Assessment of Employee Health Program at Ministry of Health Hospitals in Saudi Arabia
Background: Due to lack of formal employee health services in ministry of health- Saudi Arabia and high exposure risk of health care workers. So it was a necessity to establish a comprehensive medical program to track occupational diseases, injuries and work place exposures.Methods: Assessment of employee health program in all MOH hospitals was carried out from January to march 2017 using survey prepared and circulated via email to staff responsible for employee clinics of all facilities at all health regions and governorates of Saudi Arabia that joined Ministry Of Health-Saudi Arabia's employee health program since its implementation in 2012.Results: Highest percent of employee health clinics was established in hospitals with a bed capacity ≥400 beds. Eighty percent of the clinics are fully supervised by infection control department, 81.3 % have one or more full time staff working in it, 91% have employee medical records either in hard or soft forms and 77.6 % have available equipment and materials necessary for the clinic duties. Services' coverage provided by employee health clinics as coverage of N95 Fit – Test , Post exposure Prophylaxis Medications, Availability of Reporting system (100 & 90 & 70 percent respectively ) with improvement of services with increased bed capacity.Conclusion: Improvement of employee health services is noticed in hospitals that implement the employee health program as employee health clinics was established in 58% of hospitals , Eighty percent of the clinics are fully supervised by infection control department, most of hospitals have one or more full time staff manage the clinics. Availability of Post exposure Prophylaxis Medications, Reporting system, and Mandatory Vaccination Supply was made available to all MOH' employee clinics especially hepatitis B vaccinations, influenza vaccinations, and meningitis. Recommendations: Expanding the employee health program to all Ministry of health' health care facilities and even the private sectors, Integration of services at different level to provide all essential vaccines mandated by international agencies to protect the health care workers, Generalization of electronic system for generating employee medical records, Recruitment of more staff to manage the employee health program.
Hail M Abdaley1, Ahmed M Hakawi2, Mervat M Eldalatony3* and Hanan M Hathout4
Saudi Arabia
Arabia
Arabia
Arabia
+966-598983409; Email: mervat.moh.abd@gmail.com
injuries and work place exposures.
its implementation in 2012.
improvement of services with increased bed capacity.
Conclusion: Improvement of employee health services is noticed in hospitals that implement the employee health program as employee health clinics was established in 58% of hospitals , Eighty percent of the clinics are fully supervised by infection control department, most of hospitals have one or more full time staff manage the clinics. Availability of Post exposure Prophylaxis Medications, Reporting system, and Mandatory Vaccination Supply was made available to all MOH' employee clinics especially hepatitis B vaccinations, influenza vaccinations, and meningitis.
Recommendations: Expanding the employee health program to all Ministry of health' health care facilities and even the private sectors, Integration of services at different level to provide all essential vaccines mandated by international agencies to protect the health care workers, Generalization of electronic system for generating employee medical records, Recruitment of more staff to manage the employee health program.
Keywords: Bloodborne; Pathogen infections; Post exposure; Varicella
Introduction
Occupational Health is the promotion and maintenance of the highest degree of physical, mental and social well- being of workers in all occupations by preventing departures from health, controlling risks and the adaptation of work to people, and people to their jobs [1]. The broad definition of occupational health was then accepted and has been later referred to: “occupational health should not only include occupational diseases and accidents but all health aspects of man at work, the adjustment of work to man and of each man to his or her job” [2]. Exposure prevention remains the primary strategy for reducing occupational bloodborne pathogen infections; however, occupational exposures will continue to occur. Health-care organizations should make available written protocols for prompt reporting, evaluation, counseling, treatment, and follow-up of occupational exposures that might place HCP at risk for acquiring a bloodborne infection [3]. Employers are required to establish exposure-control plans that include post exposure follow-up for their employees and to comply with incident reporting requirements mandated by OSHA [4]. Access to clinicians who can provide post exposure care should be available during all working hours, including nights and weekends. HBIG, hepatitis B vaccine, and antiretroviral agents for HIV PEP should be available for timely administration (i.e., either by providing access Mervat M Eldalatony, et al. The University Desk Chair: Examining the Impact on Student Comfort and Ability to Focus. Ergonomics Int J 2018, 2(2): 000140.
on-site or by creating linkages with other facilities or providers to make them available off-site). Persons responsible for providing post exposure management should be familiar with evaluation and treatment protocols and the facility's plans for accessing HBIG, hepatitis B vaccine, and antiretroviral drugs for HIV PEP [3]. Employee health services in the health care facilities of kingdom of Saudi Arabia was in the form of primitive informal services conducted to health care workers in the form of :- supplying vaccination (HBV vaccine, influenza and meningitis vaccine) a duty that was carried out mainly by infection control personnel in the facility, and providing sick leave permissions to healthcare workers by staff clinic ( if present), There was no reporting of occupational accidents as exposure to needle stick or sharp object and blood and body fluid incidents, and no post exposure management and follow up was provided. Employee health program is required to make sure of the well-being of all healthcare workers in the institution and protect patients of contracting communicable infections transmitted by the healthcare workers. Ministry of Health Executive Board - Saudi Arabia (2013) approved the establishment of the employee health program in ministry of health' hospitals to provide a good healthcare service to healthcare workers. The program was built up and managed by the General Directorate of Infection Prevention & Control- Ministry Of Health-Saudi Arabia (GDIPC-MOH-KSA).
Objective
Assessment of Employee Health Program in Ministry of Health related healthcare facilities after 4 years of program implementation.
Methodology
- Physical construction of the clinic
- No. of full-time staff
- Available Employee Medical Records (hard or soft forms)
- Equipment & materials availability
- Evaluation of services (N95 fit testing, Availability of Post exposure Prophylaxis (HB immunoglobulin-Anti HIV medications-chicken pox immunoglobulin, Availability of Mandatory Vaccination Supply (HB vaccine,
- Influenza vaccine, Varicella (chickenpox), DTaP, MMR, Meningitis vaccines.
- Availability of Incidents Reporting system The form was filled out by the employee health program coordinators in the regions / governorates, Data fed back to the program owner from 18 regions all over the kingdom. Analysis: The hospital categorized into: hospitals <200 bed, 200-400 bed and, > 400 bed according to their bed capacity. Collected data were analyzed using SPSS program version 21 and results displayed in the form of number and percent as following:
- Results
- Hospitals <200 beds (Total =
- 169)
- Hospitals 200-400 beds (Total = 35)
- Hospitals ≥ 400 beds (Total = 25)
- = 229)
- No. of EHC
- %
- No. of EHC
- %
- No. of EHC
- %
- No. of EHC
- %
- 91
- 53.8
- 23
- 65.7
- 20
- 80
- 134
- 58.5
Table 1: Distribution of employee health clinics in the health regions sharing in the survey according to categories of

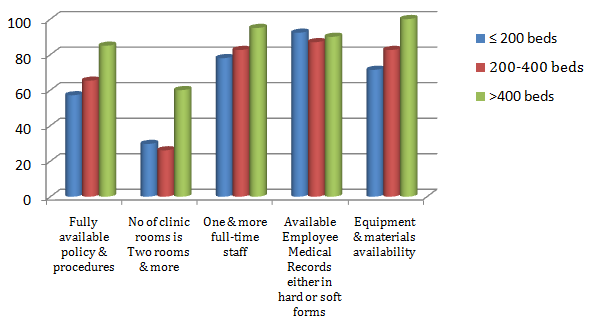
Highest percent of employee health clinics was established in hospitals with a bed capacity ≥400 beds (Table 1). Eighty percent of the clinics are fully supervised by infection control department, 81.3 % have one or more full time staff working in it, 91% have employee medical records either in hard or soft forms and 77.6 % have available equipment and materials necessary for the clinic duties (Figure 1). Table 2 shows percent of services' coverage provided Mervat M Eldalatony, et al. The University Desk Chair: Examining the Impact on Student Comfort and Ability to Focus. Ergonomics Int J 2018, 2(2): 000140.
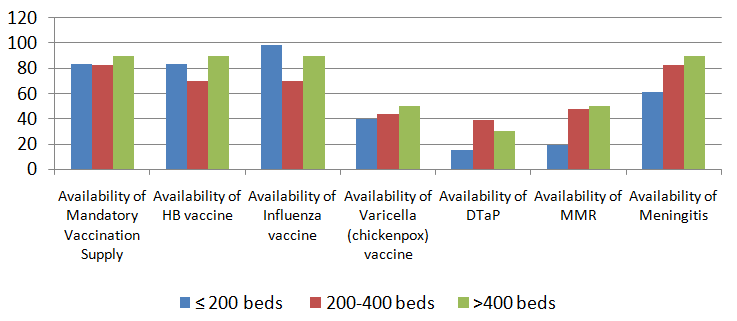
by employee health clinics as coverage of N95 Fit – Test (> 75% coverage rate), Availability of Post exposure Prophylaxis Medications, Availability of Reporting system as follow 100 & 90& 70 percent respectively with improvement of services with increased bed capacity. Figure 2 Available vaccinations provided to employee health clinics are mainly hepatitis B vaccinations, influenza , and meningitis vaccine (82.1&92.5&69.4 percent) respectively with low availability of Varicella, DTaP, and MMR vaccine (41.8&21.6&28.4percent)respectively.
| Hospitals <200 beds (Total = 169) | Hospitals 200-400 beds (Total = 35) | Hospitals ≥ 400 beds (Total = 25) | Total Hospitals (Total = 229) | |||||
|---|---|---|---|---|---|---|---|---|
| No | % | No | % | No | % | No | % | |
| Coverage of N95 Fit – Test (> 75% coverage rate) | 35 | 38.5 | 15 | 65.2 | 17 | 85 | 134 | 100 |
| Availability of Post exposure Prophylaxis Medications (HB immunoglobulin-Anti HIV medications-chicken pox immunoglobulin) | 82 | 90.1 | 21 | 91.3 | 18 | 90 | 121 | 90.3 |
| Availability of Reporting system | 59 | 64.8 | 19 | 82.6 | 16 | 80 | 94 | 70.1 |
Table 2: Data representing some services available to healthcare workers according to categories of hospital bed capacity.
Mervat M Eldalatony, et al. The University Desk Chair: Examining the Impact on Student Comfort and Ability to Focus. Ergonomics Int J 2018, 2(2): 000140.
Discussion
Due to lack of formal employee health services in ministry of health- Saudi Arabia and high exposure risk of health care workers. so it was a necessity to establish a comprehensive medical program to track occupational diseases, injuries and workplace exposures ,provide mandatory vaccination without charge to employees at multiple convenient sites and times, providing post exposure medications, establishment of reporting system for staff exposure and keeping the medical record for health care workers. According to U.S. Public Health Service [3] all institutions in which health care personnel might experience exposures should have a written policy for management of exposures. So, In May 2013 a comprehensive policy & procedures was established by the employee health team of GDIPC-MOH-KSA containing all requirements for establishment of employee health clinic in all health care facilities. The policy also includes the duties of the employee health clinic as pre- employment screening, employee vaccination according to international standards, periodic medical examinations (and follow-up examinations when appropriate), post exposure prophylaxis, --etc). In addition, intensive training courses were implemented to prepare qualified staff to be responsible for duties of the clinics. Provision of exposure management services requires infrastructure and manpower to support infection control and occupational health activities [5]. The highest percent of employee health clinics in this study was established in hospitals with a bed capacity ≥400 beds which may be explained in part by perception of the importance of employee health program due to high number of staff and high workload which subject staff to high risk of exposures to occupational hazards (Table1). Available resources as infrastructure in form of equipment and materials in hospitals ≥400 beds (100%) compared to 71%& 82% in hospital categories ≤ 200& 200- 400 respectively, also available staff to implement the policy and procedures of the program in hospitals ≥400 beds is 95 percent of employee clinics have one or more full time staff compared to 78%& 82% in hospital categories ≤ 200 & 200- 400 respectively (Figure 1). N95 fit testing was one of the main tasks of employee health clinics and is obligatory to all health care workers at high risk of exposure to air borne infections to be repeated annually as per CDC recommendations.
Mervat M Eldalatony, et al. The University Desk Chair: Examining the Impact on Student Comfort and Ability to Focus. Ergonomics Int J 2018, 2(2): 000140.
Employee clinics were equipped with all necessary requirements for N95 fit testing including kits, different models and sizes of N95 respirators, in addition to Powered Air Purifying Respirators (PAPR) for unfit and beard health care workers, intensive training courses of clinic' staff was also implemented as a part of MOH efforts to fight newly emerging infectious diseases especially Middle East respiratory syndrome corona virus (MERS- CoV) that was a great challenge in KSA since 2012. Coverage of N95 test is steadily increasing with increased hospital bed capacity (38% & 65%& 85%) in hospitals> 200 & 200- 400&>400 beds respectively which reflects insistence of the MOH to provide highest level of protection to health care workers ( Table 2). Post exposure medications become accessible at the employee clinics for all exposed staff in 90% of employee clinics to provide timely management (Table 2). Vaccination of health care workers reduces employee illness and absenteeism (6) in nursing home settings, vaccination of health care workers has been shown to decrease morbidity and mortality among nursing home residents [7]. Furthermore, staff vaccination programs are cost-effective for health care institutions because of reduced staff illness and absenteeism [8]. Mandatory Vaccination Supply including (HB vaccine, Influenza vaccine, Varicella (chickenpox) vaccine, DTaP, MMR and Meningitis vaccine) was made available to all MOH' employee clinics especially hepatitis B vaccinations, influenza vaccinations, and meningitis (Figure 2). Health care facilities should establish exposure- reporting systems [3] Ministry of Health mandates the establishment of a reporting system for occupational exposures to workplace hazards specially those related to blood borne pathogens through needle stick and sharp objects injury and exposure to blood and other body fluid. Accordingly 70% of MOH’ hospitals (Table 2) Now already have reporting systems of infectious diseases. And a unified electronic system of exposure prevention information network (EpiNet)
Conclusion
Improvement of employee health services is noticed in hospitals that implement the employee health program as employee health clinics was established in 58% of hospitals , Eighty percent of the clinics are fully supervised by infection control department, most of hospitals have one or more full time staff manage the clinics. Availability of Post exposure Prophylaxis Medications, Reporting system, and Mandatory Vaccination Supply was made available to all MOH' employee clinics especially hepatitis B vaccinations, influenza vaccinations, and meningitis.
Recommendations
• Expanding the employee health program to all Ministry
of health' health care facilities and even the private sectors.
- Integration of services at different level to provide all essential vaccines mandated by international agencies to protect the health care workers.
- Generalization of electronic system for generating employee medical records.
- Recruitment of more staff to manage the employee health program.
References
-
World Health Organization (1995) Global strategy on occupational health for all”. Recommendations of Second Meeting of the WHO Collaborating Centers in Occupational Health. Document WHO/OCH/95.2. Geneva.
-
Jerzy a Kopias (2001) Multidisciplinary model of occupational health services. Medical and non- Mervat M Eldalatony, et al. The University Desk Chair: Examining the Impact on Student Comfort and Ability to Focus. Ergonomics Int J 2018, 2(2): 000140. medical aspects of occupational health. International Journal of Occupational Medicine and Environmental Health 14(1): 23-28.
-
U.S. Public Health Service (2001) “Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for post exposure prophylaxis. MMWR Recommendations Rep 50(RR-11): 1-52.
-
Occupational Safety and Health Administration (OSHA) 1995:“OSHA’s Bloodborne Pathogens Standard”. Occupational Safety. www.osha.gov 1-800- 321-6742
-
Mbaeyi C, Adelisa L. Panlilio, Cynthia Hobbs, Priti R. Patel, David T Kuhar (2012) Assessment of Management Policies and Practices for Occupational Exposure to Bloodborne Pathogens in Dialysis Facilities. Am J Kidney Dis 60(4): 617-625
-
Salgado C, Farr B, Hall K, Hayden F (2002) Influenza in the acute hospital setting. Lancet Infect Dis 2(3): 145-155.
-
Hilary M, Nancy G, Marilyn J, Claiborne D, Keith F (2010) Mandatory Influenza Vaccination of Health Care Workers: Translating Policy to Practice. Clinical Infectious Diseases 50(4): 459-464
-
Olga A, Annette B, and Wendy R (2009) Requiring Influenza Vaccination for Health Care Workers. Am J Public Health 99(1): 24-29.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30