Effects of Physical Activity on Lower Extremity Muscle Pump and Volume Changes
The objective of the research was to explore the effects of human motion type and angles of inclination on lower limb muscle activity and lower extremity volume change. The muscle activity was quantified by the time domain of the EMG signal. The change in calf circumference and in foot volumeter helped assess the fluid shifts in the lower extremity and the lower limb volume. The results found a significant main effect of motion type on lower extremity muscle activity. Specifically, running was revealed to lead to greater muscle contractions. Also, the calf circumference increase was significantly larger after running than after walking. Calf circumference was significantly greater after running on an inclined surface than on a level surface. Based on the results, inferences were drawn regarding the pattern of fluid shifts in the lower extremity. The research provides valuable inspiration and deep insight into rehabilitation, physiotherapy, and fatigue prevention as well as in the design of prosthetics, compression tights, sports shoes and industrial jobs.
Introduction
Gravity plays a key role in regulating lower extremity volume in humans. Typically, lower extremities (LE) are placed in loaded positions, such as standing, and unloaded positions like sitting. Lower leg muscle’s contract-relax actions prevent venous blood from pooling in LE by facilitating venous return through one-way valves. This effect is known as muscle pump and it is vital in ensuring haemo- dynamic balance in the body [1]. Activity is believed to lead to significant differences in leg volumes. Some studies have reported that aerobic exercise causes a volume increase in LE while others found a leg volume reduction or no change at all [2]. Edema in lower extremities can be an indicator of peripheral vascular diseases. The unclear relationship between the formation of edema and lower-leg position combined with motion type poses a serious research question.
However, excessive lower leg exercises are also risky. Exercising edematous limbs can inflict patients with lymphedema or lower leg circulatory insufficiencies. For those with prostheses, a pronounced limb volume fluctuation due to lower extremity aerobic exercise can render the prosthesis unfit. With a deepening understanding of LE venous dynamics, people can develop a variety of corresponding exercises to diminish the risk of edema.
Study of the relationship between lower leg physical activity and the extent of edema has potential in design for suitable prosthetic limbs, sport shoes, and compression tights. For example, it is not uncommon for marathon runners to select shoe sizes bigger than their foot size to accommodate the supposed swelling of feet during running. But if foot volume change doesn’t actually take place, larger shoe sizes may result in blisters [3]. As a result, there is an increasing focus on ergonomic interventions to prevent musculoskeletal disorders (MSDs) at workplaces by redesigning tasks. However, the lack of consensus regarding LE venous dynamics makes it difficult to design appropriate ergonomic interventions. Overall, this study enriches our understanding of LE dynamics by providing a new perspective obtained by the innovative combined of EMG, volumetry, and calf circumference measurements, thus promoting our design guideline of effective ergonomic interventions at the workplace.
Literature Review
Effect of Walking
The effect of walking on foot conditions has been explored intensively [4]. A higher walking speed (6 km/h) for the same duration initially caused a rapid reduction of foot volume, yet later on that change became insignifcant. This phenomenon is due to the effect of musculo-venous pumping counteracting the increased blood flow to the exercising muscles. Skeletal muscle pump plays an important role in preventing edema in lower legs [5]. In another study, a significant increase in foot volume was observed during a 10-minute walk at a self-selected speed among male and female student participants aged 22 to 34 [6]. The symptom of increased edema is explained by the increased blood flow to the exercising muscles of lower extremities and the subsequent shift of capillary fluid to the interstitial space [7].
Effect of Running
Previous studies have demonstrated divergent results of how running affects lower limb volume change after long time activities. The decrease in lower extremity volume is explained by muscle pumping effect that leads to a better rate of venous return [8]. Similarly, significant increases in foot volume were found after running at a self-selected speed [9]. During daily activities, human body tries to maintain equilibrium of fluids in the lower extremities by pumping excess interstitial fluid back into the heart [10]. The balance of fluids between the capillaries and interstitial space is maintained by balancing the hydrostatic pressure of the capillaries and the osmotic pressure of the interstitial fluid. Limitations of Previous Research The effect of activities, such as walking and running, on lower leg volume change is considered controversial. It has been widely accepted that some degree of limb motion can help in reducing edema during activities [11]. For most studies, an increased foot volume has been observed after short bouts of running, whereas after longer duration of running a reduction has been observed. There has been conflicting literature regarding the effect of walking on feet. The difference may be attributed to the diversity of measurement technique, such as mercury-in-silastic strain gauge, water displacement volumetry, or optical foot scanner [12]. Varied duration of tasks and gait speeds may also account for outcome difference.
Large fluctuations of lower leg volume can potentially contribute to aggravated edema in the long term. Also, a couple of research has independently studied the EMG signal readings of lower leg musculature for different task types [13]. However, so far no work has explored the relationship between the LE muscle EMG activity and the lower leg volume change. It is also uncertain how much muscle activity is sufficient to prevent leg volume increase. Finally, several studies have proposed different mechanisms to explain their results on LE volume change; however, no consensus has been obtained.
Research Question
This study seeks to investigate if leg muscle pump varies with inclination and gait speed, as well as to find the best possible combination of motion type and inclination as prescriptive exercises for people with chronic edema.
Methodology
Participants
A screening questionnaire was first employed to exclude volunteers with any prior lower leg disorders, lower leg injury, breathing problems, respiratory illnesses, heart diseases or abnormal high or low blood pressure (over 140/90 or below 100/80). As a result, a small group of twelve healthy male participants aged 22 to 42 years (M=27.16, SD=6.27), weighted from 60.3 to 93 kg (M=73.28, SD=10.01) and with stature from 165.1 cm to 185.5 cm (M=174.13, SD=5.61) were enrolled into the study. All the participants were either moderately or highly active. Moderate activity level was defined as the performance of lower leg activities for 1-2 times a week and high activity level was defined as that for 3 or more times a week. All participants were provided with written, informed consent forms. The study had been reviewed and approved by the Institutional Review Board (IRB) of Lamar University.
Apparatus
The experiment used MP150 data acquisition and analysis systems with AcqKnowledge software to conduct EMG. Other apparatus include foot volumeter (North Coast Medical Inc. Foot Volumeter), gulick tape (Country Technology Inc, WI), EL 500 Electrodes, 40 EL Electrode Leads, a Biopac EL-Check Electrode Impedance Checker, and a treadmill (Trackmaster TMX425C).
Experiment Design
Independent Variables: The type of motion (treadmill walking at 2.5 mph, treadmill running at 4.5 mph) and angle of inclination (0 and 5 percent) were chosen as independent variables. The experiment was a 2 x 2 factorial within- subjects design.
Dependent Variables: The dependent variables included variations of the calf circumference, foot volume variation, and the peak RMS EMG amplitude of Tibialis Anterior (TA) and Gastrocnemius (GA) muscles normalized to their Maximum Voluntary Contraction (MVC). GA and TA muscles were chosen as they play a key role in maintaining postural stability during standing. RMS EMG is defined as the time windowed RMS value of the raw EMG and can produce more easily analyzable waveformse.
Task Description Running: The participants followed a normal gait for running. The running speed was set at 4.5 mph and the duration was 5 minutes. This motion was experimented at two different inclinations of 0 and 5percent. Walking: The participants followed a normal gait for walking. The walking speed was set at 2.5 mph and the duration was 5 minutes. This motion was experimented at two different inclinations of 0 and 5 percent.
The sequence of all experiment tasks was completely randomized by online research randomizer before being assigned to participants. Procedure The recruited participants were first instructed on the experiment protocol prior to the experiment. Following this, each participant was handed an informed consent form. Pre-test questionnaires were assigned to learn participants’ demographic information, such as age, weight, and height, as well as their typical amount of activity each week.
After reporting to the researchers, the participants had a portion of hair removed from the skin over GA and TA to facilitate the attachment of electrodes to measure skin-electrode impedance and EMG. The participants were then allowed to lie in a supine position for 20 minutes. Afterwards, the participants slowly shifted to a sedentary posture with legs extended. Then a gulick tape was used to measure baseline calf circumference; the baseline foot volume was measured with the volumeter. The electrodes were then attached at the skin over GA and TA. The leads were then connected to the impedance checker to measure the impedance. Once an acceptable reading of the impedance was achieved (<5 kilo ohms), the electrode leads were detached from the impedance checker and attached to the EMG signal transmitter. The transmitter was attached to each participant’s ankle with a Velcro strap at a very minimal pressure.
After having baseline measurements taken, the participants moved to the treadmill with the EMG electrodes attached to their lower limbs. The walking task was performed at a moderate speed of 2.5 mph and the running session was performed at a speed of 4.5 mph, all for a duration of 5 minutes, all at two inclines: 0percent and 5percent. The running speed was set at 4.5 mph bexause this speed was observed to be a common speed adopted while participants transitioned from a walking gait to a running gait. The raw EMG was collected for the final 30 seconds of the task at a sampling rate of 2000 Hz. The signals were filtered with the notch filter at 60 Hz to remove power line noise, and band- pass filter at 50Hz- 500Hz to remove motion artefacts. At the end of each task, the calf circumference was measured using the gulick tape and the change in foot volume was measured with volumetry.
Data Analysis
EMG analysis was performed in time domain. Peak RMS EMG normalized to the Maximum Voluntary Contraction (MVC) was analyzed for walking and running tasks. To exert GA, the participants flexed their foot soles against the ground while supporting a certain fixed resistance on their shoulders in a gradual and continuous 2-second build-up of effort culminating in a 2-second maximal effort. For TA, participants dorsiflexed their foot against a fixed resistance applied at the metatarsals while standing (Figure 1). A repeated two-way ANOVA was conducted to analyze the effect of motion type and inclination on foot volume, calf circumference, and EMG activity.

Results
Foot Volume Change
No significant main effect of either motion type (F_1,11 = 1.47, p = 0.2500) or inclination (F_1,11 = 1.53, p = 0.2420) was detected on foot volume change. Foot volume tended to increase for both incline and level conditions; however, the rate of increase was more pronounced for the inclined surface (M = 11.66, SD = 27.82) compared to the level surface (M = 4.88, SD = 16.83). Also, although both running and walking conditions led to a foot volume increase, running led a greater foot volume increase (M = 11.96, SD= 19.21) compared to walking (M = 4.58, SD = 26.15). There was no significant interaction effect (F_1,11 = 0.03, p = 0.8661). The greatest increase in leg volume was observed for inclined running (M = 14.58, SD = 22.93), followed by level running (M = 9.33, SD = 15.20), and inclined walking (M = 8.75, SD = 32.77). The least increase was noted for level walking (M = 0.42, SD = 17.83).
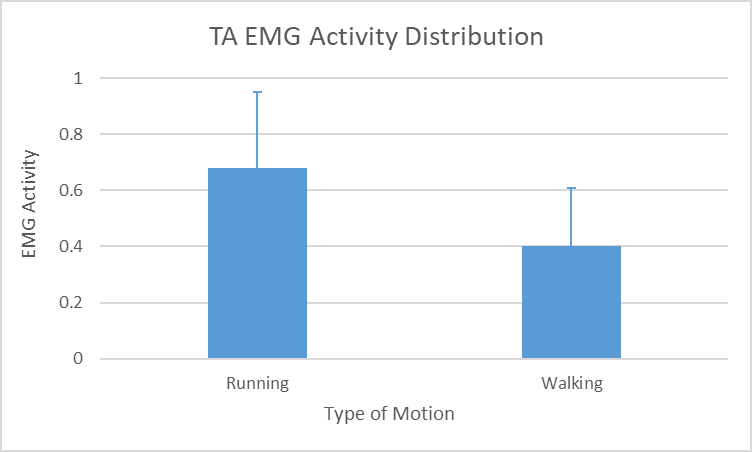
EMG Activity at Tibialis Anterior (TA)
There was a significant main effect of motion type on TA activity (F_1,11= 14.59, p = 0.0028). Post hoc analysis revealed that muscle activity on TA during running (M = 0.68,
SD = 0.27) was significantly greater than that for walking (M = 0.40, SD = 0.21) (Figure 2). It was observed that the level of inclination did not alter the TA EMG activity significantly (F_1,11= 0.71, p = 0.4160) nor was there an significant interaction effect (F_1,11 = 0.02, p = 0.9011). An incline of 5 percent was not found to significantly affect TA muscle activity. The highest EMG activity was recorded for inclined running, followed by level running. The least EMG activity was noted for level walking.
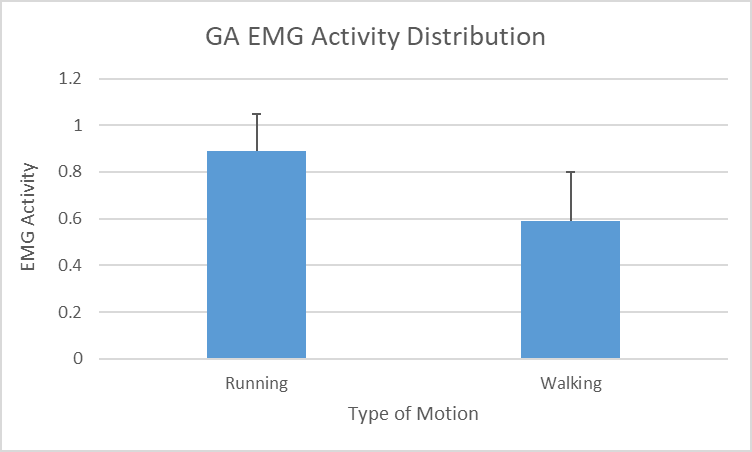
EMG Activity at Gastrocnemius (GA)
GA muscle activity was found to be significantly affected by motion type (F_1,11= 34.07, p <0.0001). Post hoc analysis revealed that muscle activity on GA for running (M = 0.89, SD = 0.16) was significantly greater than that for walking (M = 0.59, SD = 0.21) (Figure 3). Although the level of exertion was in general higher for the inclined surface (M = 0.78, SD = 0.21) compared to the level surface (M = 0.70, SD = 0.25), the effect was not significant (F_1,11= 2.40, p =0.1497). An elevation of up to 5 percent was not found to significantly change GA muscle activity. Inclined running had the highest EMG activity, followed by level running. Level walking generated the least intensive EMG activity. However, there was no significant interaction effect (F_1,11= 1.46, p = 0.25).
Calf Circumference
The analysis revealed a significant main effect of both the motion type (F_1,11 = 40.18, p < 0.0001) and inclination (F_1,11 = 5.36, p = 0.0410) on calf circumference. Running led to a significant greater calf circumference increase (M = 0.53, SD = 0.28) compared to walking (M = 0.15, SD = 0.21). The inclined surface tended to evoke a significant greater increase in calf circumference (M = 0.43, SD = 0.33) compared to the level surface (M = 0.26, SD = 0.27). There was no significant interaction effect (F_1,11 = 0.01, p = 0.9061). The largest increase in calf circumference was observed from inclined running, followed by level running, while the least increase was found in level walking.
Discussion
Effect of Motion Type
There is a significantly greater increase in calf circumference during running compared to walking. Also, under running conditions, the foot volume tends to increase more than walking although this phenomenon is not significant. Practically these findings provide valuable ergonomics insight on shoe design for different groups of users. The significantly higher intensity of muscular exercise under running conditions could be evidenced from the EMG signals at both TA and GA. Both muscles function at a higher percentage of their MVC under running conditions. Hence, there might have been less blood flowing to the exercising muscles of LE during walking, which resulted in a lower calf circumference increase. This could be another reason why walking resulted in a lower LE volume increase compared to running. Also, the effect of muscle pump during walking could be sufficient to ensure a consistent venous return and an efficient pumping of fluid out of interstitial spaces.
Research has identified three potential contributing factors for LE volume reduction: lowered venous pressure, which reduces filtration pressure; better lymph dynamics, removing colloid proteins from interstitial spaces; and increased muscle tissue pressure, due to muscle contraction. A short period of relaxation of soleus during gait cycle could decrease venous pump efficiency [14]. Less interstitial fluid, owing to reduced filtration pressure in walking, also leads to a correspondingly less load on lymphatics. Therefore, it is not surprising that several participants had a reduced leg volume even after walking. Since an increase in interstitial and extracellular fluid volume is manifested in the swelling of lower limbs and is related to workload, this could be one reason why running resulted in LE volume increase [15].
This study has noted an interesting contradiction with the suggestions of previous research: Two studies suggested that stronger muscular contractions would result in greater interstitial fluid pressure, which counteracts the intravascular pressure and stops trans-capillary filtration, thereby contributing to foot volume reduction [16]. This effect is, however, not observed in this study as foot volume seems to be increasing with stronger muscular contractions. Hence it is possible that this effect may be a natural muscle mechanism to counteract the increasing fluid shift to the interstitials over a prolonged activity and may be evident only if the interstitial fluid volume exceeds a particular quantity. Therefore, in a short bout of intense activity, as in this experiment, above mentioned effect may not be manifest.
Effect of Inclination
As observed from the experiment, across both running and walking, a generally higher TA and GA EMG activity and an increasing trend for foot volume was observed under incline conditions, suggesting the role of strong muscle contractions in foot volume increase.
A significantly greater calf circumference after incline activity confirms the results of volumetry. Incidentally, the highest TA and GA EMG activity, which was recorded during inclined running, also witnessed the greatest foot volume and calf circumference increase. This indicates how greater inclines and rigorous activity types can jointly generate greater muscle contractions to result in a foot volume increase. It is possible that the metabolites and macromolecules released due to the high levels of exertion might have overloaded the lymphatics.
Walking gait has been found to be more efficient than running at minimizing foot volume change. This could probably be due to the characteristic of muscle dynamics, the way the muscles contract and extend during walking gait. More studies need to be performed to examine difference of muscle dynamics between gait patterns of walking and running, and how the degree of foot dorsiflexion affects muscle pump. This could conclusively show the effect of calf muscle pump on controlling foot volume.
Conclusion
This study finds that motion type and inclination can significantly affect calf circumference. Also a direct relationship is identified between muscle contraction levels and LE swelling. Specifically, running leads to greater muscle contractions, and the calf circumference increase significantly after running. This study, for the first time combines EMG, volumetry, and calf circumference measure to study the effect of LE muscle dynamics on volume change and to assess fluid shifts under different activity-incline combinations. Calf circumference is proven to be more reliable in detecting fluid volume shifts which inspires the innovation of smart wearables detecting occupational fatigue that prevails among policemen, rescuers, emergency responders and etc. This study also validates level walking as the most suitable gait-incline combination to exercise edematous limbs. By combining foot volumetry and calf circumference, this is the only study to date which provides an overall picture of the cumulative effect of peripheral and deep vein circulation on the regulation of foot volume without the use of invasive techniques.
There are some shortcomings in this study. The sample size is expected to be enlarged and the population background needs to be enriched in future research. In the future, female, people with different occupations and life style will be recruited, to study gender, occupational and life style difference in the physiological parameters. It is known that walking exercise training help reduce intermittent claudication symptoms [17]. Also, the contribution of lymph dynamics in aiding LE volume regulation may be studied using a colored dye technique. Ultrasound sonometers and perometers could also be employed to further study whether the volume accumulation is intravascular or extravascular in origin.
Acknowledgments
Declaration of interest
None
References
-
Recek C (2013) Calf pump activity influencing venous hemodynamics in the lower extremity. International Journal of Angiology 22(1): 23-30.
-
Chalk PJ, McPoil T, Cornwall M (1995) Variations in foot volume before and after exercise. Journal of American Podiatric Medical Association 85(9): 470-472.
-
Mailler-Savage EA, Adams BB (2006) Skin manifestations of running. Journal of the American Academy of Dermatology 55(2): 290-301.
-
Buldt K, Murley GS, Butterworth P, Levinger P, Menz HB, et al. (2013) The relationship between foot posture and lower limb kinematics during walking: A systematic review. Gait & posture 38(3): 363-372.
-
Uhl JF, Gillot C (2014) Anatomy of the veno-muscular pumps of the lower limb. Phlebology: The Journal of Venous Diseses 30(3): 180-193.
-
McWhorter JW, Wallmann H, Landers M, Altenburger B, LaPorta-Krum L, et al. (2003) The effects of walking, running and shoe size on foot volumetrics. Physical Therapy in Sport 4 (2): 87-92.
-
Gellman R, Burns S (1996) Walking aches and running pains: injuries of the foot and ankle. Primary Care: Clinics in Office Practice 23(2): 263-280.
-
Lazzarini KM, Troiano RN, Smith RC (1997) Can running cause the appearance of marrow edema on MR images of the foot and ankle? Radiology 202(2): 540-542.
-
Mayrovitz HN (1998) Posturally induced leg vasoconstrictive responses: Relationship to standing duration, impedance, and volume changes. Clinical Physiology 18(4): 630-634.
-
Kunde S, Milani TL, Sterzing T (2009) Relationship between running shoe fit and perceptual, biomechanical and mechanical parameters. Footwear Science 1(suppl 1): 19-20.
-
Karimi Z, Allahyari T, Azghani MR, Khalkhali H (2016) Influence of unstable footwear on lower leg muscle activity, volume change and subjective discomfort during prolonged standing. Applied ergonomics 53: 95-102.
-
Hoyer C, Pavar S, Pedersen BH, Biurrun Manresa JA, Petersen LJ (2013) Reliability of mercury-in-silastic strain gauge plethysmography curve reading: influence of clinical clues and observer variation. Scandinavian journal of clinical and laboratory investigation 73(5): 380-386.
-
Isezaki T, Kadone H, Niijima A, Aoki R, Watanabe T, et al. (2019) Sock-type wearable sensor for estimating lower leg muscle activity using distal EMG signals. Sensors 19(8): 1954.
-
Stick C, Hiedl U, Witzleb E (1993) Venous pressure in the saphenous vein near the ankle during changes in posture and exercise at different ambient temperatures. European journal of applied physiology and occupational physiology 66(5): 434-438.
-
Lerebourg L, L’Hermette M, Menez C, Coquart J (2020) The effects of shoe type on lower limb venous status during gait or exercise: A systematic review. PLoS One 15(11): e0239787.
-
Mahesh V, Li Y, Craig B (2018) Effect of Motion Type and Inclination on Muscle Activity and Edema. In: Goonetilleke R, et al. (Eds.), Advances in Physical Ergonomics and Human Factors, Springer, USA, pp: 335- 342.
-
Lane R, Harwood A, Watson L, Leng GC (2017) Exercise for intermittent claudication. Cochrane Database of Systematic Reviews 12: CD000990.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30