Repurposing Drugs for Covid-19 by a Developing Country
Background: Early treatment of COVID-19 disease with repurposed drugs has been controversial. Most guidelines in the developed world recommend monoclonal antibodies or Ritonavir/Nirmatrelvir therapies for patients at risk of clinical deterioration, but accessibility to these in developing countries is a big challenge. The primary purpose of this study is to Epidemiology International Journal 2 Sekhon AK, et al. Repurposing Drugs for Covid-19 by a Developing Country. Epidemol Int J 2022, 6(2): 000234. Copyright© Sekhon AK, et al. review the impact of early treatment of COVID-19 with repurposed drugs on hospitalizations, oxygen requirement, and mortality in a limited resource setting. Methods: This observational cohort study was Institutional Review Board (IRB) approved. Data was collected from medical records from November 2020 until October 2021. A multiphasic multidrug protocol of repurposed drugs was used as COVID-19 outpatient therapy in Honduras. Patients within 7 days of disease onset and mild symptoms received Ivermectin, Aspirin, Colchicine, Fluvoxamine, and Famotidine. On day 7, patients received Prednisolone and Apixaban if CT-chest showed pulmonary infiltrates and inflammatory markers were elevated. Patients were followed every 24-72 hours, and pulse doses of methylprednisolone were given for clinical deterioration. Results: Of 415 patients, 208 were men (50.1%), and 207 women (49.9%). Average age of the cohort was 47.4 years, and 94 patients were above age 60. 414 patients survived (99.7% survival). Twenty-six patients required hospitalization (6.5%, 95% CI: 4.5% - 9.3%). All the hospitalized patients were unvaccinated. Other significant risk factors for hospitalization included age ≥ 60 years, hypertension, diabetes, late Fluvoxamine start (>4 days), and steroid use prior to presentation. Only thirteen patients required oxygen (3.1% 95% CI: 1.8% - 5.3%). Significant risk factors for oxygen requirement included age ≥ 60 years, male gender, and prior steroid usage. All the thirteen patients that required oxygenation were unvaccinated. The average length of hospital stay was 5.9 days. Conclusion: Early outpatient treatment with affordable, easily accessible repurposed drugs focusing on the pathophysiology of COVID-19 disease progression shows promising results vs. the standard of care by WHO, with only one death, 3.1% requiring oxygen, 6.5% hospitalizations, and an average hospital stay of 5.9 days in a developing country.
Introduction
In December 2019, even before mainstream media’s first reports of the events to come, Sharon Sanders, an online blogger from Florida, U.S.A. documented an unusual pattern of occurrences from clinic reports in Wuhan, China [1]. An infectious outbreak involving an unknown cause was occurring among patients presenting with three common factors: respiratory symptoms, hypoxia, and bilateral opacities on imaging, among others [2]. Slowly, the local and international mainstream media began raising suspicion of an epidemic caused by an agent yet to be determined at that time. Days later, both the Chinese Center for Disease Control and Prevention (CCDC) and the World Health Organization (WHO) jointly confirmed this suspicion and promised to continue informing the world of further developments [3, 4, 5].
Shortly after that, the world was introduced to a novel coronavirus, later identified as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-COV-2), the cause of Coronavirus Disease 2019 (COVID-19), the worst pandemic of this century [6]. Few would have predicted that this pandemic would create multiple and extreme points of view amongst physicians and scientists worldwide in regards the approach to combat this new evolving catastrophe. Unfortunately, this polarized positions still remain a huge area of debate around the globe.
From the beginning of this ongoing and devastating disease, there have been significant advancements in managing hospitalized patients with SARS-CoV-2. The RECOVERY Trial has conclusively proven that dexamethasone reduces the mortality of patients requiring oxygen [7]. Therapeutic anticoagulation also became a vital care component for critical hospitalized patients with SARS-CoV-2 given the now well-known COVID-19- associated coagulopathy [8]. Additionally, the combination of Interleukin-6 (IL-6) inhibitors, such as tocilizumab and sarilumab, with corticosteroids has been shown to further reduce the mortality rate in COVID-19 in critical patients [9, 10]. Unfortunately, advancements in COVID-19 disease management in the first 12 months were almost exclusive in the hospitalized patient with SARS-Cov-2 infection.
Nearing the end of 2021, most academicians and frontline physicians would agree that the course of the SARS-CoV-2 infection is anything but predictable. Thus, implementing a therapeutic approach early in the disease course becomes logical and essential to reducing COVID-19 related hospitalizations and mortality, making time a critical factor for COVID-19 management.
It became evident in the second year of the pandemic that early outpatient treatment was essential to anticipate the Covid 19 complications. However, the therapeutic way of approaching this, became divergent with a clear distinct between developed and underdeveloped countries. Most guidelines in the developed world are supporting the use of monoclonal antibodies or the recently approved Ritonavir/Nirmatrelvir therapies for patients at risk of clinical deterioration, but accessibility to these in developing countries is still a challenge. Although these are outstanding scientific achievements, the global disparity of vaccine distribution in underdeveloped region has already proven that these countries will not be able to prioritize these as viable therapeutic options. Low-income countries have been more proactive by utilizing more easily accessible medications, subsequently reporting success with early ambulatory management of SARS-CoV-2 infection [11]. Proponents of this method have predicted that early outpatient treatment with easily accessible, repurposed medications is a more practical approach for preventing COVID-19 related hospitalizations and complications, or at the very least lessening the course of illness.
Medications that may demonstrate a theoretical impact on the course of SARS-CoV-2 infection include Ivermectin, Colchicine, Aspirin, and Fluvoxamine. Ivermectin is a safe antiparasitic, with a wide spectrum of evidence throughout the world with very controversial data supporting or against its use when treating COVID-19 itself [12]. Colchicine works by acting on the NLRP3 inflammasome, and Aspirin is a well-known antiplatelet and anti-inflammatory agent [13, 14]. Interestingly, there is new evidence that serotonin acts as an essential molecule in COVID-19 pathology due to its effects on platelet adhesion [15]. The study presented herein demonstrates the outcomes of a multifaceted protocol utilizing repurposed, easily accessible medications for the early management of SARS-CoV-2 infection in the ambulatory setting of a developing country.
Definitions and Methods
Definitions of COVID 19 Severity
Mild Disease (COVID): Patients presenting with any of the common signs or symptoms of SARS-CoV-2 infection, including fever, cough, sore throat, malaise, headache, myalgias, nausea, vomiting, diarrhea, or loss of taste and smell, but do not have dyspnea, hypoxia, or abnormal chest radiography. Moderate Disease: Patients who show evidence of lower respiratory disease (e.g., dyspnea) at clinical presentation and/or abnormal chest radiography and who have pulse oximetry of ≥ 94% on room air. Severe Disease: Patients who show evidence of lower respiratory disease with pulse oximetry of < 94% on room air, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mmHg, a respiratory rate of >30 breaths per min, and/or abnormal chest radiography demonstrating > 50% pulmonary infiltrates. Critical Illness: Individuals presenting with respiratory failure, septic shock, and/or multiple organ dysfunction.
We conducted an observational cohort study, data was collected from medical records according to the Institutional Review Board (IRB) permission, from November 2020 until October 2021. This study was performed in the COVID-19 outpatient clinic at the Hospital Centro Médico Sanpedrano (CEMESA) in San Pedro Sula, Cortes, Honduras. The institutional review board approved the study as a minimal risk for the retrospective character of the study, and informed consent was not required. All patients fifteen years of age or older with mild or moderate signs and symptoms of COVID-19 with a positive SARS-COV-2 antigen or Reverse Transcription Polymerase Chain Reaction (RT-PCR) were included in the study. In addition, patients who developed signs and symptoms of the disease and were in close contact with one of the patients in the cohort were also treated and included in the study. Pregnant women, patients younger than fifteen years of age, and patients presenting with severe COVID-19 symptoms were excluded. A multidrug multifaceted treatment protocol was used according to the clinical presentation and days of symptoms of the disease.
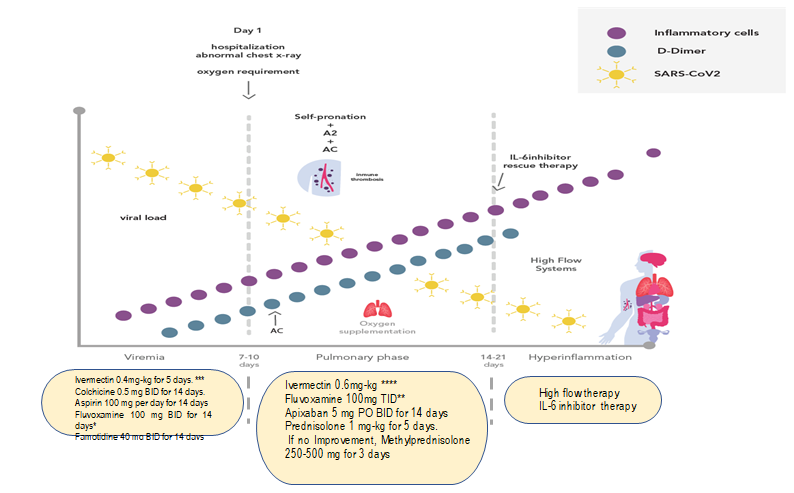
Viral Replication Phase treatment
Patients with less than seven days of disease onset in the viral replication phase with mild symptoms received the first phase (viral replication phase) of treatment, which consisted of Ivermectin 0.4 milligrams per kilogram (mg/kg) orally daily for five days, Aspirin 100 milligrams (mg) orally per day for fourteen days if no history of allergy, Colchicine 0.5 mg orally twice per day for fourteen days, Fluvoxamine 50 mg orally twice daily for three days, which, depending on patient tolerance, was increased to 100 mg orally twice daily to complete fourteen days, and Famotidine 40 mg orally twice daily for fourteen days.
Early Pulmonary Inflammatory Phase treatment
Patients were clinically evaluated on the eighth day following symptom onset or earlier for dyspnea, worsening cough, or a three percent reduction in oxygen saturation, measured by a home pulse oximeter. Chest computed tomography (CT) or chest radiograph and inflammatory markers, including complete blood counts (CBC), C-reactive protein (CRP), aspartate transaminase (AST), alanine transaminase (ALT), D-Dimer and lactate dehydrogenase (LDH), were obtained.
If the patient had clinical deterioration or had pulmonary infiltrates present on imaging studies and associated elevation of inflammatory markers, treatment with oral corticosteroids in association with oral anticoagulation was started even if they did not have oxygen desaturation considering they were developing an early pulmonary inflammatory phase. Prednisolone 1 mg/kg orally per day was used. All patients were reassessed after three days of using corticosteroids. If improving, a total five days of same treatment was completed followed by slow weaning of steroids (i.e fifty percent every three days).
If any inflammatory markers increased or clinical deterioration was present, which was defined as a progressive elevation of C-reactive protein, D-Dimer, or LDH, worsening dyspnea or oxygen saturation of less than 94% after three days of initiating oral corticosteroids, then intravenous (IV) methylprednisolone 250 mg per day for three days was administered, and oral prednisolone was discontinued. This was followed by a close daily clinical assessment at the COVID-19 clinic site to address whether the patient required hospital admission. If the patient’s clinical course and inflammatory markers improved, prednisolone was tapered down from a dose of 1 mg/kg per day with fifty percent reduction every three days. Apixaban 5 mg orally every twelve hours was given to patients who had elevated inflammatory markers or had worsening signs or symptoms and radiologic evidence of pulmonary disease progression by Chest CT or radiography.
If the patient had an oxygen saturation of less than 95%, then the dose of Ivermectin was escalated from 0.4 mg/kg to 0.6 mg/kg orally per day for five days. Additionally, the frequency of Fluvoxamine 100 mg was escalated from every twelve hours to every eight hours. If patients presented after day seven of the onset of symptoms and had clinical and radiologic evidence of pulmonary disease, they were treated with the viral replication phase medication as well as prednisolone and oral anticoagulation.
Statistical Analysis
Descriptive analysis was performed to find the average and median values for quantitative analysis. Univariate analysis using Chi-square analysis was performed on the categorical variables to establish the risk association. SPSS Version 26 was used for statistical analysis (Figure 1).
Results
A total of 415 patients participated in the study. 208 were men (50.1%) and 207 were women (49.9%). The average age was 47.4 years (46.8 in men and 47.9 in women, p = 0.5). Only 94 patients (22.6%) were older adults i.e age ≥60 years. 158 (38.1%) were overweight (BMI 25.0 – 29.9 kg/m2), and 117 (28.2%) patients were obese (BMI ≥30 kg/m2). Ninety- eight (23.6%) patients had hypertension. Forty-seven (11.3%) were diabetic, and twenty-four (5.8%) patients had hyperlipidemia. Bronchial asthma and hypothyroidism were seen in sixteen (3.9%) patients each. Eleven (2.7%) had psychiatric illnesses. A total of 176 (47.8%) had at least one of the comorbidities.
Out of 415, only 100 people were adequately vaccinated, whether they had two doses or a single dose (Johnson and Johnson), and at least 14 days had elapsed since the last dose. All 415 patients received Fluvoxamine and ivermectin. Aspirin was given to 379 patients. 375 received Famotidine, and 388 received colchicine. Only 191 were prescribed Apixaban and 186 received steroids. Only five patients required Tocilizumab (1.2%, 95% CI: 0.5% - 2.8%). Ninety- three patients (22.4%) had received premedication before presenting to the study clinic. Only eleven patients had prior documented steroid usage.
Of the 415 patients, 414 survived (99.7% survival). Only one patient died. She was a 50-year-old unvaccinated female with class I Obesity, who was self-medicating with prednisolone 50 mg/day and Azithromycin 500 mg/day since day one of symptom onset. She presented on the fifth day of symptoms. Upon evaluation, she was classified as moderate disease needing supplemental oxygen and was hospitalized.
Of 415 patients, twenty-six patients required hospitalization (6.5%, 95% CI: 4.5% - 9.3%). All of the hospitalized patients were unvaccinated. Other significant risk factors for hospitalization included age ≥ 60 years (RR = 2.6, 95% CI: 1.2-5.4, p = 0.009), hypertension (RR = 2.1, 95% CI: 1.0-4.5, p = 0.003), Diabetes Mellitus type 2 (RR = 2.9, 95% CI: 1.3-6.8, p = 0.01), late Fluvoxamine start (>4 days) (RR = 2.8, 95% CI: 1.2-6.9, p = 0.007), and steroid use in the early viral replication phase (RR = 5.1, 95% CI: 1.9-13.5, p = 0.01).
The average length of hospital stay (LOS) was 5.9 days (P25 4.0, P50 5.5, P75 7.7). Only thirteen patients required oxygen (3.1% 95% CI: 1.8% - 5.3%). Significant risk factors for oxygen requirement included age ≥ 60 years (RR = 3.5, 95% CI: 1.2-10.1, p = 0.01), male gender (RR = 3.2, 95% CI: 0.9-11.4, p = 0.03), and use of steroids in the early replication phase (RR = 7.3, 95% CI: 1.9-28.2, p = 0.02). All of the thirteen patients that required oxygenation were unvaccinated.
Discussion
History will remember the COVID-19 pandemic for multiple reasons, but the most striking will likely be the conflict and diversity of opinions in all areas of modern society. Among scientists, academicians, and frontline healthcare providers, there has been an unrelenting debate revolving around whether to wait for the evidence provided by randomized controlled trials before proceeding with a therapeutic strategy or utilizing the best available evidence at present to develop a targeted therapeutic approach. This was exemplified by the early debate over the responsiveness of SARS-CoV-2 to corticosteroids, as six months went by before a randomized controlled trial answered this critical question. However, many frontline healthcare providers were already implementing corticosteroids into their therapeutic approach for SARS-CoV-2 infection despite enduring criticism. Underdeveloped countries, like Honduras, did not have the luxury of awaiting the results of randomized controlled studies because of the potential for collapse of their healthcare system without developing a treatment strategy. In contrast to New York City, which has a population of 8.9 million, 1060 critical care physicians, and 1644 intensive care unit (ICU) beds, Honduras has only nineteen critical care physicians and 125 ICU beds for a population of 9.9 million [16, 17]. This has led to the need to develop a multifaceted therapeutic approach utilizing repurposed medications that are more readily accessible to underdeveloped countries like Honduras.
Early in the COVID-19 pandemic, there was considerable controversy and debate at all levels of government, and the medical community, regarding how to mitigate the impact of this rapidly progressing coronavirus infection. Logically, medical authorities looked to past experiences with the epidemics caused by Severe Acute Respiratory Syndrome Coronavirus 1 (SARS-CoV-1) and Middle East Respiratory Syndrome Coronavirus (MERS-CoV). These epidemics were approached with large-scale quarantines of infected patients and close contacts alike in all settings, including healthcare. Because this seemed to be an effective strategy, this approach was utilized in the initial phases of SARS-CoV-2 infection, with isolation of ill patients followed by contact tracing, progressing to closures, even with fervent debate, of large sectors of the populace. However, it has now become clear that this was not an effective means of control, given a better understanding of the pathogenesis of SARS-CoV-2 compared to SARS-CoV-1 and MERS-CoV. When discussing SARS-CoV-1, MERS-CoV, and SARS-CoV-2, one cannot assume that they can each be managed similarly, simply because they are categorized as coronaviruses. With SARS-CoV-1 and MERS- CoV, infected patients develop symptoms before the peak of viral load.
Therefore, there are no asymptomatic carriers, which is why patient and contact isolation is effective. There was no indication for the development of an early outpatient treatment approach to slow transmission because symptomatic patients were placed in isolation early in the disease process. This is in direct contrast to SARS-CoV-2. In their study, Benefield A, et al. [18] clearly demonstrated that the SARS-CoV-2 viral load peaks before symptom onset and remains elevated for approximately twenty days [18]. This allows for asymptomatic persons to propagate SARS-CoV-2 early on, before progression to more severe, complicated illness, even as viral load declines. Thus, along with aggressive testing, an early aggressive outpatient therapeutic approach becomes of the utmost importance to mitigating the impact of SARS-CoV-2.
Since January 2020, there has been a plethora of emerging evidence by scientists worldwide regarding the pathophysiology of SARS-CoV-2 infection. A consensus exists that there is an initial viral stage whereby symptoms may vary from a minimal to a mild undifferentiated viral syndrome in some, which may progress in others to a pulmonary phase with hypoxia and associated organizing pneumonia. COVID-19 is multi-systemic, most of the time, and follows the pattern of Angiotensin-Converting Enzyme 2 (ACE) receptors in various body organ systems, including the cardiovascular, renal, and gastrointestinal systems [19]. There is also a significant body of evidence that the timing of interferon release plays a crucial role in the severe inflammatory phase. The dysfunction caused by SARS- CoV-2 promotes a vigorous activation of the nucleotide- binding oligomerization domain, Leucine-rich repeat and Pyrin domain-containing protein 3 (NLRP3) inflammasome, caspase, interleukin-1 (IL-1) and interleukin-6 (IL-6) pathways [20]. Another point of convergence among experts is the fact that COVID-19 causes endothelitis. This gives rise to an unregulated prothrombotic state that ultimately leads to endothelial cell dysfunction, dysregulation of angiotensin II, and a vicious pro-inflammatory state leading to unabated immune thrombosis. In addition, immobilization, hypoxia and disseminated intravascular coagulation can increase the prothrombotic state of these patients. It has been speculated that microvascular thrombosis may play a critical role in hypoxemia and multiorgan failure [21, 22].
Another important pathway in COVID-19 pathogenesis is excessive platelet activation. An excess of free plasma serotonin derived from platelets leads to excessive platelet- fibrin aggregation and the formation of microthrombi [23]. Fluvoxamine, a medication classified as a selective serotonin reuptake inhibitor (SSRI), has been shown to play a significant role in modulating this pathway through agonistic activity on the sigma 1 receptor. This, in turn, mediates inflammation, potentiates an antiplatelet effect, and reduces mast cell degranulation and cytokine storm, among other actions specific to the pathophysiology of SARS- CoV-2 infection. Further, Aspirin, a well-known antiplatelet agent, also plays a role in limiting SARS-CoV-2 pathogenesis through inhibition of the Cyclooxygenase-1 (COX-1) pathway, leading to a decrease in Thromboxane-A2 (TX-A2), subsequently decreasing platelet aggregation [24]. Evidence from autopsies and bronchoscopy samples shows a clear macrophage activation syndrome that perpetuates all the above pathways. With all this knowledge acquired since the first days of the COVID-19 pandemic, it would be logical to anticipate the activation of all these pathologic pathways and attempt to effectively intervene with a targeted therapeutic approach early in the disease course rather than later.
Colchicine is an anti-inflammatory medication that has been available for centuries and the mechanism of action interferes with microtubules auto formation within the cytoplasm of cells. It is thought to interfere with these inflammatory pathways through microtubule inhibition and inhibiting the neutrophil recruitment and adhesion in the site of inflammation. It interferes with the proinflammatory protein complex, the nod-like receptor protein 3 (NLRP3) inflammasome, which produces inflammatory pathways and enzymes such as caspase-1 which are responsible for activating interleukin 1Beta, that induce macrophages to release large quantities of additional pro-inflammatory cytokines, one of them being IL-6, a cytokine that induces C-reactive protein that has been deeply associated as an important proinflammatory component of the cytokine storm that is characteristic in COVID-19 patients. The concentration of colchicine in inflammatory cells such as leukocytes is very high, its concentrated about 16 times more than in serum, hence the importance of anti-inflammatory properties in the entire COVID-19 pathophysiology [25]. New released evidence states that these pathways need to be blocked very early on the disease course [26]. A recent review by Kory P, et al. [27] shows that Ivermectin has antiviral properties against an increasing number of RNA viruses including SARS-COV2. Its mechanism of action in the disease to name a few, is due to the high binding activity of the medication to the spike protein on SARS-COV2, which makes it harder for the virus to bind to the ACE2 receptors located all around the body and therefore a decrease on viral cellular entry. It is also noticeable that Ivermectin inhibits viral replication by binding and blocking the RNA-dependent RNA polymerase. For a more detailed review we invite the reader to see the excellent manuscript of Kory P, et al. [27]
A recent metanalysis by Bryant et al showed that using Ivermectin early in the clinical course may reduce numbers progressing to severe disease having a significant impact on the SARS-CoV2 pandemic [28].
A multi-mechanistic and stepwise approach in the outpatient setting, which is initiated early in the disease course and has been geared toward these pathogenic pathways, is not only logical but scientifically founded. Recently, Valerio Pascua FV et al. [29] proposed a multi- mechanistic approach for the management of hospitalized patients with COVID-19, which has since been adopted by many countries with very minimal differences in implementation. This treatment approach consists of high- dose corticosteroids, preferentially methylprednisolone, tocilizumab as a rescue agent, high-intensity, or therapeutic anticoagulation, Ivermectin, high-flow oxygen systems, and self-proning, if possible, to improve oxygenation [29]. An early outpatient treatment based on clear pathophysiologic states of the disease is an extension of these principles. The basis for this clinical study is to apply these principles and investigate their impact on the course of COVID-19 in an outpatient clinic in Honduras, utilizing readily available repurposed medications.
Limitations
Vaccination has been the first globally accepted pharmaceutical contingency measure for the COVID-19 pandemic and it has become within reach for underdeveloped countries, including Honduras. The massive vaccination campaign programs promoted by the WHO may impact the severity of some cases in this research. Some patients were fully vaccinated, while others had only one dose, affecting the study outcome. The lack of ethnic diversity, the absence of a control group, and the fact that this study was conducted in a single hospital during the COVID-19 pandemic are all limiting factors with respect to the study outcomes. However, the lack of significant research performed on this topic makes this study a strong starting point for further investigations. Also, it has been so deeply rooted in the population to stay at home and not search for an early treatment that some cases that were not in an early stage were included, limiting the study outcomes. However, it was a small percentage of the whole population in the study. Despite all these limitations there’s a counterbalance when applying this protocol accessibility in an underdeveloped nation like the one doing the study. The pandemic has proven to the world that there have been disparities in the distribution of novel therapies directed to SarsCov2, in the vaccines and monoclonal antibodies. When the manuscript was being written two new antivirals were released: molnupiravir and ritonavir/nirmatrelvir in the United States for early outpatient treatment [30]. Given our prior experiences in the distribution of new therapies, it would be naïve to believe that Honduras will be a priority to these two big pharmaceutical companies producing these products.
Confounding Factors
Individual Socioeconomic Status
This study was conducted at a private hospital. Therefore, due to specific social considerations, some patients were admitted despite not meeting the criteria. As a result of this, the rate of hospitalizations increased by a small percentage. We don’t think that this will play a role in mortality rate and length of hospital stay since patients were treated under the same circumstances and same criteria were used per our protocol in the entire cohort, not being influenced by their socioeconomic status. All patients that were admitted and treated in our study were able to afford a private health setting which gave us the opportunity to use the same resources in all our patients.
Number of Comorbidities
Another confounding factor is the comorbidities in the patient group, among these comorbidities were: obesity, hypertension, diabetes, bronchial asthma, hypothyroidism, hyperlipidemia, and psychiatric illnesses which may have contributed to the increase of length of stay and mortality in some patients. Also is very important to clarify that the comorbidities needed to be seen in every patient individually, because the outcomes of every patient could also be determined if those comorbidities were under control or not.
Hospital Care Quality
The hospital care quality was the same in the entire patients under the study, since they were treated just in one hospital which was private, with the same conditions for all of them. We will consider that this confounding will play a role on our results if we were comparing patients between a private and public hospital, since the care quality can sometimes be diminished in a public hospital setting because there are less resources available for healthcare workers and even for the patients itself. Our entire cohort were under the same circumstances regarding hospital care quality which would not affect the mortality and hospitalizations rate, nor the length of hospital stay.
Social and Economic Impact
When repurposed drugs for the treatment of COVID-19 are referenced herein, it is innovative and beneficial for patients overall and essential for managing the disease within developing countries, such as Honduras. In addition, by using a redirected drug, Fluvoxamine, this study presents a proposal for a low-cost option that is within financial reach for a large portion of a developing society, within which many live in extreme poverty. Therefore, the evidence presented in this study will have both an economic and social impact on the management of ambulatory patients with COVID-19.
Conclusion
The study provided an undeniable insight into the concept of early outpatient treatment in COVID-19 disease in a cohort of unvaccinated, partially, and fully vaccinated patients within a country with such limited resources as Honduras. This regimen focused on an early multi-mechanism approach to better understand the pathophysiology and phases of this viral infection. Emphasizing the use of affordable, easily accessible repurposed drugs for COVID-19 decreased critical epidemiological markers like hospitalization, oxygen need, mean hospital stay, and death, which are fundamentally crucial in the COVID-19 puzzle. Despite the study’s limitations, it proves that the intention of treatment is lifesaving. These findings merit further investigation in a comparative, multi- institutional study to reinforce/replicate its results.
Acknowledgments
We wish to thank Mrs. Waleska Solis-Hoffman, Mr. Edgardo Melgar and Mr. Daniel Antonio Fortin and Ing. Robert Maas Chavez for their altruism during the pandemic in Honduras, the success and outcome of this study required their voluntarily constant dedication and hard work.
References
-
Farhi P (2020) How a blogger in Florida put on an early warning about the coronavirus crisis. The Washington Post.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet 395(10223): 497-506.
-
Zhang Y, Chen C, Zhu S, Shu C, Wang D, et al. (2020) Isolation of 2019-ncov from a stool specimen of a laboratory-confirmed case of the coronavirus disease 2019 (covid-19). China CDC Weekly 2020 2(8): 123-124.
-
(2020) Pnuemonia of unkown cause-China. World Health Organization.
-
(2019) Coronavirus disease (covid-19) - events as they happen. World Health Organization.
-
(2021) Statistics Say Large Pandemics Are More Likely Than We Thought. Duke Global Health Institute.
-
Horby P, Landray MJ, Haynes R, Bailie K, Juszczak E, et al. (2021) Dexamethasone in hospitalized patients with covid-19. N Eng J Med 384(8): 693-704.
-
Ackermann M, Verleden SE, Kuehnel M, Haverich A, Welte T, et al. (2020) Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N Eng J Med 383(2): 120-128.
-
Del Pozo JSG, Galindo MF, Nava E, Jordán J (2020) A systematic review on the efficacy and safety of IL-6 modulatory drugs in the treatment of COVID-19 patients. Eur Rev Med Pharmacol Sci 24(13): 7475-7484.
-
Nasonov E, Samsonov M (2020) The role of Interleukin 6 inhibitors in therapy of severe COVID-19. Biomed Pharmacother 131: 110698.
-
Ontai S, Zeng L, Choi D, Hoffman MS, Valerio Pascua F, VanBuren V, et al. (2022) Early Multidrug Treatment of SARS-Cov-2 (COVID-19) and Decreased Case Fatality Rates in Honduras. Epidemol Int J 6(1): 00217.
-
Chaccour C, Casellas A, Di Matteo AB, Pineda I, Montero AF, et al. (2021) The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. EClinicalMedicine 32: 100720.
-
Reyes AZ, Hu K, Teperman J, Wampler Muskardin TL, Tardif JC, et al. (2021) Anti-inflammatory therapy for COVID-19 infection: the case for colchicine. Ann Rheum Dis 80(5): 550-557.
-
Awtry EH, Loscalzo J (2000) Aspirin. Circulation 101(10): 1206-1218.
-
Hamed MG, Hagag RS (2020) The possible immunoregulatory and anti-inflammatory effects of selective serotonin reuptake inhibitors in coronavirus disease patients. Medical Hypotheses 144: 110140.
-
United Nations (2019) World Population Prospects- Population Division. Department of Economic and Social Affairs.
-
Choi A, Bhat S, Velasquez J, Welch W (2022) Coronavirusin New York City. The City.
-
Benefield A, Skrip A, Clement A, Althouse R, Chang S, et al. (2020) SARS-CoV-2 viral load peaks prior to symptom onset: a systematic review and individual-pooled analysis of coronavirus viral load from 66 studies. MedRxiv.
-
Zhang X, Li S, Niu S (2020) ACE2 and COVID-19 and the resulting ARDS. Postgrad Med J 96(1137): 403-407.
-
Rodrigues T, de Sá K, Ishimoto A, Becerra A, Oliviera S, et al. (2020) Inflammasomes are activated in response to SARS-CoV-2 infection and are associated with COVID-19 severity in patients. J Exp Med 218(3): e20201707.
-
Ackermann M, Verleden SE, Kuehnel M, Haverich A, Welte T, et al. (2020) Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in covid-19. N Eng J Med 383(2): 120-128.
-
Liu P, Blet A, Smyth D, Hongliang L (2020) The Science Underlying COVID-19 Implications for the Cardiovascular System. Circulation 142(1): 68-78.
-
Zaid Y, Puhm F, Allaeys I, Naya A, Oudghiri M, et al. (2020) Platelets can associate with SARS-COV-2 RNA and are hyperactivated in COVID-19. Cir Res 127(11): 1404-1418.
-
Sukhatme VP, Reiersen AM, Vayttaden SJ, Sukhatme VV (2021) Fluvoxamine: A Review of Its Mechanism of Action and Its Rolein COVID-19. Front. Pharmacol 12: 652688.
-
Leung Y, Li Yao L, Kraus V (2015) Colchicine-Update on mechanisms of action and therapeutic uses. Semin Arthritis Rheum 45(3): 341-350.
-
Vora S, Lieberman J, Wu H (2021) Inflammasome activation at the crux of severe COVID-19. Nature 21: 694-703.
-
Kory P, Meduri G, Varon J, Iglesias J, Marik P (2021) Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of Covid-19. Am J Ther 28(3): e300-e318.
-
Bryant A, Lawrie TA, Dowswell T, Fordham EJ, MitchellS, et al. (2021) Ivermectin for Prevention and Treatmentof COVID-19 Infection: A Systematic Review, Metanalysis, and Trial Sequential Anlaysis to Inform Clinical Guidelines. Am J Ther 28(4): e434-e460.
-
Pascua FV, Diaz O, Medina R, Contreras B, Mistroff J, et al. (2021) A multi-mechanism approach reduces length of stay in the ICU for severe COVID-19 patients. PloS One 16(1): e0245025.
-
Hotez P, Batista C, Amor YB, Ergonul O, Figueroa J, et al. (2021) Global public health security and justice for vaccines and therapeutics in the COVID-19 pandemic. EClinicalMedicine 39: 101053.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria