Why is the Implementation of Crew Resource Management through Checklists in Healthcare not Systematically Successful? An Answer from Cognitive Systems Engineering
Medical checklists come from researches on Crew Resource Management originally performed in the aviation domain. Despite significant benefits brought by checklists, difficulties have appeared in practice through the emergence of individual resistance, passive non-compliance, or partial application of instructions. Our hypothesis is that the medical field differs significantly from the aviation field. Contrary to the aviation field, healthcare systems are loosely coupled systems in which standardization of practices with checklists can be inappropriate. Through cognitive work analysis, Cognitive Systems Engineering can provide alternative methodological frameworks to consider this issue.
Introduction
It is commonly asserted that the birth of crew resource management (CRM) occurred during a workshop organized by NASA in 1979 [1]. In the first paper, Lauber argued that “one of the principal causes of incidents and accidents in civil jet transport operations is the lack of effective management of available resources by the flight-deck crew” [2]. These resources are those involved in nontechnical skills that are not directly involved in controlling the aircraft (e.g., team communication, leadership, decision-making, task management, stress management). The author envisaged three approaches to improve the management of these nontechnical resources: training, operational procedures, and publications on incident data that would improve awareness within the community. Rapidly, the CRM approach spread to healthcare through the same channels originally proposed by Lauber [1]. General reports on hazards were regularly published by healthcare agencies [3]. The development of medical simulation facilitated the development of Commentary nontechnical skills training. And, task procedures, notably in the form of checklists, were widely implemented. For instance, the WHO Surgical Safety Checklist decreased the risks of wrong-site surgery, the number of post-operative complications, the number of communication failures in the operating room, and helped develop greater safety awareness among team members [4]. However, despite the significant positive effects mentioned above, difficulties have appeared in practice through the emergence of individual resistance, passive non-compliance, or partial application of instructions. Checklists are sometimes viewed as repetitive with regards to other existing safety barriers or as inappropriate regarding the intrinsic variability involved in medical activity and its sudden time-pressured emergencies. Caregivers also report side-effects caused by these new routines. A checklist can lead to a false feeling of security decreasing vigilance in teams or produce distractions if the checklist is used at an inappropriate time [5]. These limitations could be considered as normal effects likely to stabilize with the adjustment of practices. However, another viewpoint might be that the medical field differs significantly from the aviation field and from other domains in which CRM is applied (e.g., nuclear plants).
Aviation is a Tightly Coupled System, Medicine is a Loosely Coupled One
In Human Factors studies, cognitive systems research has pointed out the importance of considering the relations between the work domain, namely the environment on which agents operate, and the work organization composed of agents, tasks, and equipment [6]. From this perspective, aircraft piloting and medical care delivery share some common features, such as dynamic process, human high stakes, and team-based activity. However, whereas aviation involves tight coupling between airspace and pilots, loose coupling exists between patient and caregivers.
A tightly coupled work system entails that numerous variables are shared by the organization and the work domain with strong relations based on conditionality [7, 8]. These networks of relations are used by agents as leverage to control the work domain accurately. Therefore, know-how procedures and automatic control systems are possible – but also requested, to drive operations in the work domain in order to avoid risks emerging from variability in activity. This is the case in the aircraft cockpit, where the airspace is tightly controlled by the human and/or an automatic pilot.
A loosely coupled work system is based on less direct conditional relationships between organization and work domain. Interactions between the two components are more probabilistic than deterministic. Consequently, the coupling can involve few procedural constraints only. More degrees of freedom in modalities to perform a task are available inside the work organization. Even though routines exist in the medical domain, variability is a core component of medical activity regarding both the specific states of each patient and the conditions of work. In contrast to a given piloting action that is highly likely to cause specific effects on the aviation dynamics, the effects of medical gestures are less predictable, as they depend on the patient’s reactions, the moment of their occurrence, and possible interactions with other previous medical interventions.
An indicative context is when the coupling must be recovered after the occurrence of a sudden decoupling event. An adverse event constitutes such decoupling in activity that must be rapidly restored by agents. When an adverse event occurs in aviation, pilots have to manage their levels of uncertainty and the available options to make decision. In the case of a medical emergency, studies show that the decision to call a rapid response team (RRT) in the hospital also depends on several other constraints proper to the work organization. For instance, a novice ward nurse may fear to be blamed for “incorrect” activation of the alarm. Strict adherence to the traditional hierarchical escalation of care leads some caregivers to call the attending physician first rather than the RRT. Calling an external team may also induce the feeling of autonomy loss. Thus, socio-psychological and socio-cultural barriers can significantly intervene in the decision-making process. They correspond with the multiple degrees of freedom that exist in a healthcare system compared with an aircraft cockpit in which the agents are more embedded in the control loop [9].
With these considerations in mind, we can describe the process engaged by the development of CRM both in the field of aviation and medicine. In the case of aviation, CRM increases the level of coupling of nontechnical skills within the cockpit. By standardizing share knowledge, training, and procedures about team coordination, task management, or decision-making, CRM reduces the number of degrees of freedom left to the self-organizing processes that the pilots can engage in context. Variability is reduced in order to reinforce the piloting control loop.
In the case of the medical field considered as a loose coupling system, standardization of nontechnical skills comes in contradiction with the basic kind of relationships established with the work domain. Procedures and checklists reduce the degrees of freedom that can be required to treat the variability emerging from both the variety of patient cases and the multiple manners with which medical teams process their tasks.
Theoretical and Methodological Solutions?
Cognitive systems engineering teaches us that according to the level of coupling between the work domain and the work organization, methodological and theoretical tools are more or less adapted to analyze work situations.
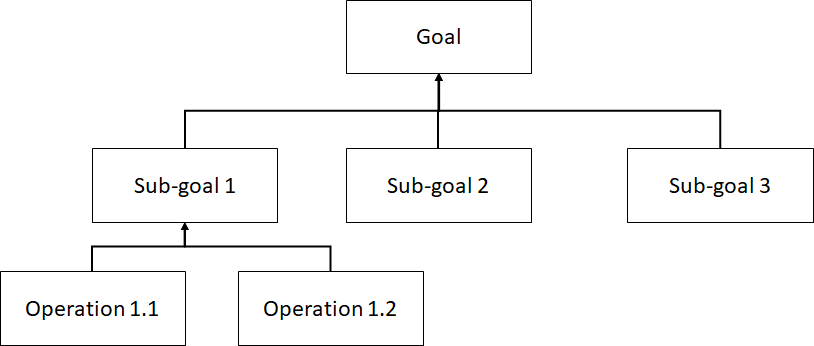
In a tightly coupled work system, such as aviation, tasks can easily be described by methods based on semi-formal sequences of states and operations to follow (Figure 1). The main issue facing this kind of analysis method is how to avoid deviations regarding task sequences that would involve risky work situations. For loosely coupled work systems, the main issue is how to resolve the many degrees of freedom. An adapted theoretical model describing this issue is the Dynamic Safety Model [10, 11]. Agents’ activity can be assimilated to a trajectory in an abstract workspace composed of many degrees of freedom and bounded by functional constraints, such as patient care, information sharing, and task management that can produce pressures on the agents’ trajectory (Figure 2).
![Figure 2: The Dynamic Safety Model describing a healthcare workspace composed of degrees of freedom and bounded by constraints, inspired from [10,11].](/fulltextimages/5244/fig_2.png)
Switching from one model to another leads to change of viewpoint on the use of cognitive aids. An example is the level of compliance required to complete medical checklists. Studies show that the completion rate can be particularly low, as for the WHO surgical checklist that has a degree of compliance of about 50% only during surgical timeout [12]. If we consider the operating room as a tightly coupled system, this low level of compliance is problematic. If we consider the operating room as a loosely coupled system, this low level of compliance indicates that caregivers need many degrees of freedom in order to deal with the multiple competing goals and variability that define their relations with patient care [12].
In fact, no clear dichotomy exists between tightly and loosely coupled work systems. For instance, anesthesia is more tightly coupled than surgery. Hence, the anaesthesia phases have been profitably compared with flight phases [13]. Therefore, even within the same domain, tight and loose relationships exist. Consequently, cognitive work analysis is central to determine the proportion of degrees of freedom (low coupling) and constraints (high coupling) that shape the agents’ behaviors at work, and to consider whether this coupling must be increased or decreased accordingly.
Funding
This study has been supported by a PhD. Grant from Région Bretagne and the Agence Nationale de la Recherche, ANR, in the frame of the VR.MARS project.
References
-
Broom MA, Capek AL, Carachi P, Akeroyd MA, Hilditch G (2011) Critical phase distractions in anaesthesia and the sterile cockpit concept. Anaesthesia 66(3): 175-179.
-
Cooper GE, White MD, Lauber JK (1980) Resource management on the flightdeck. NAS Industry Workshop, NASA CP-2120, NASA, USA.
-
Kohn KT, Corrigan JM, Donaldson MS (1999) To Err Is Human: Building a Safer Health System. National Academy Press.
-
Fomberstein K, Ruskin KJ (2015) Human factors in anesthesia: Risk assessment and clinical decision making. Curr Anaesth Crit Care 5(1): 14-16.
-
Walker IA, Reshamwalla S, Wilson IH (2012) Surgical safety checklists: do they improve outcomes? Brit J Anaesth 109(1): 47-54.
-
Vicente KJ (1999) Cognitive work analysis: Toward safe, productive, and healthy computer-based work. CRC Press.
-
Glassman RB (1973) Persistence and loose coupling in living systems. Behav Sci 18(2): 83-98.
-
Weick K (1976) Educational Organizations as Loosely Coupled Systems. Adm Sci Q 21(1): 1-19.
-
Chua WL, See MTA, Legio-Quigley H, Jones D, Tee A, et al. (2017) Factors influencing the activation of the rapid response system for clinically deteriorating patients by frontline ward clinicians: a systematic review. Int J Qual Health Care 29(8): 981-998.
-
Rasmussen J (1990) The role of error in organizing behaviour. Ergonomics 33(10-11): 1185-1199.
-
Morineau T, Bernard CI, Thierry S (2019) How to control degrees of freedom in a loosely coupled work system? A proposal within the Cognitive Work Analysis framework. Human Factors & Ergonomics Society (HFES) 63rd annual meeting: Seattle.
-
Rydenfält C, EK A, Larsson PA (2014) Safety checklist compliance and a false sense of safety: new directions for research. BMJ Qual Saf 23(3): 183-186. 13. Catchpole K, Russ S (2015) The problem with checklists. BMJ Qual Saf 24(9): 545-549.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30