African Histoplasmosis Misdiagnosed as Tuberculosis: A Case Report and Literature Review
African histoplasmosis, caused by Histoplasma capsulatum var. duboisii, is a rare fungal infection endemic to sub-Saharan Africa, including Uganda. It primarily affects the skin, subcutaneous tissues, and bones, often mimicking more common conditions such as tuberculosis (TB). This report describes a 35-year-old Ugandan male who presented with a chronic, non-healing ulcer on his upper right arm, initially misdiagnosed and treated as TB for three months without improvement. Histopathological analysis of a biopsy revealed granulomatous inflammation with large, thick-walled yeasts characteristic of H. capsulatum var. duboisii, confirmed using Grocott methenamine-silver and Periodic Acid-Schiff stains. The patient was subsequently treated with itraconazole, resulting in significant clinical improvement. This case highlights the diagnostic challenges of African histoplasmosis in resource-limited settings and emphasizes the critical role of histopathology in differentiating it from other chronic infectious diseases. Increased clinician awareness and diagnostic capacity are essential for timely and accurate diagnosis.
Abbreviations
GMS: Grocott Methenamine-Silver; PAS: Periodic Acid-Schiff; TB: Tuberculosis; H&E: Hematoxylin and Eosin.
Introduction
African histoplasmosis is a rare fungal infection caused by Histoplasma capsulatum var. duboisii, endemic to tropical regions of Africa, including Uganda. Unlike the more common form of histoplasmosis caused by H. capsulatum var. capsulatum, which predominantly affects the lungs, H. capsulatum var. duboisii primarily involves the skin, subcutaneous tissues, and bones [1]. The disease manifests with a range of symptoms, including nodules, ulcers, and abscesses, which often mimic other chronic infections such as tuberculosis or leprosy [2].
Diagnosing African histoplasmosis in Uganda remains challenging due to its clinical overlap with more common infectious conditions such as tuberculosis, which has a high prevalence in the region. This diagnostic challenge is compounded by limited access to advanced diagnostic tools in many healthcare facilities. Histopathological examination, combined with special stains like Grocott methenamine- silver (GMS) and Periodic Acid-Schiff (PAS), is critical for identifying the characteristic large, thick-walled yeasts [3]. Despite its potential severity, African histoplasmosis is

frequently underdiagnosed in Uganda, leading to delayed or inappropriate treatment [4]. This report describes a rare case of cutaneous African histoplasmosis in a 35-year- old Ugandan male misdiagnosed as tuberculosis. The case underscores the importance of histopathological evaluation in diagnosing chronic ulcers and highlights the need for increased clinician awareness and diagnostic capacity in endemic regions like Uganda.
Case Presentation
Clinical History
A 35-year-old male from a rural area in Uganda presented to Kayunga Regional Referral Hospital with a painless, non-healing ulcer on his upper right arm. The lesion had progressively enlarged over six months, accompanied by swelling on his limbs. He reported no systemic symptoms such as fever, weight loss, or night sweats. Initially, the ulcer was suspected to be tuberculosis (TB)-related, and he was started on empirical anti-TB treatment. However, after three months of therapy, there was no clinical improvement, prompting further investigation.
Figure 1A: Showing a non-healing ulcer on his upper right arm. Figure 1B: Showing non-tender swellings on the left limb.
On physical examination, the lesion was an ulcerated plaque with raised, indurated edges and an erythematous base. Multiple non-tender swellings were observed on his limbs, but there was no regional lymphadenopathy (Figure 1A & 1B).
The rest of the systemic examination was unremarkable. The patient denied any history of trauma, travel outside Uganda, or contact with individuals with similar symptoms.
Histopathological Findings
A biopsy from the wound edge was obtained and submitted to the Department of Pathology at Mulago National Referral Hospital for analysis. Three hematoxylin and eosin (H&E) stained sections were examined.
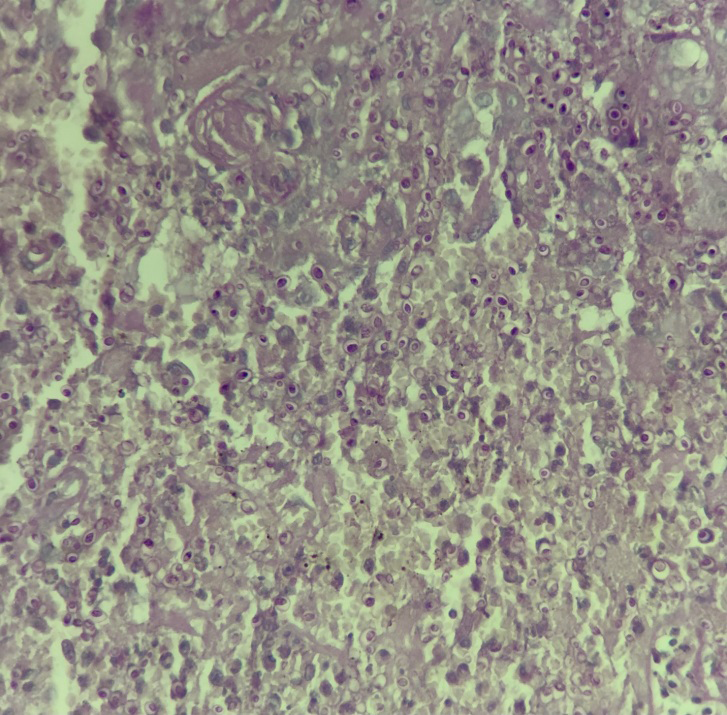
Microscopy revealed granulomas composed of macrophages, lymphocytes, plasma cells, neutrophils, and multinucleated giant cells. Numerous large, thick-walled, intracellular yeasts with clear halos were observed within macrophages and multinucleated giant cell (Figure 2). No evidence of malignancy was noted.
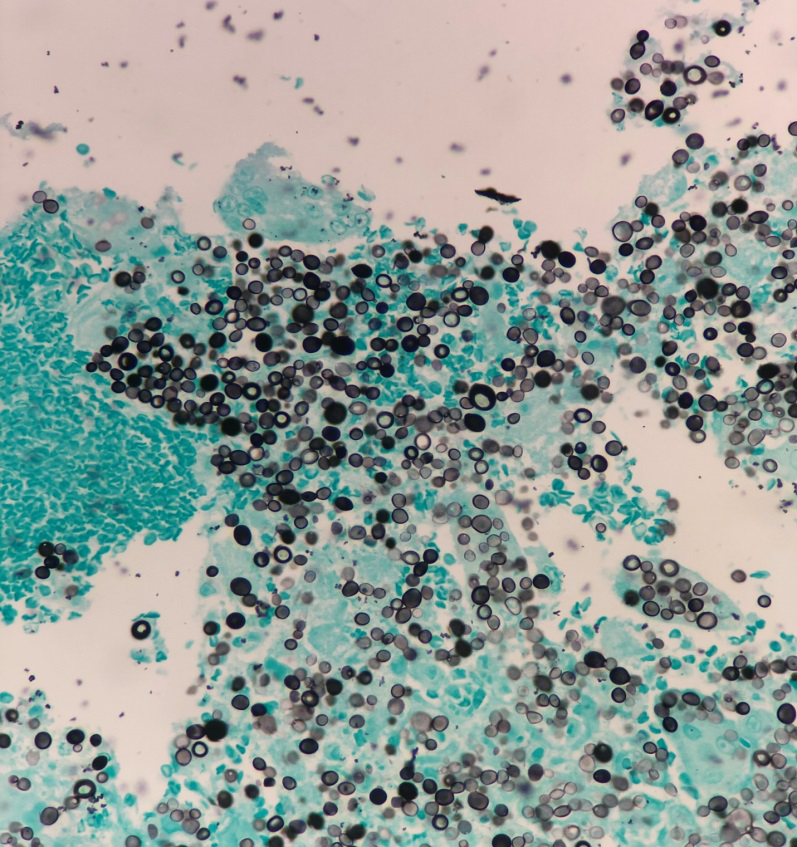
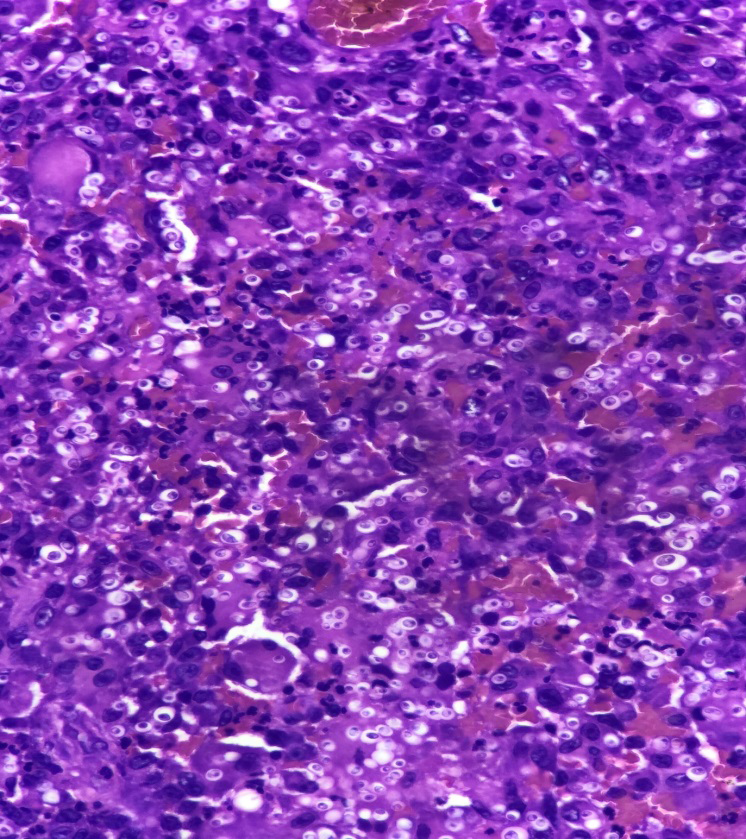
$$ \text{Figure 4: GMS stain showing fungal elements (magnification} \times 200). $$ To confirm the diagnosis, special stains were employed. Periodic Acid-Schiff (PAS) (Figure 3) and Grocott methenamine-silver (GMS) (Figure 4) stains highlighted the fungal elements, confirming the presence of Histoplasma capsulatum var. duboisii. Based on these findings, a diagnosis of cutaneous African histoplasmosis was established.
Clinical Course
The patient was referred to a specialist for antifungal therapy with itraconazole. After initiating treatment, the ulcer showed significant improvement within six weeks. He remains under follow-up for monitoring and to rule out systemic involvement.
Discussion
African histoplasmosis, caused by Histoplasma capsulatum var. duboisii, is a rare yet significant fungal infection endemic to sub-Saharan Africa. The disease disproportionately affects individuals in tropical regions, with Uganda being part of its endemic belt. Its clinical manifestations vary, with cutaneous, subcutaneous, and osteolytic lesions being the most common presentations. The rarity of the condition, combined with overlapping symptoms with other tropical diseases such as tuberculosis, poses significant diagnostic challenges [5, 6].
This case underscores the diagnostic dilemmas in endemic settings. Chronic ulcers and non-healing lesions are common clinical problems in tropical regions, frequently attributed to tuberculosis, bacterial infections, or malignancies. Such assumptions often lead to mismanagement, as seen in this patient, who was treated for tuberculosis for three months without improvement. Studies have reported similar scenarios where African histoplasmosis was initially misdiagnosed as TB or leprosy, delaying appropriate treatment [7].
Histopathology is critical in diagnosing African histoplasmosis. The hallmark features include granulomatous inflammation with macrophages and multinucleated giant cells containing large, thick-walled yeast forms. Special stains, such as Grocott methenamine-silver (GMS) and Periodic Acid- Schiff (PAS), enhance fungal visualization by staining fungal walls distinctly [8]. In this case, histopathology confirmed the diagnosis by demonstrating these typical features. However, the reliance on advanced histopathological techniques can be challenging in resource-constrained settings where such diagnostics may not be readily available.
Molecular diagnostics, such as polymerase chain reaction (PCR) for fungal DNA, have been explored as complementary tools for diagnosing fungal infections, including histoplasmosis. However, these techniques remain underutilized in many low- and middle-income countries [9, 10]. The absence of these advanced tools in rural Uganda highlights the need for investment in laboratory capacity and training to enhance early and accurate diagnosis.
The clinical features of African histoplasmosis often mimic those of other chronic infectious diseases prevalent in tropical regions. Differential diagnoses include cutaneous tuberculosis, leishmaniasis, cryptococcosis, blastomycosis, and bacterial ulcers such as Buruli ulcer. Malignancies, such as cutaneous squamous cell carcinoma, should also be considered, especially in non-healing lesions [11, 12]. The initial misdiagnosis of this case as tuberculosis illustrates the importance of considering fungal infections in the differential diagnosis of chronic ulcers, particularly in endemic areas.
The management of African histoplasmosis hinges on antifungal therapy. Itraconazole, an azole antifungal, is the first-line treatment for localized disease due to its oral administration, efficacy, and tolerability [13]. For severe or disseminated cases, liposomal amphotericin B remains the drug of choice, followed by oral itraconazole for maintenance therapy [14]. In this patient, itraconazole therapy led to significant clinical improvement within six weeks, emphasizing its effectiveness in localized disease.
Despite being endemic, African histoplasmosis remains poorly studied in Uganda and other parts of sub-Saharan Africa. There is limited information on the disease’s true prevalence, risk factors, and natural history. Research efforts should prioritize epidemiological studies to determine the burden of the disease and clinical studies to evaluate the efficacy of different treatment regimens. Investment in diagnostic research, including point-of-care tests, would also significantly enhance disease detection in low-resource settings [15].
Conclusion
This case highlights the importance of considering African histoplasmosis in the differential diagnosis of chronic ulcers, particularly in endemic regions like Uganda. Accurate diagnosis relies heavily on histopathological evaluation, supported by special stains. Misdiagnosis as tuberculosis or other conditions not only delays appropriate treatment but also increases morbidity. Efforts to improve fungal disease diagnosis, ensure access to antifungal therapy, and enhance clinician awareness are critical for addressing this neglected tropical disease. Collaboration between health systems, public health programs, and researchers is essential to reduce the burden of African histoplasmosis and improve patient outcomes.
Acknowledgments
We express our gratitude to the technical teams at the Department of Pathology, Mulago National Referral Hospital, the Uganda Cancer Institute (UCI), and the Department of Pathology at Makerere University for their exceptional technical support.
Ethical Approval
This case report did not require ethical approval based on local and national guidelines.
Consent
Written informed consent was obtained from the patient for the publication of this case and accompanying images. The investigation adhered to the principles outlined in the Declaration of Helsinki (1975).
Conflict of Interest
The authors declare no conflicts of interest.
Funding
This study did not receive any specific funding from organizations or institutions.
Data Availability
All data generated or analyzed in this study are included within this article. For additional details, inquiries can be directed to the corresponding author.
Author Contributions
O.P. was responsible for conceptualization, methodology, investigation, and data curation. M.S. contributed to the methodology and performed the initial pathological diagnosis. B.M. drafted the manuscript. T.O., M.A., O.M., G.A., W.E., B.E., M.J.D., N.J., K.M., A.R., N.G., L.R., B.P., and Y.M. reviewed the manuscript and contributed to the methodology. N.B. performed the special stains. K.F. conducted the biopsy, and K.S. provided the final pathological diagnosis. All authors reviewed and approved the final manuscript.
References
-
Develoux M, Amona FM, Hennequin C (2021) Histoplasmosis Caused by _Histoplasma capsulatum_ var. duboisii: A Comprehensive Review of Cases From 1993 to 2019. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 73(3): e543-e549.
-
Khathali LC, Nhlonzi GB, Mwazha A (2022) _Histoplasma_ _capsulatum_ var. duboisii: A KwaZulu-Natal, South Africa public sector perspective. Journal of cutaneous pathology 49(2): 139-146.
-
Guarner J, Brandt ME (2011) Histopathologic diagnosis of fungal infections in the 21st century. Clinical microbiology reviews 24(2): 247-280.
-
Ocansey BK, Kosmidis C, Agyei M, Dorkenoo AM, Ayanlowo OO, et al. (2022) Histoplasmosis in Africa: Current perspectives, knowledge gaps, and research priorities. PLoS neglected tropical diseases 16(2): e0010111.
-
Bongomin F, Fayemiwo SA (2021) Epidemiology of fungal diseases in Africa: A review of diagnostic drivers. Current medical mycology 7(1): 63-70.
-
Gugnani HC (2000) Histoplasmosis in Africa: a review. The Indian journal of chest diseases & allied sciences 42(4): 271-277.
-
Kuate MPN, Ekeng BE, Kwizera R, Mandengue C, Bongomin F (2021) Histoplasmosis overlapping with HIV and tuberculosis in sub-Saharan Africa: challenges and research priorities. Therapeutic advances in infectious disease 8: 20499361211008675.
-
Guemas E, Sobanska L, Demar M (2020) _Histoplasma_ _capsulatum_ and Histoplasmosis: Current Concept for the Diagnosis. IntechOpen 92782.
-
Khot PD, Fredricks DN (2009) PCR-based diagnosis of human fungal infections. Expert review of anti-infective therapy 7(10): 1201-1221.
-
Gudisa R, Harchand R, Rudramurthy SM (2024) Nucleic- Acid-Based Molecular Fungal Diagnostics: A Way to a Better Future. Diagnostics (Basel, Switzerland) 14(5): 520.
-
Ekeng BE, Edem K, Akintan P, Oladele RO (2022) Histoplasmosis in African children: clinical features, diagnosis and treatment. Therapeutic advances in infectious disease 9: 20499361211068592.
-
Ocansey BK, Kosmidis C, Agyei M, Dorkenoo AM, Ayanlowo OO, et al. (2022) Histoplasmosis in Africa: Current perspectives, knowledge gaps, and research priorities. PLoS neglected tropical diseases 16(2): e0010111.
-
Wheat J, Hafner R, Korzun AH, Limjoco MT, Spencer P, et al. (1995) Itraconazole treatment of disseminated histoplasmosis in patients with the acquired immunodeficiency syndrome. AIDS Clinical Trial Group. The American journal of medicine 98(4): 336-342.
-
Pasqualotto AC, Lana DD, Godoy CSM, Leitão TDMJS, Bay MB, et al. (2023) Single High Dose of Liposomal Amphotericin B in Human Immunodeficiency Virus/ AIDS-Related Disseminated Histoplasmosis: A Randomized Trial. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 77(8): 1126-1132.
-
Oladele RO, Ayanlowo OO, Richardson MD, Denning DW (2018) Histoplasmosis in Africa: An emerging or a neglected disease. PLoS neglected tropical diseases 12(1): e0006046.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet