Isolated Collagen Disease of Gastroesophageal Junction (Collagenous GEJ Mucositis)
A 46 y/o male patient with diarrhea and symptoms mimicking gastroesophageal reflux disease (GERD) was admitted for Esophagogastroduodenoscopy and Colonoscopy. The microscopic examination of biopsies from gastroesophageal junction (GEJ) showed increased thickness of subepithelial collagen layer and other histomorphological characteristics similar to collagenous colitis; however, the gastric, duodenal and colonic biopsies were within normal limits. To our best knowledge, this is the first report on the isolated collagen disease of gastroesophageal junction (GEJ collagenous mucositis).
Abbreviations
GEJ: Gastroesophageal Junction; GERD: Gastroesophageal Reflux Disease; PPI: Proton Pump Inhibitor.
Introduction
Collagenous disease of GI tract including collagenous colitis, collagenous sprue of small intestine and collagenous gastritis have been well recognized [1]. However, isolated collagenous disease of gastroesophageal junction without involvement of stomach or an underlying disease such as eosinophilic esophagitis has not been reported. Herein, and for the first time, we report a case of isolated collagenous disease of GEJ (GEJ collagenous mucositis) without involvement of other parts of GI tract.
A 46-year-old man with long-standing symptoms of gastroesophageal reflux disease (GERD) and diarrhea was admitted to the endoscopy clinic. He had been followed for his irritable bowel syndrome for 4 years prior to this. He had no other significant health issue.
Upper endoscopy showed hiatus hernia, irregular Z line of the GEJ, and features suspicious for short segment Barrett’s esophagus. The colonoscopy was reported as unremarkable.
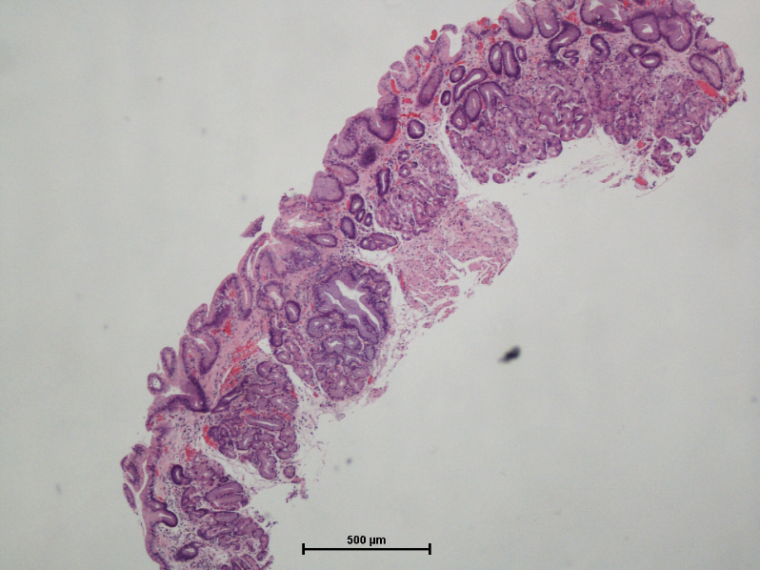
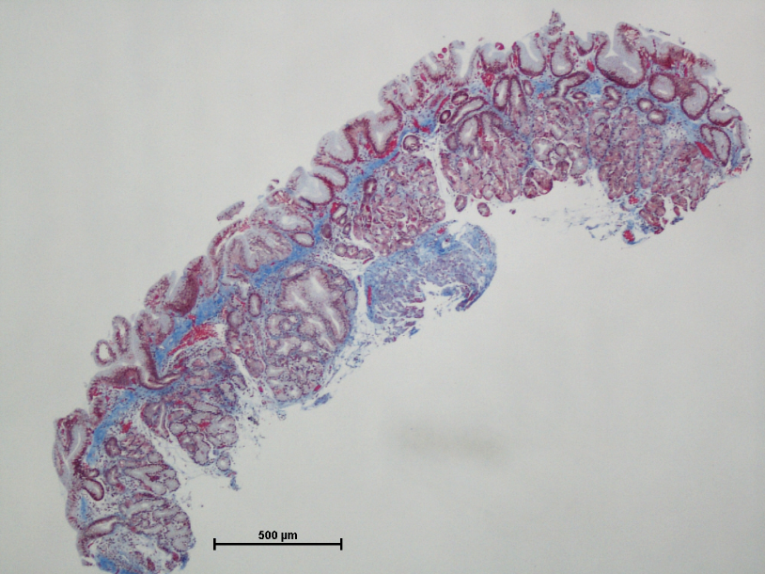
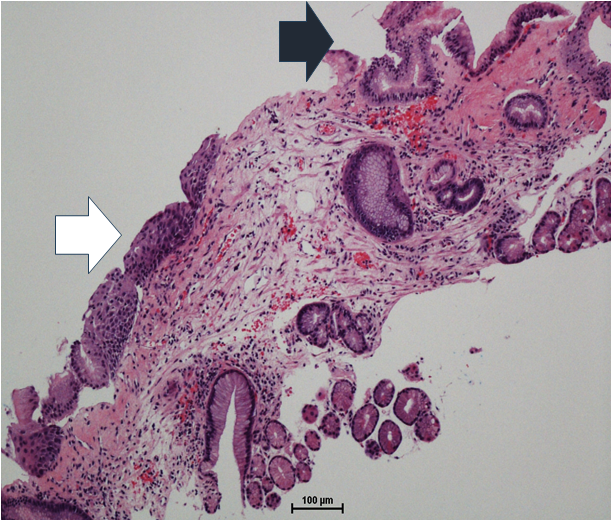
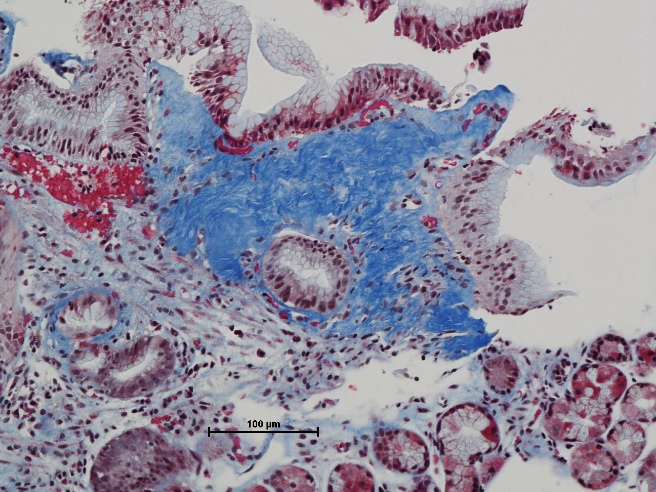
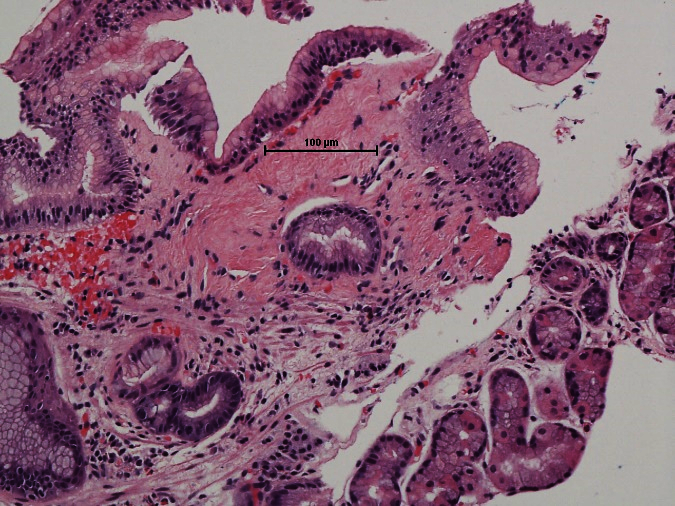
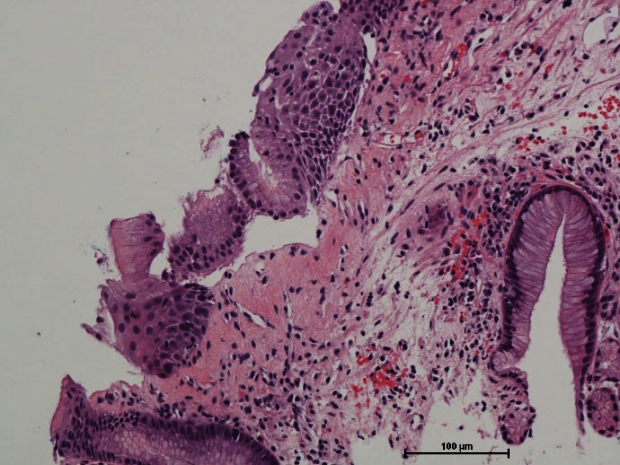
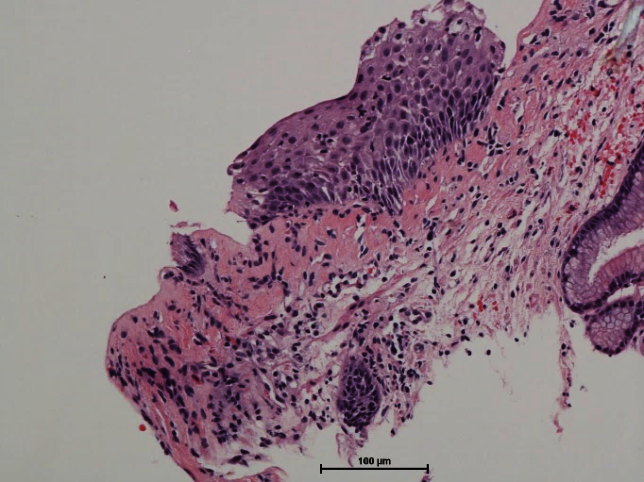
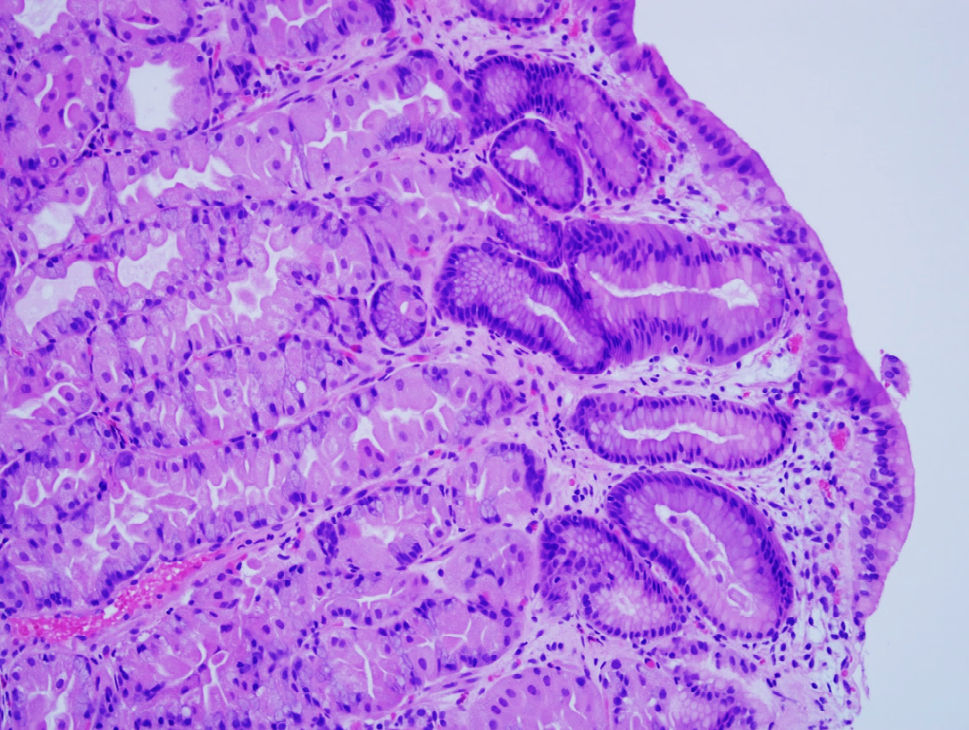
Histopathology assessment of the GEJ mucosal biopsies showed an increased thickness of the subepithelial collagen layer up to 100 uM, confirmed by trichrome stain (Figure 1). Thick collagen deposition involved both columnar and squamous epithelial components of GEJ (Figure 2). The collagen fibers focally extended into deeper lamina propria and surrounded glands/pits (Figure 3) and superficial blood vessels. Thick collagen layer was associated with focal detachment and denudation of squamous and columnar epithelial cells (Figure 4). These features are similar to histomorphology of collagenous colitis. In addition to these findings, the squamous epithelium showed mild intercellular
edema (spongiosis) and scattered rare lymphocytes, but no intraepithelial neutrophil or eosinophil. The lamina propria of GEJ showed mild lymphoplasmacytic inflammation. There was no histomorphology finding suggestive of scleroderma. There was no Goblet cell metaplasia to support the endoscopic findings of a short segment Barrett’s esophagus. Special stain (GMS) did not identify any yeast/fungus.
The gastric biopsies including corpus and antrum showed scattered lymphoplasmacytic inflammatory cells mainly in the antrum and proton pump inhibitor (PPI) effects in corpus mucosa (Figure 5). There was no
evidence of increased subepithelial collagen layer thickness, intraepithelial lymphocytosis, intestinal metaplasia, atrophy, endocrine hyperplasia or Helicobacter pylori infection in the gastric biopsies.
Multiple biopsies from duodenum, terminal ileum, right and left colon were within normal limits. Unfortunately, no information about patient’s follow-up is available due to change of institution.
Discussion
Collagenous colitis as the causes of diarrhea and malabsorption has an incidence of 2-10.8 per 100,000 per year [2]; however, collagenous sprue and collagenous gastritis are relatively considered as rare diseases.
Collagenous gastritis shows a bimodal distribution; 1- Children and young adults presenting with anemia, 2- Older adults presenting with diarrhea. Collagenous gastritis may be found in isolation (mainly in children and young adults), or in association with other diseases (in older adults) such as microscopic colitis, duodenal intraepithelial lymphocytosis, celiac disease, collagenous sprue, inflammatory bowel disease, autoimmune disorders [3, 4, 5] and some medications including immunotherapy drugs and Olmesartan [1]. The subepithelial collagen deposition in collagenous gastritis ranges between 15 to 115μM [6].
There is no report on isolated collagenous disease of GEJ (GEJ collagenous mucositis); however, there are two case reports of collagen deposition of GEJ associated with collagenous gastritis. In one paper, gastric biopsy showed sever chronic inflammation, patchy collagenous deposits, focal lymphocytic gastritis, severe mucosal atrophy, fibrosis and focal intestinal metaplasia. However, no detailed histomorphology description such as diameter of collagen layer or photomicrograph of GEJ was provided except this phrase: “an area of fibrosis under the luminal surface consistent with collagen deposits, which may be consistent with collagenous esophagitis” [7]. The second paper reported patchy thickened subepithelial collagen plate in the columnar component but not in squamous component of GEJ associated with collagenous gastritis [8]. This paper did not provide detailed histomorphology description of GEJ involvement such as diameter of collagen layer, neither.
Fibrosclerotic changes of lamina propria of GEJ has been reported in both eosinophilic esophagitis and reflux esophagitis; however, there was no histomorphology finding to suggest these entities in our patient [9, 10].
There is no established treatment for collagenous disease of GEJ (GEJ collagenous mucositis); however, proton pump inhibitors (PPI) were reported to be effective in resolution of the subepithelial collagen plate in the esophagus and gastric body [8]. Unfortunately, this was not an option for our patient because his gastric biopsies showed that he was on PPI.
Our case report is the first report of collagenous disease of GEJ (GEJ collagenous mucositis) without collagenous disease of stomach and intestines, celiac disease or other above-mentioned diseases commonly seen with collagenous gastritis [11].
Conclusion
Collagenous disease of GEJ (GEJ collagenous mucositis) may present with clinical symptoms of GE reflux (GERD) and diarrhea, either as an isolated disease or in association with collagenous gastritis. It is not uncommon to biopsy the epithelial lining of GEJ during endoscopy assessment; however, histopathology diagnosis of Collagenous disease of GEJ (GEJ collagenous mucositis) requires full thickness of squamocolumnar mucosa (both epithelial ling and lamina propria) of GEJ.
Acknowledgement
This work was in part published in CAP 19 [11].
Conflict of Interest
This work was carried out with no conflict of interest.
References
-
Longacre TA (2022) Mills and Sternberg’s Diagnostic Surgical Pathology. Wolters Kluwer Health 7: 3157.
-
Dietrich CF (2024) Microscopic (lymphocytic and collagenous) colitis: Clinical manifestations, diagnosis, and management. UpToDate.
-
Genta RM, Turner KO, Morgan CJ, Sonnenberg A (2021) Collagenous gastritis: Epidemiology and clinical associations. Dig Liver Dis 53(9): 1136-1140.
-
Srivastava A, Allende DS (2022) Gastrointestinal and Liver Pathology. In: Foundations in Diagnostic Pathology 3rd (Edn.), Goldblum JR (Ed.), Medicine, pp: 704.
-
Deb A, Songtanin B, Thongtan T, Islam S (2022) Collagenous gastritis presenting as chronic heartburn in a patient with psoriatic arthritis. Southwest Respir Crit Care Chron 10(45): 45.
-
Arnason T (2015) Collagenous gastritis: a morphologic and immunohistochemical study of 40 patients. Mod Pathol 28(4): 533-544.
-
Usta Y, Millstine D, Kenny F (2014) Collagenous gastritis: Gastroesophageal reflux disease in an adult patient without collagenous colitis. Int J Case Rep Images IJCRI 4(12): 678-681.
-
Tamai R, Simmons OL, Gong Y, Sheibani S, DeLeve L (2020) S1927 Collagenous Gastritis With Esophageal Involvement: An Unusual Cause of Dysphagia. Off J Am Coll Gastroenterol 115: S1002.
-
Mud HJ (1989) Healing of esophagitis and intraparietal esophageal collagen. In: Giuli R, McCallum RW (Eds.), Benign Lesions of the Esophagus and Cancer, Germany, pp: 574-576.
-
Haugen EJ, Locke AK, Correa H, Baba JS, Mahadevan- Jansen A, et al. (2024) Characterization of lamina propria remodeling in pediatric eosinophilic esophagitis using second harmonic generation microscopy. Transl Med Commun 9(1): 10.
-
(2024) Abstracts and Case Studies from the College of American Pathologists 2019 Annual Meeting (CAP19). Archives of Pathology & Laboratory Medicine 143 (9): e2–e226.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet