Incisive Canal Cyst (Nasopalatine Duct Cyst) in a Pediatric Patient – A Rare Case Report
Incisive canal cyst also called as Nasopalatine duct cyst is a rare non-odontogenic and non-neoplastic cyst occurring in the oral cavity. The most common occurrence in the general population usually varies from third to sixth decade. Development of this cyst is uncommon in children. Therefore, the aim of this case publication is to report an occurrence of incisive canal cyst in a 14-year-old Indian male patient. As this cyst is asymptomatic and painless most of the time it is accidentally diagnosed following a radiographic examination. Therefore, knowledge about its occurrence, diagnosis and management is utmost important among pediatric dentist.
Abbreviations
NPDC: Nasopalatine Duct Cyst.
Introduction
“Incisive Canal Cyst” also referred as “Nasopalatine Duct Cyst” (NPDC) is the most common developmental, non- odontogenic, non-neoplastic and epithelial cyst of the oral cavity [1]. This cyst develops from remnants of embryonic nasopalatine duct found with a prevalence of 1% in the general population. Other etiologic factors include local trauma, mucus retention and bacterial infection which may provoke the epithelial cell remnants of nasopalatine duct to proliferate and finally leading to cyst formation [2]. They are located in the midline of anterior maxilla (median of the palate) near the incisive foramen. The first description of this cyst is given by Meyer AW [3] in 1914, and called by various synonyms like incisive duct cyst, fissural cyst, maxillary midline cyst and anterior middle palatine cyst.
These cysts show a predilection for males than females (ratio ranging from 2.5:1) and reported in 40 to 60 years of age. Radiographically they found between the roots of the maxillary central incisors and appears as a heart-shaped radiolucency. Most of the time, they are asymptomatic and slow growing and rarely produce an elevation in the anterior portion of the palate [1, 2, 3]. The aim of this research paper is to showcase occurrence of incisive canal cyst in 14-year-old male Indian patient.
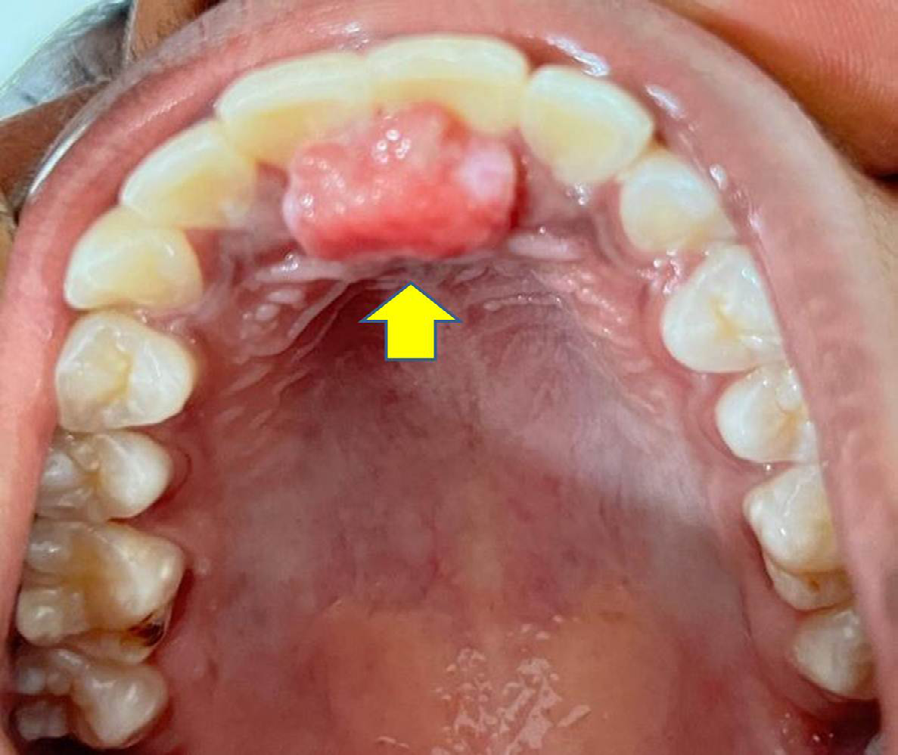
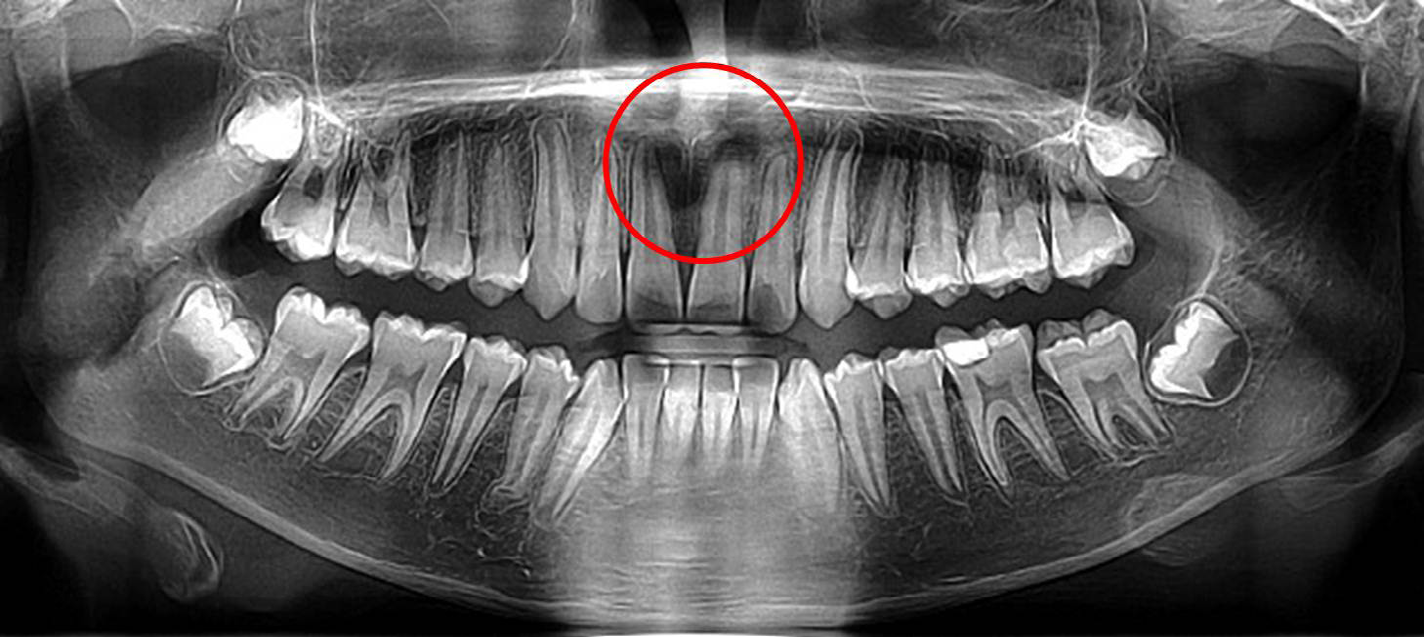
A 14-year-old Indian male patient reported to a private dental clinic seeking treatment for the irregularly positioned lower anterior teeth. Detailed examination of the patient was carried out and scheduled for the orthodontic treatment. After a month, patient reported complaining of small soft tissue swelling present behind the upper front teeth. The details of patient presented with soft tissue swelling is shown in Table 1 (Figures 1 & 2).
| Age Gender Ethnicity | Chief Complaint | Clinical Features (Figure 1) | Radiographic Features (Fig- ure 2) | Treatment Pro- vided |
|---|---|---|---|---|
| 14 years Male Indian | Complains of small swell- ing in the upper anterior portion of palate behind the upper anterior teeth. | A painless, small (2X3 cm) soft tissue swelling observed at the incisive papilla behind the maxillary two central incisors. Vitality test revealed vital cen- tral incisors. | An ovoid radiolucent lesion observed at the incisive fora- men between two maxillary central incisors on panoramic radiograph. | Surgical enucle- ation of the cyst |
Table 1: Patient details with Incisive Canal Cyst or Nasopalatine Duct Cyst.
Complains of small swelling in the upper anterior portion of palate behind the upper anterior teeth.
A painless, small (2X3 cm) soft tissue swelling observed at the incisive papilla behind the maxillary two central incisors.
Vitality test revealed vital central incisors. An ovoid radiolucent lesion observed at the incisive foramen between two maxillary central incisors on panoramic radiograph, surgical nucleation of the cyst.
Discussion
Exploring of dental literature pertaining to odontogenic and non-odontogenic pathologies including either cysts or tumors occurring in humans highlighted numerous publications [4, 5, 6, 7, 8, 9, 10]. Incisive canal cyst or nasopalatine duct cyst is rarely reported in children with first or second decade of life and reported more in adults. In differential diagnosis, periapical cyst or granuloma, inflammatory periapical lesions and sometimes wide incisive foramen is considered with the incisive canal cyst. Most of the time, they are asymptomatic and detected on routine radiographic examination [11, 12]. However, in some cases a tiny swelling or painful swelling and drainage at the anterior part of palate have been reported. But in the present case, patient had soft, painless small swelling in the anterior part of the palate behind the maxillary right and left central incisors. Recently Talebi A, et al. [2] reported occurrence of nasopalatine duct cyst as a delayed consequence of dental implant placement in the anterior maxilla while placement of a dental implant. In the case described here, clinical features, radiological features and histological features were suggestive for incisive canal cyst.
In larger cyst, the two central incisors get displaced along with its roots. Hence, based on their position these cysts are classified as central and unilateral. There is no prevalence for side affected. On radiographic examination, they appear as well-defined round or oval radiolucency in the dental midline, and sometimes appear as heart-shaped radiolucency. This is because during cyst expansion, the cyst becomes notched by the nasal septum or nasal spine is superimposed on the radiolucent area [11, 12, 13].
Management of this cyst includes surgical treatment which depends on the size and location of the cyst. If the cyst is large, marsupialization is recommended to first to reduce the size of the cyst later followed by enucleation. In addition to this autogenous bone grafting has also been suggested following cystectomy in case of larger cyst [1, 2, 3, 14]. During surgical enucleation of the cyst, incision and reflection of flap is carried out using either sublabial or palatine approach. In the present case too, palatine approach was used for the enucleation of the cyst. Histologically, in 71% of the cases, these cysts consist of columnar, squamous, cuboidal or some combination of these epithelial cell types. Respiratory epithelium was found in only 9.8% of cases [14, 15].
Francoli JE, et al. [12] performed a retrospective observational study comprising a period of 36 years from 1970-2006. Authors found only 22 patients with histopathological confirmation of nasopalatine duct cyst. In all cases, surgical treatment was carried out under local anesthesia which included the dissection and removal of the cyst adopting a usual palatine approach. No statistically significant correlation was observed between the size of the lesion and patient age, although the size of the cyst differed according to the patient gender with a mean diameter of 16 mm in males and 12 mm in females. Authors also recorded absence of root resorption and loss of vitality of the upper incisors following surgery. Radiological features showed rounded structure in 15 cases and heart-shaped structure in the remaining 7 cases. In the majority of the cases, periapical, occlusal and panoramic radiographs were used to identify the lesion.
However, in doubtful cases, computed tomography scan was also performed. In addition to the palatal approach, Sheikh OA, et al. [14] and Kagoya R, et al. [15] suggested management of this cyst by transnasal endoscopic marsupialization. Therefore, from the literature search it is evident that an awareness about occurrence of various intra oral soft tissue lesions is highly essential among clinicians dealing with children [4, 5, 6, 7, 8, 9, 10, 16, 17].
Conclusion
Although development of incisive canal cyst or nasopalatine duct cyst is rare, detailed knowledge about its occurrence, diagnosis, differential diagnosis and management is highly essential among all dental professionals to provide appropriate care to the patient.
References
-
Dedhia P, Dedhia S, Dhokar A, Deai A (2013) Nasopalatine duct cyst. Case Rep Dent 2013: 869516.
-
Talebi Ardakani M, Houshmand B, Kheiri A (2023) Nasopalatine duct cyst as a delayed consequence of dental implant placement in the anterior maxilla: A case report. J Adv Periodontol Implant Dent 15(2): 134-137.
-
Meyer AW (1914) A unique supernumerary paranasal sinus directly above the superior incisors. J Anat 48: 118-129.
-
Nagaveni NB (2023) Lateral periodontal cyst in a pediatric patient – report of a rare case. J Pediatr Dent Hyg 2(1): 1008.
-
Nagaveni NB, Umashankara KV, Radhika NB (2011) Inflammatory dentigerous cyst associated with an endodontically treated primary second molar: a case report. Arch Orofac Sci 6(1): 27-31.
-
Nagaveni NB, Umashankara KV, Radhika NB, Satisha TM (2011) Eruption cyst: A literature review and four case reports. Indian J Dent Res 22(1): 148-151.
-
Umashankara KV, Manjunath S, Nagaveni NB (2012) Ameloblastic fibro-dentinoma: Report of a rare tumor with literature review. J Cranio-Max Dis 1(2): 141.
-
Nagaveni NB, Umashankar KV, Ashwini KS, Chiranjeevi H (2024) Inversion of impacted mandibular third molar in ascending ramus of the mandible – report of a rarest case. Clin Pathol 8(1): 000185.
-
Nagaveni NB, Umashankar KV (2024) A giant radicular cyst involving the left maxillary sinus diagnosed on CBCT image-Report of a rare case. J Oral Health Dent 7(1): 591-595.
-
Nagaveni NB, Shashikiran N, Reddy VS (2009) Surgical management of palatal placed, inverted, dilacerated and impacted mesiodens. Int J Clin Pediatr Dent 2(1): 30-32.
-
Chen IJ, Lai PT, Jin YT, Chiang CP (2023) Nasopalatine duct cyst – Diagnosis from the content in the cystic wall. J Dent Sci 18(3): 1449-1451.
-
Francoli EJ, Marques AN, Aytes BL, Escoda GC (2008) Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cir Bucal 13(7): E438- 443.
-
Sheikh OA, Hussein AAM, Mukhtar AA. Abdi IA, Ahmed NM, et al. (2024) Nasopalatine duct cyst treated by Transnasal endoscopic marsupialization: A case report. Int Med Case Rep J 17: 459-464.
-
Kagoya R, Iwanami T, Mochizuki M, Kondo K, Ito K (2022) Case report: Unilateral transnasal endoscopic marsupialization of nasopalatine duct cyst. Front Surg 9: 978915.
-
Hasan S, Popli DB, Ahmad SA, Sircar A, Mansoori S, et al. (2022) Nasopalatine duct cyst with impacted inverted mesiodens: A rare case report and literature review. Case Rep Dent 2022: 5981020.
-
Umashankar KV, Khan MM, Prasad SM, Nagaveni NB (2024) Plunging ranula in a pediatric patient: A rare case report. IP Int J Maxillofac Imag 10(3): 117-120.
-
Basavanthappa NB, Nagaveni NB, Murthy NC, Amulya NP (2024) Sub-lingual implantation keratinized epidermoid cyst masquerading as plunging ranula: Report of a rare case with literature review. Indian J Otolaryngol Head Neck Surg 2024.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet