Updates on Vestibular Schwannoma Cellular Variant: Case Reports and Review of Literature
Background: Schwannoma is a benign, well-circumscribed tumor attached to peripheral nerves, consisting of a clonal population of Schwann cells. Cellular Schwannomas is a relatively uncommon but significant variant of Schwannoma, have a higher cellularity and mitotic rate than conventional Schwannomas. Case Reports: Case 1 presented in a 22 year female patient presented with headache, vertigo, facial numbness and loss of balance of one month duration. Past history, she was case of cerebellopontine angle tumor (Vestibular Schwanomma) operated for the same in two year back. MRI brain plain and contrast findings were, a well-defined lobulated extra axial mass lesion noted at left CP angle measuring 3.2x3.3x2.7cm. Patient treated with surgical excision of left cerebellopontine space occupying lesion. On histopathological examination reported as vestibular Schwannomas-cellular variant. Case 2 was a 55 year female patient presented with headache, ataxia, giddiness and dementia. MRI Brain showed a well- defined hypointense, heterogenously hyperintense solid-cystic extra-axial lesion in left cerebello-pontine cistern measuring 2.4 x 2.8 x 2.5 cm. Excision of left cerebellopontine space occupying lesion was done. On gross, irregular, grey-white, soft tissue mass lesion 2.5x2x0 cm. On histopatholical findings reported as vestibular schwannoma-cellular variant. Immunohistochemistry revealed S100, SOX10 positive and Ki-67 proliferation index is moderately elevated (3%). Conclusion: Cellular Schwannomas is an uncommon variant of Schwannoma. Local recurrence in cellular schwannoma may observe related to its high cellularity, increased mitotic activity, resection extent and tumor size. Herewith presenting this cases for its clinical, radio imaging, and histopathological findings.
Jagtap SV¹*, Jagtap SS², Dodia D³, Bandodkar N³, Patil P³ and Jadhav AS⁴
Abbreviations
CISS: Constructive Interference in Steady State; MPNST: Malignant peripheral Nerve Sheath Tumor; LINAC: Linear accelerator-based radiosurgery.
Introduction
Schwannoma is a benign peripheral nerve sheath tumor composed of Schwann cells. Vestibular Schwannoma arises from the vestibular branch of the vestibulocochlear VIII cranial nerve [1].
The epidemiology in the United States in 2004-2016 observed that the incidence of Vestibular Schwannoma at 20-44 year age is 0.75 per 100,000 cases [2]. The clinical presentation is usually as slowly progressive unilateral hearing loss. Cellular Schwannoma is composed of Antoni A patterns predominantly, lacking Verocay bodies. Although benign, it often displays local aggressiveness in the form of bony erosion. Increased cellularity, atypia, raised mitotic activity in cellular Schwannoma mimics malignant change. In this case cranial nerve VIII was involve with local recurrences. The degree of surgical resection and larger tumors were associated with the risk of recurrence and postoperative outcome [3].
Case Report
Case 1
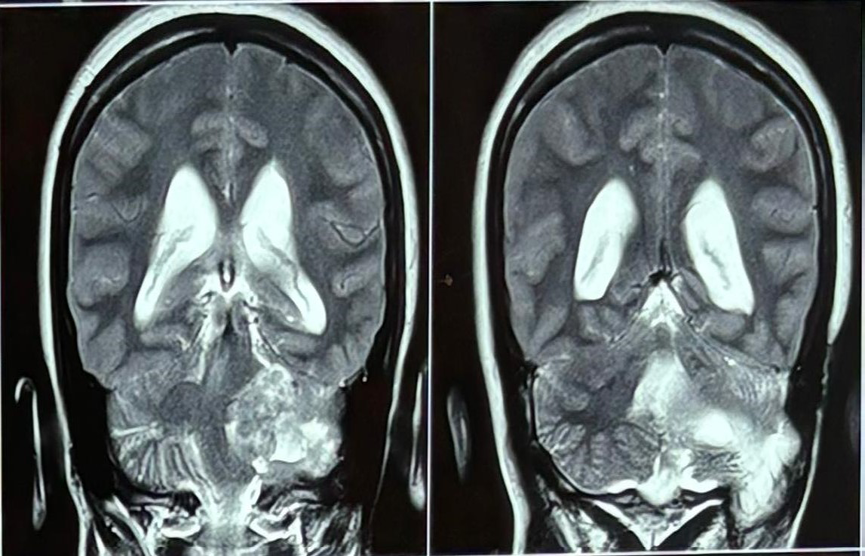
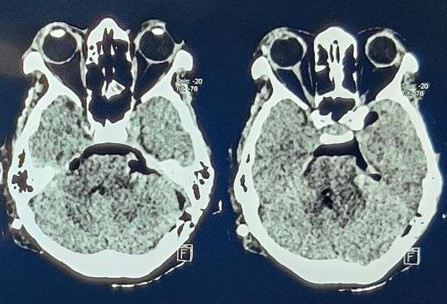
A 22 year female patient presented with headache, vertigo, facial numbness and loss of balance of one month duration. Patient was apparently alright 1 month back. She experienced headache which was moderate in severity without any aggregating or relieving factors of one month duration. Patient was also having vertigo while getting up from lying position. Patient experienced loss of balance while walking since last one month, also noted left facial numbness. No history of seizure, fever, diabetes, hypertention or any systemic disorders. Past history, she was case of cerebellopontine angle tumor (Vestibular schwanomma) operated for the same in two year back. Central nervous systems higher function were normal, other cranial nerves were normal and Pupil, Sensation, motor power were normal. Clinically suspected of left cerebellopontine angle space occupying lesion. Routine investigations were normal. MRI brain plain and contrast findings were, a well- defined lobulated extra axial mass lesion noted at left CP angle measuring 3.2x3.3x2.7 cm. Figure 1, showing signal characteristics as hypointense on T1W, heterogeneously hyperintense on T2W/FLAIR, shows heterogenous avid post contrast enhancement. Few focal areas of blooming noted on SWI (hemorrhages). Facial and vestibulocochlear nerves not seen separate from the lesion.
The lesion was extending medially and causing mass effect on adjacent left half of pons, posteriorly it was causing mass effect on middle cerebellar peduncle. No evidence of calcifications within the lesion.
Laterally the lesion is extending into left internal acoustic canal with its widening. Cranioplasty defect with soft tissue replacement noted in left occipital bone related to old postoperative changes. Impression given was supratentorial mass lesion with abnormal post contrast enhancement, in a previously operated case of left vestibular schwannoma, features suggestive of recurrent/residual lesion. There was no evidence of any other supratentorial mass lesion.
On Constructive Interference in Steady State (CISS) sequence showed the lesion which was not separately from left cranial nerve VII and VIlI complex and shows extension into the internal auditory canal. It was causing mass effect on the proximal portion of adjacent left trigeminal nerve and superior cerebellar artery. Rest of the cerebral hemispheres including white matter, bilateral thalami, basal ganglia appear normal in morphology and signal intensity.
Patient treated with surgical excision of left cerebellopontine space occupying lesion. The long-term follow-up is recommended in this case.
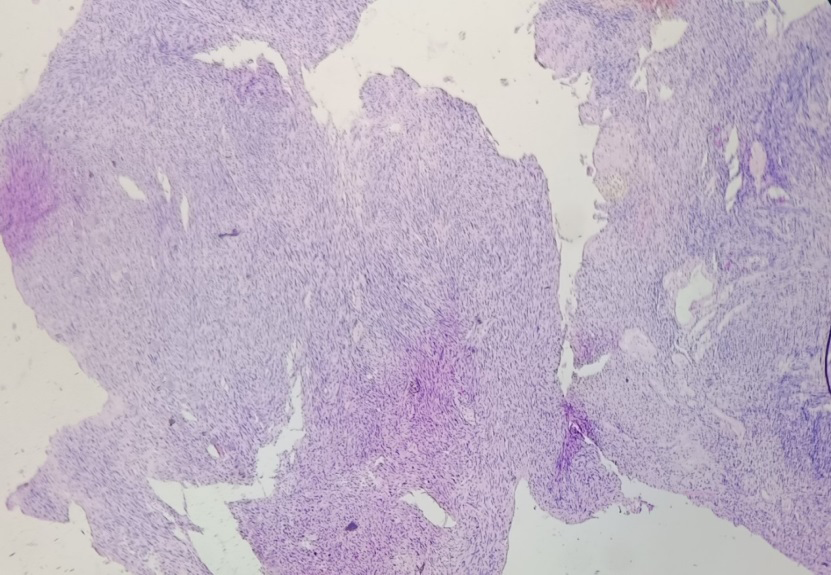
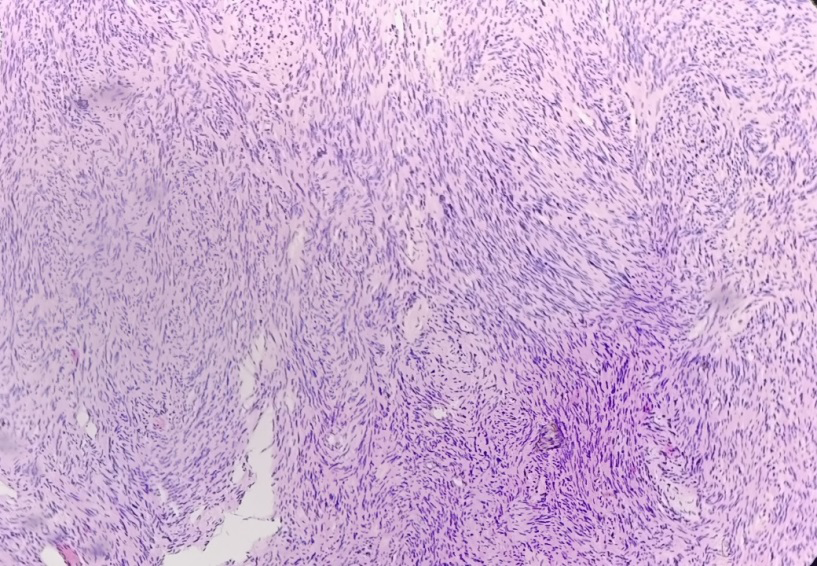
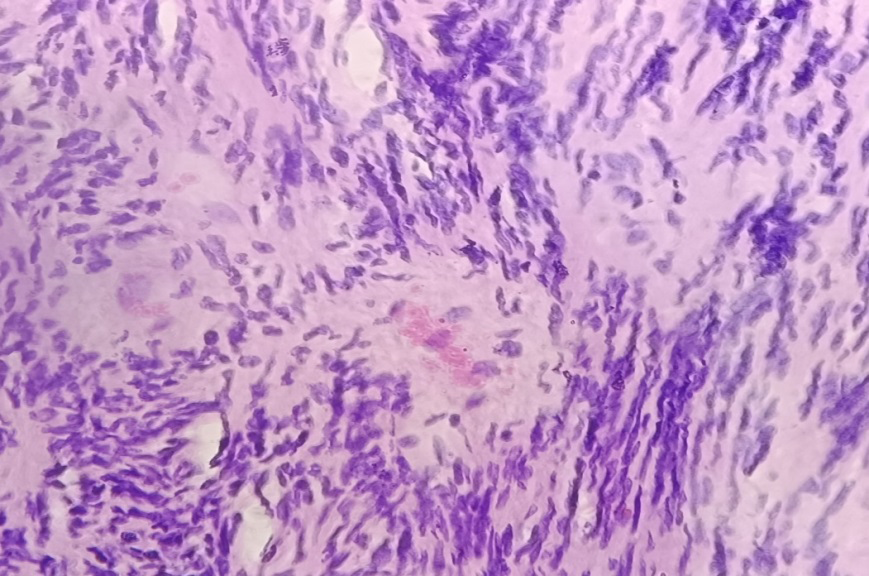
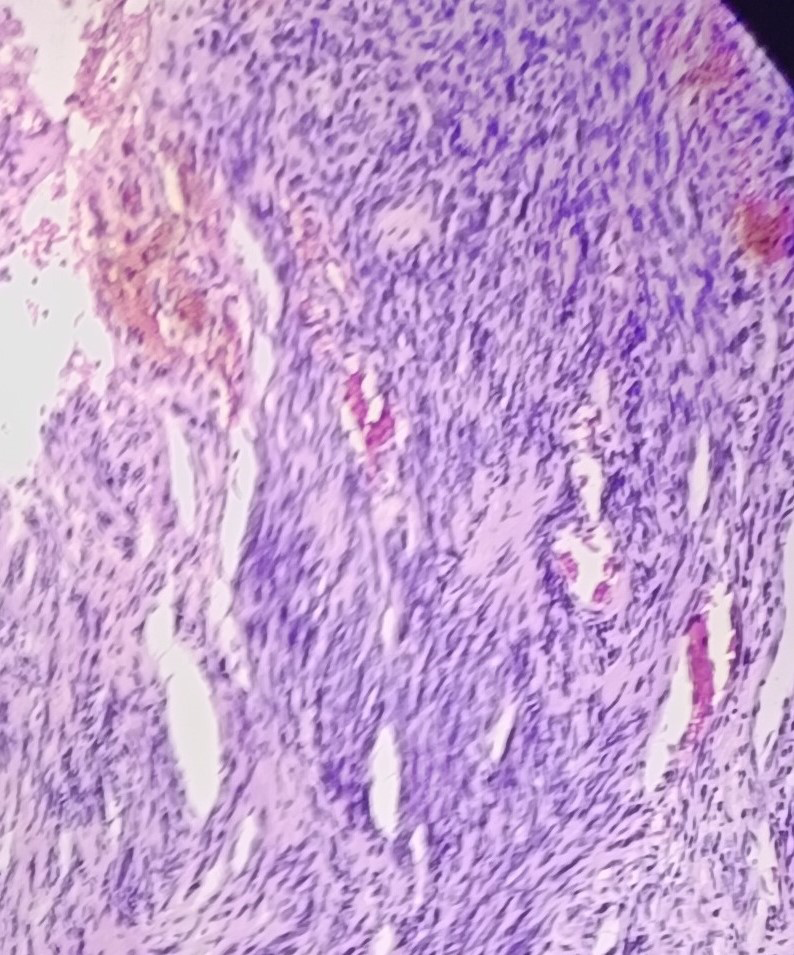
On gross we received (Figure 2), multiple, irregular, soft to firm, light tan-white-yellow -grey tissue. On histopathogical examination showed an encapsulated tumor composed of highly cellular, compact areas entirely of Antoni A tissue and devoid of Verocay bodies. A loose microcystic areas, hyalinized vessels, lipid laden macrophages, focal degenerative atypia was present. The tumor showed 4 mitoses per 10 high power fields, on histopathological findings reported as Vestibular Schwannomas-cellular variant (Figures 3-5).

Case 2
A 55 year female patient presented with headache, ataxia and loss of balance, giddiness of 7 days duration, and history of dementia six month, urinary incontinence 5 days. Also noted 2-3 episodes of involuntary movements, past history of head injury, frontal area five year back. No history of fever, diabetes, hypertention or any systemic disorders. Clinically suspected space occupying lesion. Routine investigations were normal. MRI Brain (Plain+Contrast) showed a well- defined altered signal intensity, T1WI- hypointense, T2WI/ FLAIR heterogenously hyperintense solid-cystic extra- axial lesion noted in left cerebello-pontine cistern (Figure 6) measuring 2.4 x 2.8 x2.5 cm and causing mass effect on adjacent cerebellar hemisphere and left half of medulla and middle cerebellar peduncle. Lesion was not separately seen from left CN VII and amp; VIII complex and shows minimal extension into the internal auditory canal for a length of (~ 7 mm). It is abutting the root entry zone of adjacent trigeminal nerve causing its mild lateral displacement and ventricular system (Lateral, 3rd and 4th ventricles): appear disproportionately prominent as compared to the sulcal spaces and basal cisterns with upward bowing and thinning of the corpus callosum. Imaging features suggestive of vestibular schwannoma.
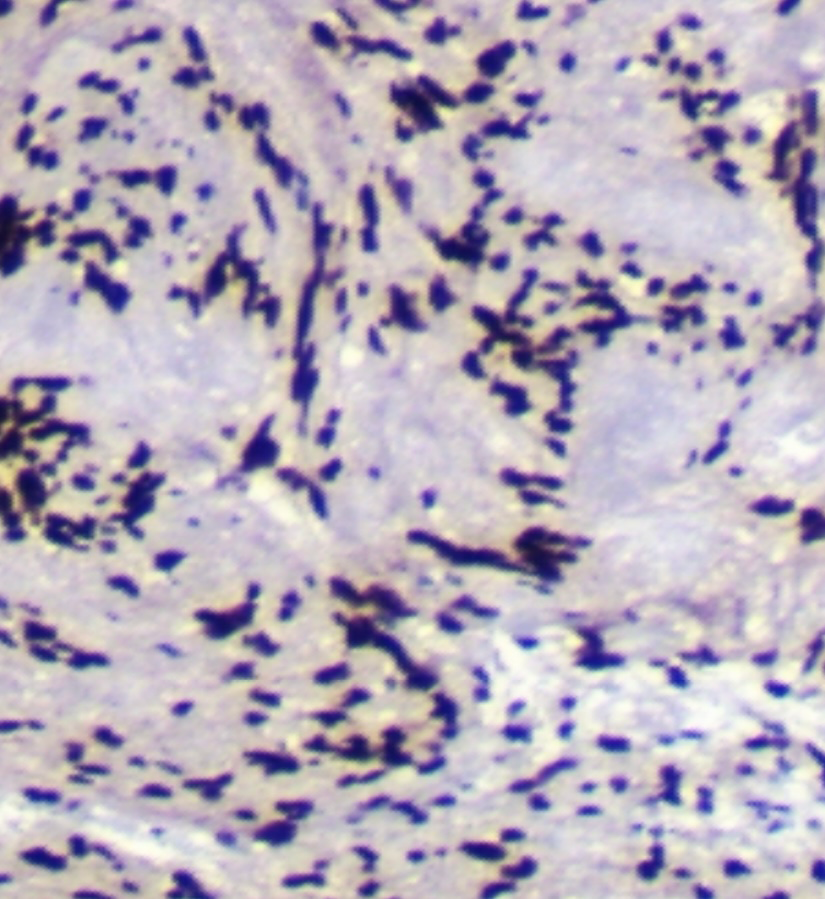
Excision of left cerebellopontine space occupying lesion was done. On gross, irregular, grey-white, soft tissue mass lesion 2.5x2x0.8 cm (Figure 7). On histopatholical findings reported as vestibular schwannoma-cellular variant left cerebello-pontine angle (Figure 8). Immunohistochemistry revealed S100, SOX10 positive (Figure 9) and Ki-67 proliferation index is moderately elevated (3%.) The long- term follow-up is recommended in this case.

Discussion
Schwannomas are benign, well-encapsulated, slow- growing nerve sheath tumors composed exclusively of Schwann cells derived from the neural creast. Most cases are sporadic; however, some are associated with NF2, schwannomatosis or Carney’s complex. Central lesions commonly arise from spinal nerve roots either intradural or extramedural. The common intracranial site is the vestibular branch of the eighth nerve, but they may also arises from other cranial nerves. Most of Schwannomas are solitary (90% of the cases) [4, 5].
If schwannoma has no relation to cranial nerves, they are considered intracerebral Schwannoma. The World Health Organization classifies Schwannoma as a grade I benign tumor. The Central Brain Tumor Registry of the United States shows that non−malignant nerve sheath tumors account for 8.6% of all central nervous system tumors reported [6]. The majority of Schwannomas are being located in the cerebellopontine angle (80–90%) [7]. About 60% of benign schwannomas are vestibular schwannomas.
The vestibular Schwannomas are mostly unilateral and occur sporadically. Rarely noted as bilateral tumor and usually associated with neurofibromatosis type 2. The incidence of bilateral vestibular Schwannomas is of 0.8 per 50,000 cases. Mostly women are affected with a common in age 30s to 60s, having the median age of patients is at 55 years. The incidence of vestibular Schwannomas in the USA is 1.2 cases per 100,000/year [8].
Radio Imaging Features
Radio imaging plays a central role in the screening and initial and follow-up assessment of vestibular Schwannomas. A MRI is the preferred technique which gives tumor characterization, surgical planning, and post therapeutic evaluation for tumor progress or any recurrence [9].
On radio imaging on MRI, these lesions are hypointense on T1-weighted images and iso or hyperintense in T2 weighted images. Well circumscribed masses that displace adjacent structures without direct invasion. The vestibular Schwannomas are located in the internal auditory canal, which give rise to wideing. Large tumors also extend into the cerebellopontine angle and cause the typical “ice cream cone” appearance.
For diagnosing and differentiating from neurofibromatosis and meningioma, T1-weighted imaging with gadolinium contrast remains the gold standard.
Histopathological Features
On gross examination shows encapsulation, with a smooth surface. On cut surfaces these are firm, light tan- white-yellow, rubbery to firm in consistency. The size is up to 5 cm, It may show cystic areas.
The histologic features shows a biphasic, encapsulated tumor composed of compact areas with spindle cells (Antoni A) and palisading nuclei (Verocay bodies) and loose microcystic areas with lipid laden macrophages (Antoni B), focal degenerative atypia may be present [10]. Other histologic findings in Schwannomas are hyalinized vessels with perivascular hemosiderin deposition. Four major forms of schwannoma are recognized. These include conventional, cellular, plexiform, and melanotic schwannoma.
Initially Woodruff JM, et al. [10] in 1981 described Cellular schwannoma. Cellular Schwannomas commonly occur in the spinal and paraspinal regions, and about 10% are intracranial locations. The tumors are composed predominantly of compact spindle cells, cellular Antoni A-type with variable hyperchromasia and pleomorphism, but without well-formed Verocay bodies. Most tumors have fewer than four mitoses per 10 high power fields, but in some cases the mitotic rate may be higher. Local recurrence and malignant transformation in cellular schwannoma may observe related to its high cellularity, increased mitotic activity, fascicular growth pattern, and occasional locally destructive character. Local recurrence varies and may be higher compared to classic Schwannomas.
Differential and Immunohistochemistry
The differentials for cellular Schwannomas are Meningioma, Neurofibroma, Malignant peripheral nerve sheath tumor (MPNST) [11, 12, 13]. MPNST are a relatively shows high cellularity, brisk mitotic activity, frequent necrosis, thick intersecting bundles, intravascular herniation, increased perivascular cellularity.
These are less sensitivities for S100 and SOX10 immunoreactivity. While cellular schwannomas shows the presence of Schwannian whorls, a peritumoral capsule, subcapsular lymphocytes, macrophage-rich infiltrates, absence of fascicles, low mitotic rate (most cases having < 4 mitosis/10hpf), perivascular hyalinization, and on immunohistochemistry uniform, diffuse S100 protein immunoreactivity [14].
Differential diagnosis can be challenging from the solitary fibrous tumor. These however show typical staghorn blood vessels, collagen fibers, and positive immunoreactivity for STAT6. Another differential is fibroblastic meningioma.
On immunohistochemistry Schwannomas typically shows tumor cells nuclear and cytoplasmic expression of S-100 as strong and diffuse positivity. Also SOX10 positive .While EMA, STAT6 and GFAP negative [15].
Treatment and Prognosis
In cases of small asymptomatic vestibular schwannomas can be managed conservatively. These cases requires MRI follow-up, to look for any recurrences. In patients with large and symptomatic lesions, management is complete surgical excision of tumor, which remains the most preferred treatment option. The overall prognosis is excellent.
In our case, patient showed recurrence. The reported rate of vestibular Schwannomas recurrence after total tumor removal is 0.5% and 9.2% [16]. The surgery or surgery followed by radiosurgery is an alternative to conventional surgical techniques. That the radiosurgery is a radiation therapy with the “gamma knife” or Linear accelerator-based radiosurgery (LINAC) may be used [17]. In cases adjuvant or neoadjuvant chemotherapy may be required.
The recurrence after total resection is very uncommon. Fabbris C, et al. [18] in meta-analysis study noted, the prognosis is depends on the symptoms size, location of the tumor, cellurarity, and association with neurofibromatosis type 2 [18]. Kano H, et al. noted that the hearing preservation after stereotactic radiosurgery can be achieved with low radiosurgical dose to the cochlea [19].
Sughrue ME, et al. [20] observed that the most common complications associated with surgical resection of vestibular Schannoma is facial nerve disorder (25.0%), cerebrospinal fluid leakage (8.5%) and postoperative neurological complications (8.4%) [20].
Conclusion
Cellular Schwannomas is an uncommon variant of Schwannoma. Local recurrence in cellular schwannoma may observe related to its high cellularity, increased mitotic activity, and resection extent and tumor size. The long-term follow-up is recommended in these cases.
Acknowledgement: None
Conflicts of Interest: None
Financial support: None
Patient’s Consent: NA
Ethical Approval: NA
Contribution of Authors: All contributed equally.
There is no any prior publication or ‘under consideration’ for publication of the manuscript.
References
-
Erickson NJ, Schmalz PGR, Agee BS, Fort M, Walters BC, et al. (2018) Koos classification of vestibular schwannomas: a reliability study. Neurosurgery 85(3): 409-414.
-
Cioffi G, Yeboa M, Kelly N, Patil N, Manzoor K, et al. (2020) Epidemiology of vestibular schwannoma in the United States, 2004-2016. NeuroOncol Adv 2(1): 1-8.
-
Nakatomi H, Jacob JT, Carlson ML, Tanaka S, Tanaka M, et al. (2017) Longterm risk of recurrence and regrowth after gross-total and subtotal resection of sporadic vestibular schwannoma. J Neurosurg 133(4): 1052- 1058.
-
Lee SU, Bae YJ, Kim HJ, Choi JY, Song JJ, et al. (2019) Intralabyrinthine Schwannoma: Distinct Features for Differential Diagnosis. Front Neurol 10: 750.
-
Coy S, Rashid R, Stemmer-Rachamimov A, Santagata S (2020) An update on the CNS manifestations of neurofibromatosis type 2. Acta Neuropathol 139(4): 643-665.
-
Ostrom QT, Cioffi G, Gittleman H, Patil N, Waite K, et al. (2019) CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012-2016. Neuro Oncol 21(Suppl 5): 1-100.
-
McLendon R, Rosenblum M, Bigner D (2012) Russell & Rubinstein’s Pathology of Tumors of the Nervous System 7Ed. Aufl, CRC Press, UK, 7: 1104.
-
Babu R, Sharma R, Bagley JH, Hatef J, Friedman AH, et al. (2013) Vestibular schwannomas in the modern era: epidemiology, treatment trends, and disparities in management. J Neurosurg 119(1): 121-130.
-
Lin EP, Crane BT (2017) The Management and Imaging of Vestibular Schwannomas. AJNR Am J Neuroradiol 38(11): 2034-2043.
-
Woodruff JM, Godwin TA, Erlandson RA, Susin M, Martini N (1981) Cellular schwannoma: a variety of schwannoma sometimes mistaken for a malignant tumor. Am J Surg Pathol 5(8): 733-744.
-
Jagtap SV, Shah HP, Jagtap SS, Beniwal, Raje V, et al. (2016) Large Thoraco-Lumbar Mass of Solitary Plexiform Neurofibroma: In A Patient of Neurofibromatosis Type- 1. Indian Journal of Pathology Research and Practice 5(2): 207-209.
-
Pekmezci M, Reus D, Hirbe A, Sonika Dahiya, David H Gutmann, et al. (2015) Morphologic and immunohistochemical features of malignant peripheral nerve sheath tumors and cellular schwannomas. Mod Pathol 28(2): 187-200.
-
Jagtap SV, Beniwal A, Shukla DB, Dahiya S, Gutmann DH, et. al. (2015) Malignant peripheral nerve sheath tumor of popliteal fossa. Int J Health Sci Res 5(1): 382-385.
-
Karamchandani JR, Nielsen TO, van de Rijn M, West RB (2012) Sox10 and S100 in the diagnosis of soft-tissue neoplasms. Appl Immunohistochem Mol Morphol 20(5): 445-450.
-
Perry A, Brat DJ (2018) Practical surgical neuropathology: a diagnostic approach. In: Livingstone C (Ed.), Pattern Recognition Series, Pathology 2: 17-42.
-
Hong B, Krauss JK, Bremer M, Karstens JH, Heissler HE, et al. (2014) Vestibular schwannoma microsurgery for recurrent tumors after radiation therapy or previous surgical resection. Otol Neurotol 35(1): 171-181.
-
Bailo M, Boari N, Gagliardi F, Franzin A, Piloni M, et al. (2017) Gamma Knife Radiosurgery for Residual and Recurrent Vestibular Schwannomas after Previous Surgery: Clinical Results in a Series of 90 Patients and Review of the Literature. World Neurosurgery 98: 60-72.
-
Fabbris C, Gazzini L, Paltrinieri D, Marchioni D (2020) Exclusive surgical treatment for vestibular schwannoma regrowth or recurrence: a meta-analysis of the literature. Clin Neurol Neurosurg 193: 105769.
-
Kano H, Kondziolka D, Khan A, Flickinger JC, Lunsford LD (2009) Predictors of hearing preservation after stereotactic radiosurgery for acoustic neuroma. J Neurosurg 111(4): 863-873.
-
Sughrue ME, Yang I, Aranda D, Rutkowski MJ, Fang S, et al. (2011) Beyond audiofacial morbidity after vestibular Schwannoma surgery. J Neurosurg 114(2): 367-374.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet