Clinical Presentation and Risk Factors of Pediatric Chronic Supportive Otitis Media: A Single Institution Pilot Study
Chronic supportive otitis media (CSOM) is the most common cause for hearing loss. It is an important cause of preventable hearing loss, particularly in the developing world. Objectives of this study are: To study the clinical presentation and risk factors of CSOM. Materials and methods: A prospective, cross sectional, analytic study conducted during the period (Sep to Nov 2019) in Khartoum ENT Teaching Hospital, including all pediatric patients below 18 years who presented with CSOM without otitis external and agreed to participate in the study. Chi square test was used to calculate the P value for significance, regarded as significant if less than 0.05. Results: A total of 76 patients were enrolled in this study, male and females were almost equal, age raged from 2 to 17 years. Symptoms of CSOM were otorrhoea, hearing loss, ear pain, dizziness and itching in that order of frequency. Most of the disease was tubotympanic type (86.1%). Significant risk factors” included percentage among studied patients” were: Recurrent upper respiratory tract infections (88.2%), recent history of acute otitis media (77.6%), recurrent acute otitis media (77%), passive smoking (80.2%), bottle feeding (77.9%), flat position during breast\ bottle feeding (73.6%), poor hygiene (86.8%), low socio-economic status (72.4%), low level of mothers’ education (72.4%) and poor nutrition (73.6%). Risk factors are interrelated and interact with each other. Irrelevant factors were: Crowded house, regular swimming, ear cleaning habits, nasal allergy and ventilation tube insertion. Recommendations: A full scale project to study CSOM at a community level is recommended with involvement of health educators. Founding a protocol for management of CSOM in a multidisciplinary approach (ENT, Audiology, Immunology, Pediatric and school health providers).
Nazik E Abdulla1*, Nagwa M Ibrahem2 and Osama M Khalid1
Introduction
Chronic supportive otitis media (CSOM) is defined as chronic middle ear mucosal inflammation with tympanic membrane perforation and persistent or intermittent otorrhoea with a discharge persisting minimum of 2-6 weeks [1]. In CSOM, bacteria reach the middle ear either from the nasopharynx through the Eustachian tube, or from the external ear canal through a perforated tympanic membrane [2]. Bacteria that cause CSOM are both aerobic and anaerobic. Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella, Proteus, and E. coli species are the predominant [3]. Symptoms of CSOM are mainly recurrent otorrhoea and hearing loss, less frequent are tinnitus, pain, itching and dizziness/vertigo [4, 5]. If complicated by intracranial extension of infection, headache, nausea-vomiting and fever are additional symptoms [6].
CSOM is usually classified into two main groups: tubotympanic (TT) and atticoantral (AA) disease according to otoscopic examination. Tubotympanic disease is characterized by a perforation of the pars tensa. Atticoantral disease most commonly involves the pars flaccida and is characterized by the formation of a retraction pocket in which keratin accumulates to produce cholesteatoma [7].
Recurrent Chronic supportive otitis media (CSOM) is the leading cause of hearing impairment worldwide. It is an important cause of preventable hearing loss, particularly in the developing world. High prevalence of CSOM is associated with inadequate breast feeding, poor hygiene, low socioeconomic status, overcrowding, passive smoking, recurrent upper respiratory tract infections, impaired immune response, and colonization of nasopharynx by pathogenic organism and unavailability of health care facilities. Some studies have shown relationship between maternal education, bathing habits and ear cleaning habits [8].
Hearing impairment of any degree has a profound effect on children. It delays development of speech, slows educational progress and leads to being stigmatized [9]. To our knowledge, no study from Sudan was published on this subject, the aim of this pilot study is to through light on this disease in this part of the world.
Objectives
To study the clinical presentation and risk factors of pediatric chronic superlative otitis media in ENT Khartoum Teaching Hospital.
Materials and Methods
This is a cross sectional prospective analytical study carried out in ENT Khartoum Teaching Hospital which is a tertiary referral hospital in the capital of Sudan. All pediatric patients below 18 years who presented with chronic supportive otitis media without otitis external, and agreed (patients and/or guardians) to participate in this study were included. Study duration: From September 2019 to Nov 2019. Included patients underwent detailed history taking including a list of risk factors, followed by a general physical examination and ENT examination. Data was analyzed using computer and statistical package for social sciences (SPSS) version 22. P value was calculated using Chi square test, it is considered significant if less than 0.05.
Results
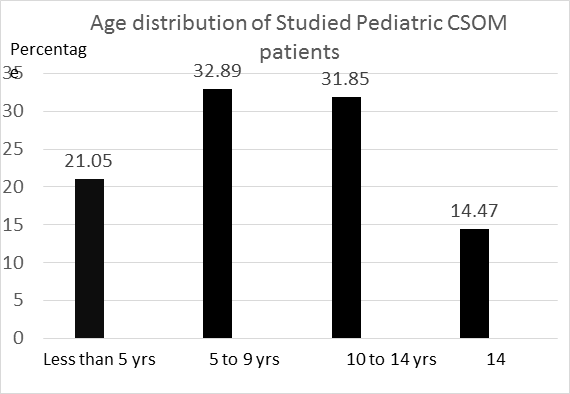
Total number of patients enrolled was 76 patients, age range was from 2 years to 17 years with the mean age of 9.9±0.98SD years. Two thirds of patients were in the age range of 5-14-year; details of age distribution are shown in Figure 1. Males were 40 patients (53%) and females were 36 patients (47%), with male to female ratio of 1.1:1.0, this difference was statistically insignificant (P value > 0.05).
Symptoms at presentation were studied, all patients complained of ear discharge, it was bilateral in 39% and profuse in 77.6%. Hearing loss was the second most common complaint, it is observed in 66 patients (86.8%). Ear pain was experienced by 24 patients (31.6 %), dizziness was a complaint of 3 patients (3.9%) and only one patient (1.3%)
complained of ear itching. Ear examination revealed central TM perforation, attic perforation, tympanosclerosis and middle ear polyp in that order of frequency as details are shown in Table 1.
| Frequency | percentage | |
|---|---|---|
| Central TM perforation | 90 ears | 83.30% |
| Attic TM perforation | 15 ears | 13.80% |
| Central TM perforation + Tympanosclerosis | One ear | 0.92% |
| Central TM perforation + Ear polyps | One ear | 0.92% |
| Attic TM perforation + Tympanosclerosis | One ear | 0.92% |
| Total | 108 | 100 |
Table 1: Otoscopic (ear) examination findings of CSOM patients, note total number of ears being examined is 108 and number of pat
History of recurrent upper respiratory tract infection was reported in (88.2%), Passive smoking in (80.2%), bottle feeding was practiced by (77.9%), Infant position on breast and/or bottle feeding was inquired, about 56 patients (73,6%) were fed flat, while 21patients (26,4%) were fed in an upright position. all these risk factors were statistically significant as shown in Table 2.
| Risk factors | Frequency | Percentage | P value |
|---|---|---|---|
| Recurrent Upper Respiratory Tract Infections | 67 | 88.20% | < 0.05 |
| Poor hygiene | 66 | 86.80% | < 0.05 |
| Passive smoking | 61 | 80.20% | < 0.05 |
| Bottle feeding | 59 | 77.90% | < 0.05 |
| Recent history of Acute Otitis Media | 59 | 77.90% | < 0.05 |
| Low level of mother’s education | 58 | 76.30% | < 0.05 |
| Recurrent Acute Otitis Media | 57 | 77.00% | < 0.05 |
| Flat position- Breast\bottle feeding | 56 | 73.60% | < 0.05 |
| Poor nutrition | 56 | 73.60% | < 0.05 |
| Low socio-economic status | 55 | 72.40% | < 0.05 |
| Crowded housing condition. More than 6 | 43 | 56.50% | > 0.05 |
| Symptoms of allergy | 39 | 51.10% | > 0.05 |
| Regular swimming | 16 | 22.10% | > 0.05 |
| Ear cleaning habit | 15 | 19.70% | > 0.05 |
| History of ventilation tube insertion | 3 | 3.90% | > 0.05 |
Table 2: Summary of studies risk actors of CSOM, arranged in order of frequency.
Episodes of Acute otitis media during the last one year were more than 6 episodes in 63.1% of patients, 3-6 episodes in 21.1 % and were less than 3 episodes in 15.8% of patients. Recent history of acute otitis media was observed in 59 patients (77.6%). Primary Healthcare was easily accessible for 48 patients (63.2%). Nasal symptoms suggestive of allergy were: Nasal discharge in 39 patients (51.3%), nasal obstruction in 28 patients (36.8%), sneezing in 25patients (32.9), post nasal drip in 22 patients (28.9%), snoring in 22 patients (28.9%) and facial pain in 14 patients (18.4%), all were statistically not significant (P value > 0.05).
Mothers’ education assessment revealed that mothers of primary school level and below were 58 (76.3%), while mothers of more than primary school level were 18 (23.7%), this difference was statistically significant (P value < 0.05).
Socioeconomic status study: The majority of patients 55 (72.4%) were found to be of low socioeconomic status (people cannot get basic things like education, treatment and nutrition) while 21patients (17.6%) were of good socioeconomic status (people can get basic things like education, treatment and nutrition), the difference was statistically significant (P value < 0.05).
Hygiene assessment revealed that 66 patients (86.8%) were of poor hygiene (not having daily bath, clean water and soap not always available) versus 10 patients (13.2%) of good hygiene (having daily bath, always available clean water and soap). The difference was strongly significant (P value < 0.05).
Nutrition is considered good when proteins, vegetables and minerals are regularly provided in the daily meals and vice versa. Poor nutrition was observed in 56 patients (73.7%), while 21patients (26.3%) had good nutrition. The difference was statistically significant (P value < 0.05).
Housing conditions in this study showed that 43 patients (56.5%) live in a house of more than 6 persons, 23 patients (30.3%) live as 3-6 persons in the house, only 10 patients (13.2%) were living as less than 3 persons per house. Ear cleaning habit was practiced by (19.7%), regular swimming was practiced by 16 patients (22.1 %) and ventilation tube or myringotomy was inserted for (3.9%), statistical significance of these factors is shown in Table 2.
Discussion
In this study of CSOM, the frequently affected children were those 5 to 14 years old, this is the school age, with expected consequent poor schooling due to impaired hearing especially if bilateral. This is an indication for special focus on hearing assessment and ear examination at screening level for this age group as part of Schools’ Health programs. No gender predominance in this study, this agrees with the majority of published data [10, 11]. Even in reports which showed gender predilection, predominance was trivial [12].
Regarding symptomatology, otorrhoea is the hallmark symptom of CSOM (100% of patients) and being recurrent signifies that the disease is active. The majority of studied patients (86.8%) suffered from hearing loss, the second most frequent symptom, and in a significant percentage 39% the disease was bilateral, making hearing loss as one of the most important problems and drawbacks caused by CSOM in this subset of patients.
World Health Organization (WHO) estimates the global burden of illness from CSOM at about 65-330 million individuals with ears discharge, 60% (39-200 million) of whom suffer from significant hearing impairment [12]. The percentage of hearing loss in our study, which is a hospital based, is higher than the global figure, this warrants a bigger scale project to study CSOM at a community based level.
Reasons of hearing loss in CSOM are: Tympanic membrane perforation and ossicular chain erosion. a simple model was suggested based on the auditory structure to predict hearing loss due to tympanic membrane perforation. Mehta et al used this model and demonstrated that hearing loss in case of tympanic membrane perforation is greater with larger size perforations [13]. Mechanism of ossicular erosion in CSOM is overproduction of cytokines-TNF alpha, interleukin-2, fibroblast growth factor, and platelet derived growth factor which promotes hyper vascularization, osteoclast activation, and bone resorption causing ossicular damage [14].
The third most frequent symptom in this study is ear pain (otalgia), it is present in 24 patients (31,6%), this agrees with a study done by Alabbasi AM, et al. [15], they reported otalgia in (40%) of patients as a symptom of CSOM, this could be attributed to attacks of acute infection of the middle ear cleft on top of a chronically discharging ear or a persistent perforation. Other symptoms were not frequent like tinnitus and itching in agreement of other studies [4]. Dizziness was reported by only 3 patients (3.9%), very low percentage when compared with Alabbasi AM, et al. study [15]. No symptoms of intracranial complications were reported among studied patients.
CSOM may occur as a part of a systemic condition, e.g. Wegener, M. tuberculosis, and histiocytosis X, where the mastoid and middle ear may be the localization of this specific inflammation in addition to other sites [16, 17, 18]. Absence of an association with systemic disease in this study could be attributed to the relatively small sample size.
Otoscopic examination demonstrated that the majority of studied ears (86.1%) were tubotympanic type of disease and only (13.9%) were atticoantral disease. Tubotympanic CSOM is not typically associated with intracranial complications [19]; this explains lack of symptoms that suggest intracranial complications among our studied patients.
Recurrent upper respiratory tract infection was the most prevailing significant risk factor, this is in agreement of reported studies [1, 18]. Recurrent respiratory tract infection could be associated with improper neutrophils response to pathogens, and immunological examination should be performed to find the reason for the increased number of infections in a year 20. Alkhater SA, et al. published a report that aims at providing guidelines for the evaluation of children with recurrent infections. It provides an overview of the diagnostic approach including important details required from the history, physical examination, and an appropriate choice of screening test to be ordered [20, 21].
Other causes of recurrent respiratory tract infections are: Allergies and malnutrition, particularly iron and zinc deficiencies [22]. In this study poor nutrition and history of nasal allergy were prevalent in a considerable number and both are known risk factors for recurrent upper respiratory infections. It is evident that CSOM is not only multifactorial, but different risk factors interact with each other. Recent history of acute otitis media (AOM) was reported in 59 patients (77.6%), and 48 patients (63.1%) experienced more than 6 episodes during the previous year, this association is reported in many studies [17, 18, 22, 23, 24]. Inadequate antimicrobial therapy of AOM may contribute to occurrence of CSOM [24].
Founding a protocol for the management and follow up of children with upper respiratory tract infections and acute otitis media at a primary health level is important, the protocol should be shared by ENT, pediatric, immunologist, nutritionist and school health professionals, aiming at reducing the risk of CSOM, correct nutritional deficiency and to early diagnose children with primary immune deficiency, considering the majority of our studied patients (63.2%) had easy access to primary health service.
Bottle feeding was a risk factor in our study, this association is reported by Van der veen EL, et al. and Dhingra R, et al. [22, 25]. Promotion of breast feeding should be initiated at a community level to explain its role in reducing the risk of CSOM beside its other benefits. In this study, (73.6%) of patients were usually fed flat in position during both breast and bottle feeding, whereas only 13,35% were most of the time fed in an upright position. This was statistically significant, and proves the importance of child’s position during feeding; lying flat is a risk factor for the development of CSOM.
Passive smoking was reported in (80.2 %) of patients, this is in agreement with many studies [26], ranking it as one of the top three risk factors in this study, this could be avoided by raising it in health education programs and antenatal care visits.
Mothers’ level of education, socioeconomic status, nutrition, housing conditions and hygiene are strongly interrelated, they are reflection of the general standard of living. From our data we can conclude that all these factors if of low quality are substantial risk factors of CSOM.
The exception of crowded housing environment as a risk factor of CSOM in this study, could be attributed to the nature of house structures in our country, where large outdoors areas and good ventilation are available even for people of low socioeconomic status.
Many studies reported regular swimming, ear cleaning habits and ventilation tube insertion as risk factors for CSOM. However, in our study these were not significant risk factors.
Conclusion
A total of 76 patients were enrolled in this study, male and females were almost equal, age raged from 2 to 17 years. Symptoms of CSOM were otorrhoea, hearing loss, ear pain, dizziness and itching in that order of frequency. Most of the disease was tybotympanic type (86.1%). Significant risk factors were: Recurrent upper respiratory tract infections, recurrent acute otitis media, recent history of acute otitis media, passive smoking, bottle feeding, flat position during breast\bottle feeding, poor hygiene, low socio-economic status, low level of mothers’ education and poor nutrition. Risk factors are interrelated and interact with each other. Irrelevant factors were: Crowded house, regular swimming, ear cleaning habits, nasal allergy and ventilation tube insertion.
Recommendations
From this pilot study, a full scale project to study CSOM at a community level is recommended with involvement of health educators. Founding a protocol for management of CSOM in a multidisciplinary approach (ENT, Audiology, Immunology, Pediatric and school health providers) aiming at reducing the incidence and drawbacks of CSOM.
References
-
Qureishi A, Lee Y, Belfield K, Birchall JP, Daniel M (2014) Update on otitis media-prevention and treatment. Infect Drug Resist 10(7): 15-24.
-
Basavaraj MC, Jyothi P (2015) Chronic Suppurative Otitis Media (CSOM): Etiological Agents and Antibiotic Sensitivity Pattern of the Isolates. J Medicine 16(2): 79- 82.
-
Prakash R, Juyal D, Negi V, Shekar P, Adekhandi S, et al. (2013) Microbiology of Chronic Suppurative Otitis Media in a Tertiary Care Setup of Uttarakhand State, India. N Am J Med Sci 5(4): 282-287.
-
Kumar N, Chilke D, Puttewar MP (2012) Clinical Profile of Tubotympanic CSOM and Its Management with Special Reference to Site and Size of Tympanic Membrane Perforation, Eustachian Tube Function and Three Flap Tympanoplasty. Indian J Otolaryngol Head Neck Surg 64(1): 5‐12.
-
Mostafa BE, Shafik AG, Makhzangy AM, Taha H, Mageed HMA (2014) Evaluation of Vestibular Function in Patients with Chronic Suppurative Otitis Media. ORL J Otorhinolaryngol Relat Spec 75(6): 357-360.
-
Yağız R, Adalı MK, Taş A, Karasalihoğlu A, Uzun C, et al. (2008) Intracranial Complications of Chronic Suppurative Otitis Media. Balkan Med J 25(3): 196-203.
-
Adhikar P, Joshi S, Baral D, Kharel B (2009) Chronic Suppurative Otitis Media in urban private school children of Nepal. Braz J Otorhinolaryngol 75(5): 669-672.
-
Khader KA, Parihar H, Mishra RK (2014) Etiological agents in Chronic Suppurative otitis Media. Int J Med Res Rev 2(5): 463-468.
-
Patel HC, Moitra M, Modi A, Contractor J, Kantharia SL (2014) Impact of Hearing Loss on Daily Life Style and Schooling among Children between 5 and 15 Years Age- Group. Natl J Community Med 5(1): 73-76.
-
Garud S, Buche A, Keche P, Chamania G (2017) Socioeconomic impact on prevalence of chronic suppurative otitis media in school going children in tribal district of India. Int J of Med Sci and Pub Health 6(4): 699-702.
-
Onotai LO, Osuji AE (2015) Chronic Suppurative Otitis Media in Nigerian Children: The Port Harcourt Experience. J of Advances in Med and Med Resarch 7(10): 833-838.
-
Nnebe-Agumadu U, Okike O, Orji I, Ibekwe RC (2011) Childhood suppurative otitis media in Abakaliki: Isolated microbes and in vitro antibiotic sensitivity pattern. Nigerian J Clin Pract 14(2): 159-162.
-
Rout MR, Mohanty D, Vijaylaxmi Y, Kamalesh B, Chakradhar M (2012) Prevalence of cholesteatoma in chronic suppurative otitis media with central perforation. Indian J Otol 18: 7-10.
-
Varshney S, Nangia A, Bist SS, Singh RK, Gupta N, et al. (2010) Ossicular chain status in chronic suppurative otitis media in adults. Indian J Otolaryngol Head Neck Surg 62(4): 421-426.
-
Alabbasi AM, Alsaimary IE, Najim JM (2010) Prevalence and patterns of chronic suppurative otitis media and hearing impairment in Basrah city. J Med Med Sci 1(4): 129-133.
-
Gupta R, Mittal M (2016) A study on clinical and epidemiological profile of chronic suppurative otitis media (CSOM) at a tertiary care center. Int J of Med Sci and Pub Health 5(5): 1021-1024.
-
Tsilis NS, Vlastarakos PV, Chalkiadakis VF, Kotzampasakis DS, Nikolopoulos TP (2013) Chronic Otitis Media in Children: An Evidence-Based Guide for Diagnosis and Management. Clinical pediatrics. 52(9): 795-802.
-
Morris PS (2009) Upper respiratory tract infections (including otitis media). Pediatr Clin North Am 56(1): 101-117.
-
Islam R, Taous A, Hossain M, Ekramuddaula AFM, Islam MS (2010) Comparative study of tubotympanic and atticoantral variety of Chronic suppurative otitis media. Bangladesh J Otorhinolaryngol 16(2): 113-119.
-
Raniszewska A, Górska E, Kotuła I, Stelmaszczyk- Emmel A, Popko K, et al. (2015) Recurrent respiratory tract infections in children - analysis of immunological examinations. Cent Eur J Immunol 40(2): 167‐173.
-
Alkhater SA (2009) Approach to the child with recurrent infections. J Family Community Med 16(3): 77‐82.
-
Veen EL, Schilder AGM, Heerbeek NV, Verhoeff M, Zielhuis GA, et al. (2006) Predictors of chronic suppurative otitis media in children. Arch of otolaryngology Head & neck Surgery 132(10): 1115-1118.
-
Verhoeff M, Veen EL, Rovers MM, Sanders EA, Schilder AG (2006) Chronicsuppurative otitis media: A review. Int J Pediatr otorhinolaryngol 70(1): 1-2.
-
Cunningham M, Guardiani E, Kim HJ, Brook I (2012) Otitis media. Future Medicine 7(6): 733-753.
-
Dhingra R, Dhillon V, Monga S, Mehta AS, Kaur G, et al. (2016) Sociodemographic profile and evaluation of associated factors in chronic suppurative otitis media patients reporting to tertiary care Hospital of Punjab. Int Archives of Integrated Med 3(6): 6-10.
-
Parvez A, Khan Z, Hashmi SF, Khan MS (2017) A cross sectional study of chronic suppurative otitis media and its associated factors among primary school children in rural and urban areas of Aligarh, India. Int J of Comm Med and Pub Health 3(8): 2150-2154.\
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria