Case of Hairy Cell Leukemia – Rare Presentation
Hairy cell leukemia (HCL) is indolent chronic B-cell neoplasm involving the bone marrow, spleen, and peripheral blood. The complete blood count reveal pancytopenia. On peripheral blood examination reveal small to medium sized lymphocytes having circumferential villous projection with reniform nuclei and moderate amount of cytoplasm. Clinical features which patient usually present is Fever, generalized weakness and abdominal pain. On clinical examination may also reveal massive splenomegaly. Most common median age of presentation is approximately 55 year. Diagnosis for hairy cell leukemia is based on morphology, immunological phenotyping by flow cytometry, immunohistochemistry on trephine biopsy, and the presence of BRAFV600E mutation.
Singh R¹*, Billawaria S² and Alexender R¹
¹Pathology Consultant, Metropolis, India ²Department of Pathology, KD Medical College, India ³Pathology Consultant, Suburba Diagnostics, India *Corresponding author: Ramnik Singh, Consultant Pathologist, Metropolis Karad, India, Tel: 9969882580; Email: ramniksingh1995@gmail.com Keywords: Hairy Cell Leukemia; Flow Cytometry; Spleenomegaly
Abbreviations
HCL: Hairy cell leukemia; SMZL: Splenic Marginal Zone Lymphoma; WBC: White Blood Cells; CECT: Contrast-Enhanced Computed Tomography; IHC: Immunohistochemistry.
Introduction
Hairy cell leukemia (HCL) is a indolent B-cell neoplasm involving mainly the bone marrow, splenic red pulp and infiltrating the peripheral blood. The patient presents with lymphadenopathy, and massive splenomegaly or hepatomegaly. The neoplastic cells size vary from intermediate to small having ample amount of basophilic cytoplasm with hairy/ Villous slender projections and bearing BRAFp.V600E mutation in >95 % cases.
Differential diagnosis includes other B-cell lymphoproliferative disorders, including Splenic diffuse Red pulp B cell lymphoma, Splenic marginal zone lymphoma and Hairy cell leukemia variant (HCL-V) [1, 2].
Variant of HCL is more aggressive than Classical HCL and have a poor prognosis in response to standard treatment. In Variant of hairy cell leukemia the atypical lymphoid cells do not show positivity for CD25, CD200, and CD123 and is also negative for BRAFV600E gene mutation which is hallmark for Classical HCL .Patients with Variant of Hairy cell Leukemia have a significantly elevated white blood cell count and bone marrow aspiration is effortless in comparison to Classical Hairy cell Leukemia in which the WBCs count are not significantly raised and bone marrow aspiration in patients usually shows dry tap [3, 4].
In Variant of Hairy cell Leukemia abnormal lymphoid cells have morphology transitioning between prolymphocytes and hairy cells. Mutations in protein kinase 1 gene was identified was detected in HCL and in HCL-VTP53 aberrations was seen [5, 6, 7, 8].
SMZL is characterized by presence of abnormal lymphoid cells with round nuclei, condensed chromatin and basophilic cytoplasm with polar short villi in the peripheral blood. Heterogeneity in blood morphology is common, ranging from small lymphoid cells with cells also showing plasmacytoid to monocytoid differentiation. A panel of cd markers including CD11c, CD22, CD76, CD38, and CD27 help to differentiate SDRPL from SMZL. SMZL develops in the white pulp of the spleen lymphoma which may also involving the red pulp in diffuse or patchy patterns with subsequent spread to the sinuses.
SDRPL is shows small to medium-sized lymphoid cells with coarse to vesicular chromatin having 1-2 prominent nucleoli. The abnormal lymphoid cells have villous projection only over the polar surface of the cell. The CD200/CD180 helpful to distinguishing HCL from SDRPL. The BRAFV600E mutation is absent in SDRPL and present in HCL [9, 10, 11].
Case Report
A 63 year male came with complaints of fever and pain in abdomen since 4 months which was gradually progressive and worsened in last 4 months. He also had B symptoms of fever and significant weight loss. Clinical examination and on USG revealed massive splenomegaly with spleen reaching upto the 1 cm below the umbilicus.
Complete blood count showed Hemoglobin 13.7 g/dl, TLC – 18,640/mm3 and Platelets – 45000/mm3.
- Differential counts showed an absolute neutrophil count of 2423,
- Absolute lymphocyte count 15471 Peripheral Blood smear examination revealed RBC morphology anisopokilocytosis with microcytic hypochromic
picture with occasional NRBCS. WBC morphology revealed atypical cells (hairy cells) which are intermediate to small size having abundant amount of basophilic cytoplasm and reniform nuclei, open chromatin and occasional nucleoli and a characteristic circumferential villous/ serrated cytoplasm (Figures 3 & 4).
On clinical examination of abdomen revealed massive enlargement of spleen reaching upto the umbilicus.
Bone Marrow Aspiration revealed suppression of erythroid and myeloid series, with marked increase in lymphoid cells with moderate amount of cytoplasm showing projections (Figures 5 & 6).
Bone Marrow Biopsy revealed moderate increase in small to medium size lymphoid cells having fried egg appearance with mild fibrosis. Features suggestive for hairy cell leukemia / SLVL (Figure 7).
On IHC revealed positivity for CD20, PAX5, DBA44, Annexin A1 and TRAP.
- Weak positivity for Cyclin D1
- Negative for CD3, CD5, CD10 and CD23.
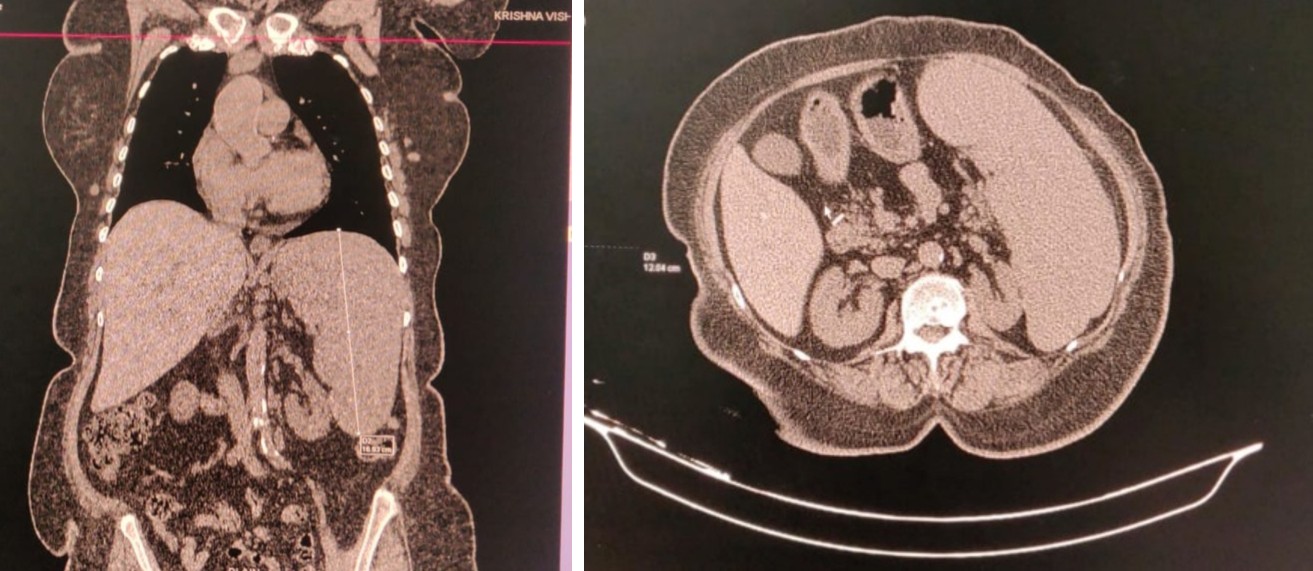
Contrast-enhanced computed tomography (CECT) of the neck and thorax, revealed no significant abnormality. CT ABDOMEN shows enlarged spleen (Figures 1 & 2) upto 20 cm with normal density.
Flow Cytometry revealed positivity for CD11c, CD 19, CD 20, CD 25, CD 38, Lambda, CD 200 and CD 103.
Figures 1 & 2: CT images of abdomen shows enlarged spleen with size more than 20 cm suggestive of spleenomegaly with normal density
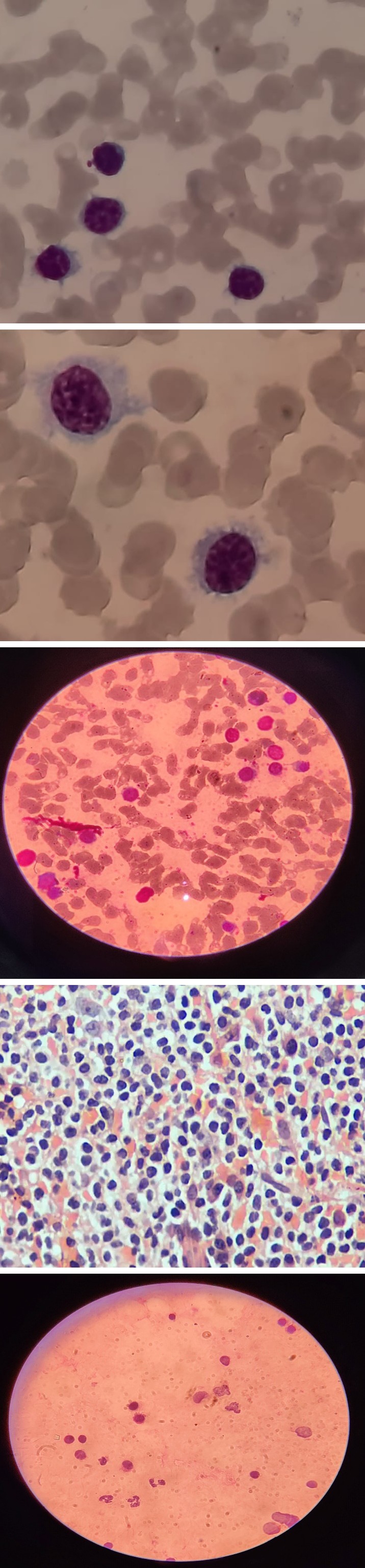
Figures 3 & 4: Peripheral smear show hairy cells that are small to medium in size moderate abundant pale blue cytoplasm, reniform nuclei, open chromatin occasional nucleoli and a characteristic serrated cytoplasmic border.
Figures 5 & 6: Shows bone marrow aspiration revealing small to medium sized cells with hairy projections.
Discussion
Hairy cell leukemia (HCL) is a chronic lymphoproliferative disorder characterized by bone marrow failure due infiltration malignant B cells with villous projections over the cytoplasm [12].
The hairy / villous morphology of the cells are mainly due to the actins and phosphoproteins [13, 14]. HCL cells are monoclonal B cells which are arrested at the late stage of differentiation showing a strong light-chain restricted surface immunoglobulin. The cell arise from germinal centre of the spleen and cause its infiltration which is the characteristic finding in HCL.
The red-pulp hypertrophy is responsible for massive spleenomegaly whereas the white pulp containing the suspected counterpart memory B cells undergoes atropy [15, 16].
The primary mutation in HCL is BRAF V600. Extracellular stimuli at cellular and molecular level along with adjacent cells, matrix proteins and cytokines in the bone marrow and spleen with specialized local stroma cells is vital for aggregation and persistence of HCL cells and responsible for tissue infiltration [17, 18].
In the bone marrow, the cellular components of the microenvironment can divided into two specialized compartments: an endosteal niche where the HSCs hide in a quiescent state and the sinusoidal–vascular niche where the HSCs stock up the peripheral blood cell counts. Mesenchymal bone marrow stromal secrete chemokines and express ligands for diverse adhesion molecules leading to activation of various signaling pathways involved in survival and growth of HCL [19].
HCL occurs in elderly with age group. Usually present with abdominal discomfort or pain which is secondary to splenomegaly and hepatomegaly Symptoms such as bleeding or recurrent infections are due to cytopenias. Usually have a late onset due to nonspecific symptoms of weakness, easy fatigue and dragging pain in the abdomen. Complete blood count of HCL shows leukocytosis and may develop cytopenias with time because of hypersplenism. On peripheral blood examination show small-to-medium lymphocyte that have abundant pale blue cytoplasm with hair-like projection. Nucleus is paracentral, reniform and has open chromatin with absent nucleoli.
SMZL with villous lymphocytes is another indolent B-cell lymphoma that may be mistaken for HCL which have unipolar or bipolar cytoplasmic projections rather than circumferential projections, as seen in HCL.
Splenic marginal zone lymphoma shows abnormal lymphoid cells with oval nuclei with vesicular to coarse chromatin and basophilic cytoplasm with villous projections over the polar surface . SDRPL is next closest differential to HCL which is characterized by the presence of a large proportion of small to medium-sized villous lymphoid cells in peripheral blood. The abnormal lymphoid cells have a polar distribution of the villi, and the nucleolus is small or invisible [20, 21].
Conclusion
Classic HCL is a rare type of B-cell chronic lymphoid leukemia characterized by splenomegaly, pancytopenia with reactive marrow fibrosis. Bone marrow studies is definitive diagnosis for HCL and confirmed on flow cytometry for morphology (CD19, CD20 or CD22) and anti- B cell antibodies markers as well as using more specific markers, such as CD11c, CD25, CD103, CD123 and TRAP staining for confirmation. Classic HCL shows positivity for BRAFV600E mutation, which is disease-defining genetic event.
References
-
King AC, Kabel CC, Pappacena JJ, Stump SE, Daley RJ 2019) No Loose Ends: A Review of the Pharmacotherapy of Hairy Cell and Hairy Cell Leukemia Variant. Ann Pharmacother 53(9): 922-932.
-
Kreitman RJ, Dearden C, Zinzani PL, Delgado J, Karlin L, et al. (2018) Moxetumomab pasudotox in relapsed/ refractory hairy cell leukemia. Leukemia 32(8): 1768- 1777.
-
Paillassa J, Safa F, Troussard X (2022) Updates in hairy cell leukemia (HCL) and variant-type HCL (HCL-V): rationale for targeted treatments with a focus on ibrutinib. Ther Adv Hematol 13.
-
Liu Q, Harris N, Epperla N, Andritsos LA (2021) Current and emerging therapeutic options for hairy cell leukemia variant. Onco Targets Ther 14: 1797-1805.
-
Forconi F, Sozzi E, Cencini E, Zaja F, Intermesoli T, et al. (2009) Hairy cell leukemias with unmutated IGHV genes define the minor subset refractory to single-agent cladribine and with more aggressive behavior. Blood 114(21): 4696-4702.
-
Hockley SL, Else M, Morilla A, Wotherspoon A, Dearden C, et al. (2012) The prognostic impact of clinical and molecular features in hairy cell leukaemia variant and splenic marginal zone lymphoma. Br J Haematol 158(3): 347-354.
-
Durham BH, Getta B, Dietrich S, Taylor J, Won H, et al. (2017) Genomic analysis of hairy cell leukemia identifies novel recurrent genetic alterations. Blood 130(14): 1644-1648.
-
Chihara D, Arons E, Stetler-Stevenson M, Yuan C, Wang H, et al. (2021) Long term follow-up of a phase II study of cladribine with concurrent rituximab with hairy cell leukemia variant. Blood Adv 5(23): 4807-4816.
-
Traverse-Glehen A, Baseggio L, Salles G, Coiffier B, Felman P, et al. (2012) Splenic diffuse red pulp small-B cell lymphoma: toward the emergence of a new lymphoma entity. Discov Med 13(71): 253-265.
-
Baseggio L, Traverse-Glehen A, Callet-Bauchu E, Morel D, Magaud JP, et al. (2011) Relevance of a scoring system including CD11c expression in the identification of splenic diffuse red pulp small B-cell lymphoma (SRPL). Hematol Oncol 29(1): 47-51.
-
Curiel-Olmo S, Mondéjar R, Almaraz C, Mollejo M, Cereceda L, et al. (2017) Splenic diffuse red pulp small B-cell lymphoma displays increased expression of cyclin D3 and recurrent CCND3 mutations. Blood 129(8): 1042-1045.
-
Campo E, Swerdlow SH, Harris NL, Pileri S, Stein, H, et al. (2011) The 2008 WHO classification of lymphoid neoplasms and beyond: Evolving concepts and practical applications. Blood 117(19): 5019-5032.
-
Miyoshi EK, Stewart PL, Kincade PW, Lee MB, Thompson AA, et al. (2001) Aberrant expression and localization of the cytoskeleton-binding pp52 (LSP1) protein in hairy cell leukemia. Leuk Res 25(1): 57-67.
-
Zhang X, Machii T, Matsumura I, Ezoe S, Kawasaki A, et al. (2003) Constitutively activated Rho guanosine triphosphatases regulate the growth and morphology of hairy cell leukemia cells. Int J Hematol 77(3): 263-273.
-
Catovsky D, Pettit JE, Galetto J, Okos A, Galton DA (1974) The B- lymphocyte nature of the hairy cell of leukaemic reticuloendotheliosis. Br J Haematol 26(1): 29-37.
-
Matutes E, Morilla R, Owusu-Ankomah K, Houliham A, Meeus P, et al. (1994) The immunophenotype of hairy cell leukemia (HCL). Proposal for a scoring system to distinguish HCL from B-cell disorders with hairy or villous lymphocytes. Leuk Lymphoma 14(Suppl. 1): 57- 61.
-
Morrison SJ, Spradling AC (2008) Stem Cells and Niches: Mechanisms That Promote Stem Cell Maintenance throughout Life. Cell 132(4): 598-611.
-
Sivina M, Kreitman RJ, Peled A, Ravandi F, Burger JA (2011) Adhesion of Hairy Cells Leukemia (HCL) Cells to Stromal Cells Can Be Inhibited by Blocking VLA- 4 Integrins and CXCR4 Chemokine Receptors. Blood 118(21): 1760.
-
Iwasaki H, Suda T (2009) Cancer stem cells and their niche. Cancer Sci 100(7): 1166-1172.
-
Visentin A, Imbergamo S, Trimarco V, Pravato S, Gargarella LR, et al. (2020) Ibrutinib in relapsed hairy cell leukemia variant: a case report and review of the literature. Hematol Oncol 38(5): 823-826.
-
Otieno SB, Ogbeide O (2022) Remarkable response of hairy cell leukemia variant to single-agent cladribine. Cureus 14(5): e24976.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet