mean weight, height, and BMI were comparable, and there was no statistically significant difference (p>0.05) between the two groups (Table 3).
In the majority (53.3%) of the children with asthma, vitamin D level was insufficient (20-30 ng/ml). On the other hand, vitamin D level was sufficient (>30 ng/ml) in the majority (46.7%) of non-asthmatic children. The mean vitamin D level was found 24.7±7.1 ng/ml and 35.9±7.6 ng/ ml in asthmatic and non-asthmatic groups, respectively. The difference was statistically significant (p<0.05) between the two groups (Table 4).
| Vitamin D Level (ng/ml) | Asthmatic Children (n=60) | Non-Asthmatic Child (n=30) | P value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Deficiency (<20 ng/ml) | 14 | 23.3 | 4 | 13.3 | |
| Insufficient (20-<30 ng/ml) | 32 | 53.3 | 12 | 40 | |
| Sufficient (30-100 ng/ml) | 14 | 23.3 | 14 | 46.7 | |
| Mean±SD | 24.7±7.1 | 35.9±7.6 | 0.000s | ||
| Range (min-max) | 13.3-43.2 | 23.0-54.1 |
Table 4: Comparison of Serum Vitamin D level between Asthmatic and Non-Asthmatic Children (N=90).
s= significant P-value reached from unpaired t-test Table 4: Comparison of Serum Vitamin D level between Asthmatic and Non-Asthmatic Children (N=90).
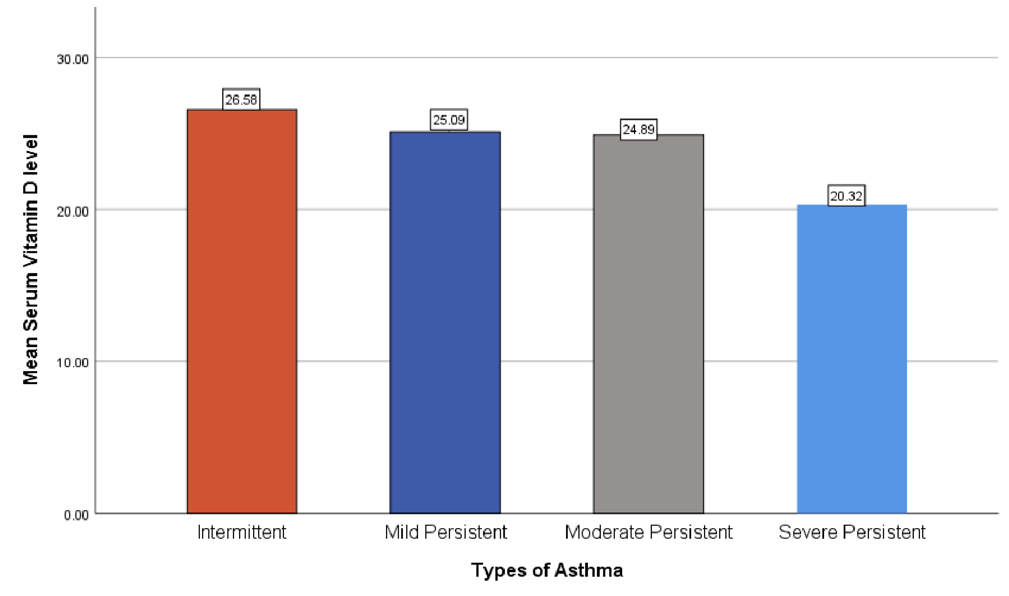
The mean serum vitamin D level was 20.32 ± 6.19 ng/ ml in severe persistent asthma. In other types of asthma, the mean serum vitamin D level was 25.46 ± 6.71 ng/ml which was not statistically significant (P=0.390) (Figure 1).
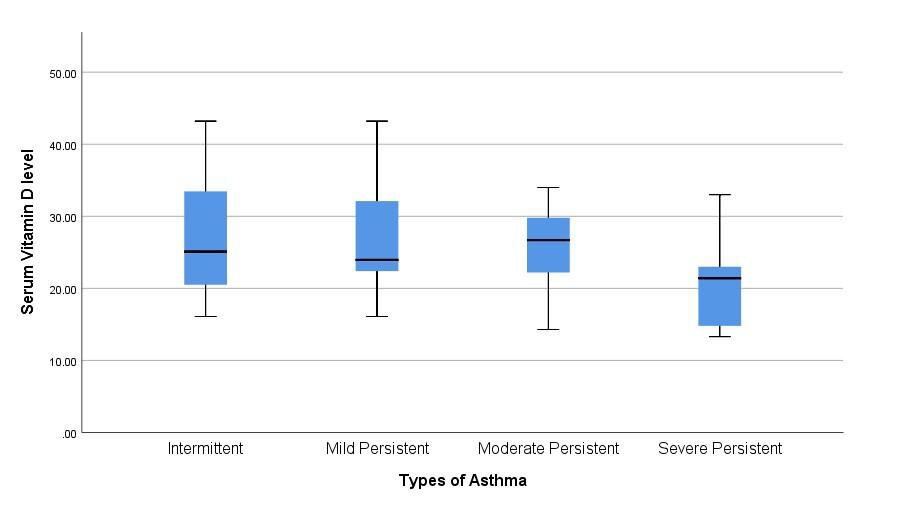
The minimum value of serum vitamin D level was 13 ng/ ml and the maximum value was 43 ng/ml among asthmatic children. The median value of serum vitamin D lies between 20-30 ng/ ml in each clinical type of asthma (Figure 2).
Different types of asthma are not affected by serum vitamin D levels. The chi-square test was not statistically significant (Table 5).
| Types of asthma | Category of Vitamin D | P value | |||||
|---|---|---|---|---|---|---|---|
| Deficiency (n=15) | Insufficient (n=35) | Sufficient (n=10) | |||||
| n | % | n | % | n | % | ||
| Intermittent | 4 | 26.7 | 8 | 22.9 | 4 | 40 | |
| Mild persistent | 4 | 26.7 | 12 | 34.3 | 2 | 20 | |
| Moderate persistent | 3 | 20 | 11 | 31.4 | 3 | 30 | 0.671 |
| Severe persistent | 4 | 26.7 | 4 | 11.4 | 1 | 10 |
Table 5: Comparison of Serum Vitamin D in Different Clinical Types of Asthma among Asthmatic Children (n=60).
s= significant P-value reached from chi-square test Table 5: Comparison of Serum Vitamin D in Different Clinical Types of Asthma among Asthmatic Children (n=60).
Discussion
In children, bronchial asthma is a prevalent respiratory disorder. Vitamin D is a fat-soluble nutrient and steroid hormone with traditional functions such as enhancing calcium absorption and preserving bone health. Recent research has shown that cardiovascular disease, inflammation, infectious diseases, multiple sclerosis, impaired physical functioning, and allergic diseases are inversely related to vitamin D concentration [31, 32].
Epidemiologic data in most of the reported studies suggest that low vitamin D levels (defined as serum 25- OH vitamin D level <20ng/ml) in children with asthma are associated with more symptoms, exacerbations, decreased lung function, increased medication use, and severe disease [33]. This study was intended to know the serum vitamin D level in asthmatic children and the association between serum vitamin D levels with different clinical types of asthma. This study showed that the difference in age, gender, and residence between asthmatic and non-asthmatic children was not statistically significant (p>0.05). A similar observation was found by many other studies [34, 35, 36].
In this study, the mean weight of asthmatic and non- asthmatic was 31.88± 6.54 kg and 31.72±6.65 kg, respectively. The mean height of asthmatic and non-asthmatic was 134.9±14.5 cm and 136±14.8 cm, respectively. The analysis of mean BMI asthmatic and nonasthmatic were 17.4±1.7 kg/ m2 and 17.1±1.86 kg/m2, respectively. The children’s mean weight, height, and BMI were comparable, and there was no statistically significant difference (p>0.05) between the two groups. A renowned study found the mean BMI was 16.1±2.0 kg/m2 in the asthma group and 16.1±1.5 kg/m2 in the without asthma group. The difference was not statistically significant (p>0.05) between the two groups [34]. A study observed that the mean BMI was found 16.93±2.60 kg/m2 in the without asthma group and 17.36±3.93 kg/m2 in the asthma group. The difference was not statistically significant (p>0.05) between the two groups [35]. In another study, they also observed no significant difference in height, weight, and BMI among asthmatic and non-asthmatic children [37], which is similar to the current study.
In this study, 73.3% of patients were vitamin D deficient/insufficient (21% were deficient with vitamin D levels <20 ng/ml and 52.2% were in the insufficient range with levels between 2030 ng/ml) which is similar to the prevalence of vitamin D deficiency in the general population [38]. Prevalence of vitamin D deficiency in a study done in Thailand reported that 64% were vitamin D deficient/ insufficient, which is similar to the present study [39].
This study showed 13.3% deficiency and 40% insufficiency of serum vitamin D among nonasthmatic children, almost similar to a study held in Turkey [40]. High prevalence rates of vitamin D deficiency/insufficiency are reported in otherwise healthy infants, children, and adolescents from diverse countries around the world, including Southeast Asia [41, 42, 43]. This may be due to behavioural factors, such as decreased time spent outdoors and lower vitamin D intake in the diet, use of sunscreen, and intrinsic factors such as skin melanin content and decreased cutaneous destruction of vitamin D3 [44].
The current study showed that 23.3% were deficient, and 53.3% had insufficient serum vitamin D among asthmatic children. A Turkish study reported 29.4% deficiency and 67.0% insufficient among children with asthma. The mean serum vitamin D level was found
24.7±7.1 ng/ml and 35.9±7.6 ng/ml in asthmatic and non-asthmatic children. The difference was statistically significant (p<0.05) between the two groups [40]. The mean (SD) serum vitamin D level in this study was similar to the study held in Thailand and in Iran [39, 45]. The mean serum vitamin D level of the children with asthma was marginally but significantly lower than their age and sex- matched counterparts without asthma. This is similar to reports of other previous studies [34, 35, 36, 40, 45]. These lower values could be thought to be due to less outdoor time and exposure to sunlight to prevent exposure to allergens with consequent lower vitamin D production, or poor intake of vitamin D-rich feeds because of fear of allergies. Children with asthma may utilize more vitamin D because of its immunoregulatory and anti-inflammatory effects in the immune system leading to lower serum levels. This cross-sectional study does not explain the reason for the lower mean serum vitamin D levels in asthmatic children Population-based longitudinal studies will be needed to ascertain the cause and effect of these lower serum vitamin D levels on childhood asthma.
This study found no significant difference between the concentration of vitamin D in the serum and the clinical types of asthma. This is similar to a study that demonstrated no relationship between the severity of childhood asthma and serum vitamin D levels [45]. This contemplates that Vitamin D deficiency may be associated with an increased incidence of childhood asthma, but its precise role in the severity of asthma is still obscure. Another study concluded that Vitamin D deficiency was not associated with asthma control in Indian children [46, 47]. Many studies also supported current study findings [34, 39, 45, 48].
However, a study reported correlations between serum vitamin D levels and asthma severity, control, and frequency of exacerbations [40]. This disparity may be because most of the children in this present study had mild diseases. The lack of association between vitamin D and different clinical types of asthma in this study signifies that vitamin D most probably plays a role in the case of its insufficiency or deficiency. This may imply that vitamin D supplementation may not be expected to benefit children with asthma who have normal serum vitamin D concentrations.
Conclusion
Serum vitamin D level were significantly lower among children with asthma shen compaired to their age and sex matched control. Different clinical categories of asthma were not affected by serum vitamin D levels.
- Limitations
- Small sampled, single center study.
- Here dietary intake of vitamin D was not assessed.
- Serum vitamin D was tested once due to lack of financial aid.
Acknowledgements: none
Declarations
Funding: done by Bangabandhu Sheikh Mujib Medical University.
Conflict of Interest: There was no conflict of interest.
Ethical Approval: done by the institutional review board of Bangabandhu Sheikh Mujib Medical University.
References
-
Hall SC, Fischer KD, Agrawal DK (2016) The impact of vitamin D on asthmatic human airway smooth muscle. Expert Review of Respiratory Medicine 10(2): 127-135.
-
World Health Organization (2020) Asthma.
-
Pal R, Dahal S, Pal S (2009) Prevalence of bronchial asthma in Indian children. Indian Journal of Community Medicine 34(4): 310-316.
-
Hassan MR, Kabir AR, Mahmud AM, Rahman F, Hossain MA, et al. (2005) Prevalence of asthma in highly polluted Dhaka city and low polluted coastal area of Bangladesh. Indian Journal of Allergy Asthma and Immunology 19(2): 85-92.
-
Hossain SK, Islam MS, Rahman MM De S, Mahmud K (2016) Clinical and demographic profiles of patients diagnosed as cough variant asthma attended at tertiary referral hospital, Journal of National Institute of Neurosciences Bangladesh 2(1): 30-33.
-
Global Initiative for Asthma (2018) Global Strategy for Asthma Management and Prevention. GINA pp: 1-162.
-
National Institute of Diseases of the Chest and Hospital (2016) National guideline Asthma and COPD, 5th (Edn.). Asthma Association Bangladesh, National Asthma Centre, NIDCH, India.
-
Global Asthma Report (2018) Asthma affects 339 million people. New Zealand: Global Asthma Network.
-
Carr TF, Zeki AA, Kraft M (2018) Eosinophilic and noneosinophilic asthma. American Journal of Respiratory and critical care medicine 197(1): 22-37.
-
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, et al. (2011) Evaluation treatment and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism 96(7): 1911-1930.
-
Camargo CA Jr, Rifas-Shiman SL, Litonjua AA, Rich- Edwards JW, Weiss ST, et al. (2007) Maternal intake of vitamin D during pregnancy and risk of recurrent wheeze in children at 3 y of age. The American Journal of Clinical Nutrition 85(3): 788-795.
-
Devereux G, Litonjua AA, Turner SW, Craig LC, McNeill G, et al. (2007) Maternal vitamin D intake during pregnancy and early childhood wheezing. The American Journal of Clinical Nutrition 85(3): 853-859.
-
Kerley CP, Elnazir B, Faul J, Cormican L (2015) Vitamin D as adjunctive therapy in asthma. Part 1: A review of potential mechanisms. Pulmonary Pharmacology and Therapeutics 32: 60-74.
-
Searing DA, Leung DY (2010) Vitamin D in atopic dermatitis, asthma and allergic diseases. Immunology and allergy clinics of North America 30(3): 397-409.
-
Jolliffe DA, Kilpin K, MacLaughlin BD, Greiller CL, Hooper RL, et al. (2016) Prevalence, determinants and clinical correlates of vitamin D deficiency in adults with inhaled corticosteroid-treated asthma in London, UK. The Journal of steroid biochemistry and molecular biology 175: 88-96.
-
Barragan M, Good M, Kolls JK (2015) Regulation of dendritic cell function by vitamin D. Nutrients 7(9): 8127-8151.
-
Berraies A, Hamzaoui K, Hamzaoui A (2014) Link between vitamin D and airway remodeling. Journal of Asthma and Allergy 7: 23-30.
-
Yawn J, Lawrence LA, Carroll WW, Mulligan JK (2015) Vitamin D for the treatment of respiratory diseases: Is it the end or just the beginning? The Journal of steroid biochemistry and molecular biology 148: 326-337.
-
Bozzetto S, Carraro S, Giordano G, Boner A, Baraldi E (2012) Asthma, allergy and respiratory infections: The vitamin D hypothesis. Allergy 67(1): 10-17.
-
Gupta A, Bush A, Hawrylowicz C, Saglani S (2012) Vitamin D and asthma in children, Paediatric Respiratory Reviews 13(4): 236-243.
-
Thacher TD, Clarke BL (2011) Vitamin D insufficiency. Mayo Clinic Proceedings 86(1): 50-60.
-
Brehm JM, Celedón JC, Soto-Quiros ME, Avila L, Hunninghake GM, et al. (2009) Serum vitamin D levels and markers of severity of childhood asthma in Costa Rica. American Journal of Respiratory and Critical Care Medicine 179(9): 765-771.
-
Kerley CP, Elnazir B, Faul J, Cormican L (2015) Vitamin D as adjunctive therapy in asthma. part 2: A review of human studies, Pulmonary Pharmacology and Therapeutics 32: 75-92.
-
Konstantinopoulou S, Tapia IE (2017) Vitamin D and the lung. Paediatric respiratory reviews 24: 39-43.
-
Tizaoui K, Berraies A, Hamdi B, Kaabachi W, Hamzaoui K, et al. (2014) Association of vitamin D receptor gene polymorphisms with asthma risk: Systematic review and updated meta-analysis of case-control studies. Lung: a journal of Springer International 192(6): 955-965.
-
Mirzakhani H, Al-Garawi A, Weiss ST, Litonjua AA (2015) Vitamin D and the development of allergic disease: How important is it? Clinical and experimental allergy 45(1): 114-125.
-
Pichler J, Gerstmayr M, Szépfalusi Z, Urbanek R, Peterlik M, et al. (2002) 1 alpha,25(OH)2D3 inhibits not only Th1 but also Th2 differentiation in human cord blood T cells. Pediatric Research 52(1): 12-8.
-
Benson AA, Toh JA, Vernon N, Jariwala SP (2012) The role of vitamin D in the immunopathogenesis of allergic skin diseases. Allergy 67(3): 296-301.
-
Bozzetto S, Carraro S, Giordano G, Boner A, Baraldi E (2012) Asthma, allergy, and respiratory infections: the vitamin D hypothesis. Allergy 67(1): 10-17.
-
Martineau AR, Jolliffe DA, Hooper RL, Greenberg L, Aloia JF, et al. (2017) Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and metaanalysis of individual participant data. BMJ pp: 357.
-
Brown SD, Calvert HH, Fitzpatrick AM (2012) Vitamin D and asthma. Dermato-Endocrinology 4(2): 137-145.
-
Sintzel MB, Rametta M, Reder AT (2018). Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurology and Therapy 7(1): 59-85.
-
Kunisaki KM, Niewoehner DE, Connett JE (2012) Vitamin D levels and risk of acute exacerbations of chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 185(3): 286-290.
-
Omole KO, Kuti BP, Oyelami OA, Adegbola AJ, Omole JO (2018) Serum vitamin D profile of Nigerian children with asthma: Association with asthma severity and control. The Journal of Pediatric Pulmonology 53(5): 544-551.
-
Somashekar, Ashwini BP, Nitha G (2014) Vitamin D Levels In Children with Bronchial Asthma. Journal of Clinical and Diagnostic Research 8(10): 04-07.
-
Esfandiar N, Alaei F, Fallah S, Babaie D, Sedghi N (2016) Vitamin D deficiency and its impact on asthma severity in asthmatic children. Italian journal of pediatrics 42(1): 108-112.
-
Fahad A, Yusra I, Mohammed AHI, Sara K (2019) Vitamin D levels in pediatric asthma: a comparative study. International Journal of Contemporary Medicine Surgery and Radiology 4(2): B31-B35.
-
Kumar J, Muntner P, Kaskel FJ, Hailpern SM, Melamed ML (2009) Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001-2004. Journal of Pediatrics 124(3): 362-370.
-
Krobtrakulchai W, Praikanahok J, Visitsunthorn N, Vichyanond P, Manonukul K, et al. (2013) The effect of vitamin d status on pediatric asthma at a university hospital, Thailand. Allergy, asthma & immunology research 5(5): 289-294.
-
Uysalol M, Levent CM, Gamze VS, Erkut K, Savas G, et al. (2013) Childhood asthma and vitamin D deficiency in Turkey: is there a cause-and-effect relationship between them?. Italian Journal of Pediatrics 39(1): 72-78.
-
Holick MF (2008) The vitamin D deficiency pandemic and consequences for nonskeletal health: mechanisms of action. Molecular Aspects of Medicine 29(6): 361-368.
-
Huh SY, Gordonm CM (2008) Vitamin D deficiency in children and adolescents: Epidemiology impact and treatment. Reviews in Endocrine and Metabolic Disorders 9(2): 161-170.
-
Marwaha RK, Tandon N, Agrawal N, Puri S, Agrawa lR, et al. (2010) Impact of two regimens of vitamin D supplementation on calcium vitamin D PTH axis of schoolgirls of Delhi. Indian Pediatrics 47(9): 761-769.
-
Heaney RP, Davies KM, Chen TC, Holick MF, Barger-Lux MJ (2003) Human serum 25hydroxycholecalciferol response to extended oral dosing with cholecalciferol. American Journal of clinical nutrition 77(1): 204-210.
-
Sharif A, Haddad Kashani H, Sharif MR (2020) Association of 25-hydroxy vitamin D with asthma and its severity in children: a case-control study. Clin Mol Allergy 18: 7.
-
Khan MH., Stanbrook MB, Anju A, Matthew B (2018) Vitamin D supplementation to prevent asthma exacerbations. The Lancet Respiratory medicine 6(6): 25-28.
-
Kavitha TK, Gupta N, Kabra SK, Lodha R (2017) Association of serum Vitamin D level of childhood Asthma. Indian Pediatrics 54(1): 29-32.
-
Harsh P, Barun KC, Isha M (2018) Association between serum vitamin D levels and allergic markers with childhood asthma. International Journal of Current Advanced Research 7(4): 1161711619.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet