Update on Pathology of Immune Checkpoint-Induced Liver Injury
Immunotherapy-associated liver injury (IALI) is a significant clinical concern that poses diagnostic and management challenges in patients treated with immune checkpoint inhibitors (ICIs). As the use of ICIs expands across various cancer types, it becomes increasingly important for healthcare professionals, researchers, and medical students specializing in oncology and immunotherapy to understand the pathological features of IALI. This understanding is crucial in effectively diagnosing and managing this condition. IALI typically presents as lobular hepatitis characterized by a mixed inflammatory infiltrate consisting predominantly of T lymphocytes, which often correlates with the clinical severity of liver damage. The inflammatory process may lead to hepatocyte necrosis, cholestasis, and sometimes bridging fibrosis, suggesting an autoimmune-like hepatitis. Notably, granulomatous inflammation has also been observed. This mini-review highlights the recent insights into the histopathological manifestations, mechanisms, and differential diagnosis of IALI, providing you with the knowledge and tools to address this clinical concern.
Abbreviations
DILI: Drug-Induced Liver Injury; PBC: Primary Biliary Cholangitis; PSC: Primary Sclerosing Cholangitis; AIH: Autoimmune Hepatitis; NSCLC: Non-Small Cell Lung Cancer; IRAES: Immune-Related Adverse Events; ICIs: Immune Checkpoint Inhibitors; IALI: Immunotherapy-Associated Liver Injury.
Introduction
Immune checkpoint inhibitors (ICIs) have changed cancer treatment, offering new hope to patients with various malignancies. These agents, including anti-CTLA-4, anti-PD-1, and anti-PD-L1 antibodies, work by exploiting the immune system to attack cancer cells. However, this enhanced immune activity can also result in immune- related adverse events (irAEs), including liver injury [1, 2]. Understanding the pathology of ICI-induced liver injury is essential for improving patient outcomes and developing effective management strategies.
Pathophysiology of ICI-Induced Liver Injury
The liver injury caused by ICIs is primarily immune- mediated. ICIs block inhibitory pathways like CTLA-4 and PD-1/PD-L1, leading to an unchecked immune response. This can result in the activation of T cells, which may target not only tumor cells but also normal hepatocytes. The liver, being rich in immune cells, becomes a site of immune- mediated inflammation and injury. The exact mechanisms are complex and involve various immune cells, including CD8+ T cells, natural killer cells, and macrophages, as well as cytokines like IFN-γ and TNF-α (2).
Risk Factors Associated with ICI-induced Liver injury
Immune checkpoint inhibitors have significantly advanced cancer treatment but come with the risk of immune-related adverse events, such as liver injury. The likelihood of ICI-induced liver injury is influenced by various patient factors, such as age, gender, and the type of tumor being treated. Older patients are at a heightened risk due to age-related changes in liver function and immune response, which can increase susceptibility to liver damage. Gender differences also play a role, with some studies indicating that males may have a higher incidence of liver injury, while in some other studies, females have been more susceptible. Also noted, patients of Asian ethnicity had a higher risk [3]. However, all this can vary depending on the type of ICI and cancer. The type of cancer is another crucial determinant; patients with melanoma, non-small cell lung cancer (NSCLC), and renal cell carcinoma, who frequently receive ICIs, are at a greater risk of developing liver injury. Additionally, the use of combination ICI therapies, particularly those that target both PD-1 and CTLA-4, is linked to a higher risk of hepatotoxicity compared to single-agent treatment. Pre-existing liver conditions, such as hepatitis or fatty liver disease and others, further amplify this risk. Identifying and understanding these risk factors is vital for clinicians to effectively monitor and manage liver toxicities in patients undergoing ICI therapy, ultimately improving patient outcomes [4].
Histopathological Patterns of Liver Injury
The histopathological patterns observed in ICI- induced liver injury are varied and can mimic other forms of liver disease, complicating diagnosis. However, several characteristic findings have been identified [5, 6, 7, 8].
Lobular Hepatitis: Lobular hepatitis is one of the most common histopathological findings in ICI-induced liver injury. It is characterized by inflammation and hepatocyte necrosis predominantly within the liver lobules. The infiltrate is typically mixed, comprising lymphocytes, histiocytes, and occasional eosinophils. The degree of necrosis can vary, with some cases showing mild spotty necrosis while others may exhibit more extensive confluent necrosis. Kupffer cell hypertrophy and activation are often observed, indicating an ongoing inflammatory process.
Portal Inflammation: Portal inflammation is another frequently observed feature. The portal tracts may show a mixed inflammatory infiltrate, including lymphocytes, plasma cells, and eosinophils. This pattern can resemble autoimmune hepatitis (AIH), making it crucial to distinguish between the two conditions. Plasma cells in the portal tracts is particularly suggestive of an immune-mediated process, but it is not exclusive to ICI-induced liver injury.
Granulomatous Hepatitis: Granulomas are occasionally found in the liver biopsies of patients with ICI-induced injury. These granulomas are typically non-caseating and can be associated with mild portal and lobular inflammation. The formation of granulomas suggests a delayed-type hypersensitivity reaction, which may be triggered by immune activation against hepatic antigens. While granulomatous hepatitis is not specific to ICI therapy, its presence should prompt consideration of this etiology in the appropriate clinical context.
Bile Duct Injury: Bile duct injury, though less common, has been reported in some cases of ICI-induced liver injury. This can manifest as cholangitis with bile duct inflammation or as bile duct paucity in more severe cases. The bile ducts may show epithelial damage, and there may be associated ductular reaction or periportal fibrosis. These findings overlap with those seen in primary biliary cholangitis (PBC) or primary sclerosing cholangitis (PSC), necessitating careful interpretation.
Vascular Changes: Vascular involvement in ICI-induced liver injury is uncommon but can occur. This may include sinusoidal dilatation, endothelialitis, or even hepatic veno- occlusive disease in rare cases. These changes are typically subtle and may require special stains or electron microscopy for definitive identification.
Comparison with Autoimmune Hepatitis
Given the immune-mediated nature of ICI-induced liver injury, there is significant overlap with the histopathological features of autoimmune hepatitis (AIH). Both conditions can show portal lymphoplasmacytic infiltrates, interface hepatitis, and lobular hepatitis. However, certain features may help differentiate the two. For example, the presence of eosinophils and granulomas is more suggestive of ICI- induced injury, while the absence of features like rosetting of hepatocytes or increased IgG levels may argue against a diagnosis of AIH. Additionally, the clinical context, including the temporal relationship to ICI therapy, is crucial in making the correct diagnosis.
Diagnostic Challenges
Histopathological evaluation of ICI-induced liver injury presents several diagnostic challenges. The overlapping features with other liver diseases, such as AIH, drug- induced liver injury (DILI), and viral hepatitis, require a comprehensive approach to diagnosis. Clinical history, including exposure to ICIs, serological tests, and imaging studies, must be integrated with histological findings to arrive at a definitive diagnosis. In some cases, additional studies, such as immunohistochemistry or molecular testing, may be necessary to exclude other etiologies.
Management and Prognosis
The management of ICI-induced liver injury often involves corticosteroids, particularly in moderate to severe cases. Steroids help suppress the immune-mediated damage to the liver. In refractory cases, additional immunosuppressive agents such as mycophenolate mofetil or tacrolimus may be required. The prognosis varies; while many patients respond
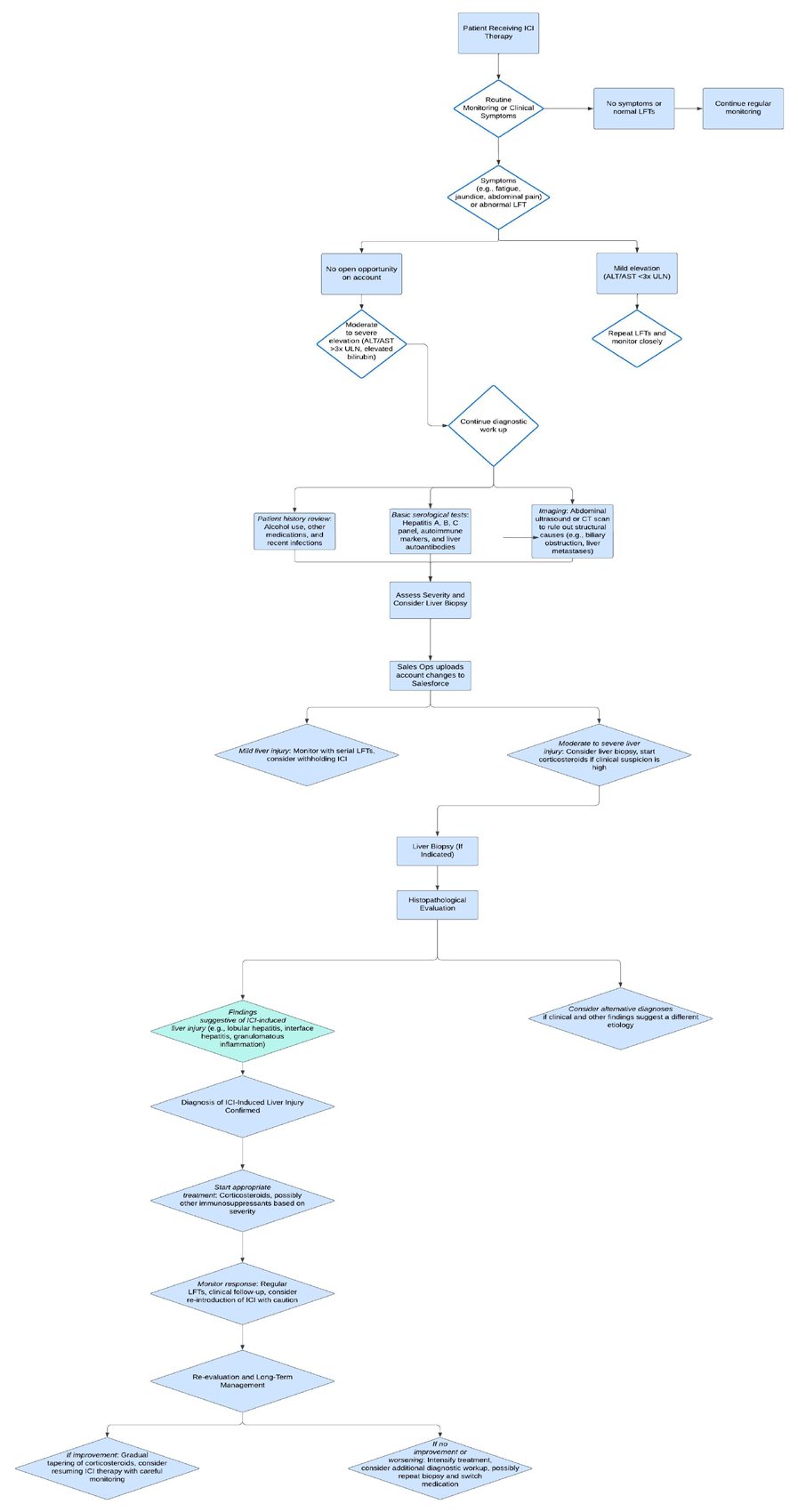
Flow Chart “Approach to ICI-induced Liver Injury”
well to treatment and can resume ICI therapy with careful monitoring, others may experience chronic liver damage or relapse upon rechallenge [9, 10, 11, 12].
Recent Advances and Future Directions
Recent studies have provided insight on the underlying mechanisms of ICI-induced liver injury, offering potential therapeutic targets. For instance, the role of specific immune checkpoints and cytokines in mediating liver injury is being actively explored. Additionally, research is ongoing to identify biomarkers that can predict susceptibility to liver injury, which would allow for personalized approaches to ICI therapy. The development of novel ICIs with a lower risk of irAEs is also a key area of interest.
Conclusion
Immune checkpoint inhibitors have transformed oncology but come with the risk of immune-related liver injury. Understanding the pathology of this condition is vital for improving diagnosis, management, and outcomes. Continued research is essential to unravel the complex mechanisms involved and to develop strategies that minimize liver injury while maintaining the efficacy of ICIs in cancer treatment.
This paper provides a comprehensive overview of the current understanding of the pathology of ICI-induced liver injury, including the mechanisms involved, histopathological features, clinical management, and recent research advances.
References
-
De Martin E, Jean-Marie M, Rosmorduc O, Guettier C, Samuel D (2020) Liver toxicity as a limiting factor to the increasing use of immune checkpoint inhibitors. JHEP Rep 2(6): 100170.
-
Taherian M, Chatterjee D, Wang H (2022) Immune Checkpoint Inhibitor-Induced Hepatic Injury: A Clinicopathologic Review. J Clin Transl Pathol 2(3): 83- 90.
-
Kawano M, Yano Y, Yamamoto A, Yasutomi E, Inoue Y, et al. (2024) Risk Factors for Immune Checkpoint Inhibitor-Induced Liver Injury and the Significance of Liver Biopsy. Diagnostics 14(8): 815.
-
Peters S, Wang H (2023) Risk factors and management of immune checkpoint inhibitor-induced liver injury. _Journal of Hepatology_ _78_(2): 321-332.
-
Zen Y, Yeh MM (2019) Checkpoint inhibitor-induced liver injury: a novel form of liver disease emerging in the era of cancer immunotherapy. Semin Diagn Pathol 36(6): 434-440.
-
Bhatia A, Kumar Y, Bhatia R (2020) Histopathology and liver injury: immune checkpoint inhibitors. Hepatology 71(5): 2121-2130.
-
Haanen J, Carbonnel F, Robert C, Kerr K, Peters S, et al. (2018) Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment, and follow-up. J Clin Oncol 30: 2691-2697.
-
Zen Y, Yeh MM (2021) Update on the histopathology of immune checkpoint inhibitor-related liver injury and current perspectives on management. Archives of Pathology & Laboratory Medicine 145(1): 80-89.
-
Peeraphatdit TB, Wang J, Odenwald MA, Hu S, Hart J, et al. (2020) Hepatotoxicity from immune checkpoint inhibitors: a systematic review and management recommendation. Hepatology 72(1): 315-329.
-
Doherty GJ, Duckworth AM, Davies SE (2017) Severe steroid-resistant immune checkpoint inhibitor- associated hepatitis successfully treated with mycophenolate mofetil. Journal of Hepatology 66(6): 1285-1287.
-
Remash D, Prince DS, McKenzie C, Strasser SI, Kao S, et al. (2021) Immune checkpoint inhibitor- induced hepatotoxicity: A systematic review. World J Gastroenterol 27(32): 5376-5391.
-
François-Xavier D, Anne-Laure V, Dyevre V, Jean-Marie M, Routier E, et al. (2018) Safety and efficacy of anti- programmed death 1 antibodies in patients with cancer and pre-existing autoimmune or inflammatory disease. Eur J Cancer 91: 21-29.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet