Compliance of Recommendations for Sessile Serrated Lesions with Dysplasia: Pathologist and GI Specialist Review
Sessile serrated lesion (SSL) with dysplasia is an accelerated phase toward invasive carcinoma, hence requiring closer followup in post-polypectomy surveillance plans. Conventional intestinal type dysplasia, such as tubular adenoma (TA), is one of the several forms of dysplasia seen in SSL, and it is recommended not to be graded. Likewise, calling such polyps ‘Mixed polyp with SSL and TA’ has been discouraged. To investigate the adherence of pathologists to new the terminology of SSL with dysplasia and how their reports may affect post-polypectomy surveillance by gastrointestinal specialists, we designed two separate surveys for both groups. Our survey showed that 69% of pathologists do grade SSL with dysplasia, and 61.5% still use the term ‘Mixed polyp with SSL and TA’. Responses from gastrointestinal specialists showed that 56% have different follow-up plans based on the grading of dysplasia in SSL, and 22% have different follow-up plans for SSL with dysplasia versus ‘Mixed polyp with SSL and TA’. Conclusions: The grading of dysplasia and the term ‘Mixed polyp with SSL and TA’ are still being used today, which affects postpolypectomy follow-ups.
Abbreviations
TSA: Traditional Serrated Adenoma; TA: Tubular Adenoma; SSL: Sessile Serrated Lesion.
Introduction
Traditional serrated adenoma (TSA) and SSL accounts for approximately 30% of colorectal carcinomas that develop via the serrated neoplasia pathway [1]. SSLs progress to carcinoma through epithelial dysplasia (SSLD) largely by MLH1 promoter methylation or, in a smaller subset, by p53 mutation or alterations in the WNT signalling pathway [2]. While SSLs show indolent growth before becoming dysplastic (> 10–15 years), SSLDs are considered to rapidly progress to either immunogenic microsatellite instable-high (MSI-H) (presumably 75% of cases) or mesenchymal microsatellite stable (MSS) colorectal carcinomas [3].
Dysplastic Changes in SSL can be Diagnosed by any of the Following Findings [2]
- Architectural changes such as crowding of crypts with complex branching and cribriforming.
- Cytological changes such as hypermucinous changes and conventional intestinal dysplasia (e.g. TA).
- Loss of MLH1 nuclear expression by immunohistochemistry.
“SSL with dysplasia” has replaced older terms such as “mixed polyp with SSL and TA”. In addition, the grading of dysplasia in SSL by pathologists has been discouraged, and it plays no role in post-polypectomy surveillance guidelines in many countries.
To investigate the compliance of surgical pathologists with these recommendations and how their reports may affect patients’ follow-up by gastroenterologists, we designed two separate surveys and emailed them to physicians.
Material and Method
A questionnaire was sent to Surgical Pathologists Signing GI Specimens with the Following Questions
- Do you grade dysplasia in SSL?
- If a polyp has both SSL and TA components, do you call it ‘Mixed polyp with SSL and TA’ or ‘SSA with dysplasia’?
- If SSL has any dysplasia, do you use this recommendation/ comment: “If complete endoscopic removal cannot be achieved, short-term re-endoscopy and biopsy, or surgical resection should be considered”.
Another Questionnaire was Sent to Gastrointestinal Specialists with the Following Questions
- Does the grading of dysplasia in SSL play a role in post- polypectomy follow-up?
- Do you have different follow-up plan for ‘‘Mixed polyp with SSL and TA’’ versus ‘‘SSL with dysplasia’’?
- Do you change your follow-up plan when you see the following pathologist’s recommendation/comment regarding SSL with dysplasia? “If complete endoscopic removal cannot be achieved, short-term re-endoscopy and biopsy, or surgical resection should be considered”.
Results
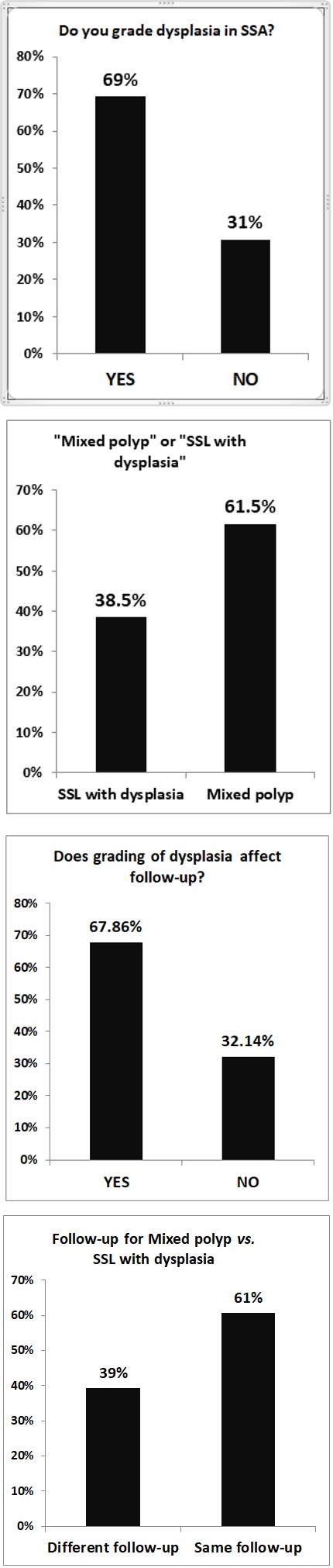
Sixty-five pathologists from North America and Asia completed the survey. Of those, 69% do grade dysplasia in SSL (Figure 1A), and 61.5% use the term ‘Mixed polyp with SSL and TA’ (Figure 1B). 64.6% of pathologists write no recommendation/comment to gastrointestinal specialists when SSL with dysplasia is present (data not shown).
Twenty-eight gastrointestinal specialists from North America, Europe, Asia, and Australia completed the survey. Of these, 67.86% have different follow-up plans based on the grading of dysplasia in SSL (Figure 2A) by giving priority to patients having SSL with high grade dysplasia. Thirty nine percent of gastrointestinal specialists said that they have different follow-up plans for SSL with dysplasia versus ‘Mixed polyp with SSL and TA’ (Figure 2B) by giving priority to patients having SSL with dysplasia. 39.28% of gastrointestinal specialists said that they change their follow- up plan based on the recommendation/comment from the pathologist regarding SSL with dysplasia (data not shown).
Discussion
The 5th edition of the World Health Organization’s Tumours of the Digestive System recommends the term ‘‘SSL with dysplasia.’’ The grading of dysplasia in SSL, i.e. low versus high grade, is not recommended, because of difficulty in grading, lack of reproducibility due to the heterogeneity of morphological changes, and the lack of correlation with loss of MLH1 expression [2].
Recommendations from an expert panel on serrated lesions [4] also discouraged grading conventional adenomatous dysplasia in SSL because the significance of the grading of dysplasia in SSL has not been evaluated. They recommend that SSL with any conventional cytological dysplasia be considered an “advanced” polyp with clinical significance similar to high-grade dysplasia in conventional adenomas. The lack of reproducibility in stratifying SSL into low-grade vs high-grade dysplasia is another reason to avoid grading dysplasia in SSL [5].
This Group Discouraged the Term “Mixed Hyperplastic/Adenomatous Polyp” for Two Reasons
- The term “Mixed polyp” does not convey the concept that the combined features represent the progression of an SSL towards carcinoma.
- Although the intestinal-type adenoma portion of SSL polyp has cytological similarities to conventional adenoma, it has molecular characteristics different from conventional adenomas.
Although the grading of dysplasia in SSL plays no role in post-polypectomy surveillance guidelines in North America and many other countries around the world, the grading of dysplasia in SSL as “low grade” or labeling such lesions as “Mixed polyp with SSL and TA” may convey the wrong message to gastrointestinal specialists. This could lead them to believe they are dealing with low-grade adenomas, in which there is no need for completeness of excision, and patients can be followed up over a longer period of time as a TA and/or SSL with no dysplasia. Our survey result from gastrointestinal specialists showed that these are indeed real possibilities.
For any SSL with dysplasia, it is strongly recommended to include a comment in the report to address the clinical significance of the diagnosis. As shown, 12.5% of gastroenterologists indicated that a comment from the pathologist affect the patient’s follow-up plan.
The Pathology Working Group on Classification of Benign Tumors in Ontario, Canada, Recommends a Comment Such as the Following
“Sessile serrated adenomas with dysplasia are considered to be advanced lesions that have an increased propensity to transform to adenocarcinoma. Complete endoscopic removal is recommended. If complete endoscopic removal cannot be achieved, short-term re-endoscopy and biopsy, or surgical resection should be considered” [6].
In conclusion, we believe that pathologists can significantly affect patients’ management by following the recommended guidelines in reporting SSL with dysplasia.
Figure 1A: Survey results from pathologists for Q1: Do you grade dysplasia in SSL?. Figure 1B: Survey Results from Pathologists for Q2: If a Polyp has both SSL and TA Components, do you call it ‘Mixed Polyp with SSL and TA’ or ‘SSA with Dysplasia’?.
Figure 2A: Survey Results from GI Specialists for Q1: Does the Grading of Dysplasia in SSL Play a Role in Post-Polypectomy Follow-Up?. Figure 2B: Survey Results from GI Specialists for Q2: Do you have Different Follow-Up Plan for ‘‘Mixed Polyp with SSL and TA’’ Versus ‘‘SSL with Dysplasia’’?.
Acknowledgement
We are very pleased with and thankful to the pathologists and gastrointestinal specialists who participated in our survey.
This paper was in part presented as a poster in CAP 18 meeting (College of American Pathologists Annual Meeting 2018), Chicago, IL, October 20-14, 2018 [7].
Conflict of Interest: This work was carried out with no conflict of interest.
References
-
Rosty C, Hewett DG, Brown IS, Leggett BA, Whitehall VLJ (2013) Serrated polyps of the large intestine: current understanding of diagnosis, pathogenesis, and clinical management. Journal of Gastroenterology 48(3): 287- 302.
-
IARC (2024) Classification of Tumours. Blue Books.
-
Utsumi T, Yamada Y, Diaz-Meco MT, Moscat J, Nakanishi Y (2023) Sessile serrated lesions with dysplasia: is it possible to nip them in the bud. J Gastroenterol 58(8): 705-717.
-
Rex DK, Ahnen DJ, Baron JA, Batts KP, Burke CP, et al. (2012) Serrated lesions of the colorectum: review and recommendations from an expert panel. Am J Gastroenterol 107(9): 1315-1329
-
Schaeffer D (2024) BC Cancer Colon Screening Program: Pathology Standards. BC Cancer.
-
(2011) Classification of Benign Polyps, Pathology Working Group Report. Capital Health Nova Scotia.
-
(2018) Abstracts and Case Studies From the College of American Pathologists 2018 Annual Meeting (CAP18). Arch Pathol Lab Med 142(9): e2-e202.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet