Standing vs. Sitting-Office Ergonomics…A Study of the Health Benefits
Groundnut holds a pivotal role in Indian agriculture, serving as a critical crop contributing to both the economic and nutritional sectors of the country. Timely harvesting of groundnut is a crucial phase in its cultivation, particularly during peak seasons, when labor shortages can lead to delays, resulting in significant yield losses. To mitigate labor constraints during peak harvesting periods and ensure timely operations, a conceptual model of a groundnut digger has been proposed. This digger is designed to uproot, collect, and transport groundnut plants, inverting them as it moves through the field. The groundnut digger consists of two primary units: a digging unit and a conveying unit. The digging unit is engineered to penetrate the soil to a precise depth, extracting the groundnut plants along with the attached pods to the surface. The conveying unit is responsible for lifting the plants and transporting them to a pod-inverting mechanism, which inverts the plant to reduce the risk of aflatoxin contamination in the pods due to excessive soil moisture.
Abbreviations
BMI: Body Mass Index; IRB: Institutional Review Board; MSD: Musculoskeletal Discomfort.
Introduction
Studies have consistently highlighted the negative effects of prolonged sitting on health. Biswas, et al. [1] conducted a comprehensive meta-analysis that revealed a significant association between sedentary behavior and various health concerns, including obesity, cardiovascular diseases, and musculoskeletal discomfort. This meta-analysis synthesized findings from multiple studies, providing a comprehensive overview of the negative health impacts of prolonged sitting. Similarly, Dunstan, et al. [2] explored the potential benefits of breaking up prolonged sitting with standing or light activity. Their research showed that such interventions could lead to improvements in blood pressure and a reduction in the risk of cardiovascular problems. This finding suggests that simple adjustments in daily routines, such as incorporating standing breaks, can contribute to better cardiovascular health.
Moreover, Parry, et al. [3] and Wilks, et al. [4] focused specifically on the impact of standing workstations. Parry, et al. highlighted the potential of standing workstations in alleviating musculoskeletal issues and reducing the risk of back pain. Wilks et al. extended these findings, emphasizing the positive effects of standing workstations on overall posture. Both studies underscored the importance of considering alternative work arrangements to mitigate the adverse effects of prolonged sitting. Adding to this body of research, Ma, et al. [5] investigated the effects of a workplace sit-stand desk intervention on health and productivity. Their study provided insights into the potential benefits of incorporating standing time for office workers, aligning with the objectives of our research study. By examining the health and productivity outcomes of standing desk interventions, Ma, et al. [5] contributed valuable information to the existing literature, emphasizing the importance of exploring alternative work arrangements to promote employee health and well-being.
To contribute to this body of knowledge and build upon these findings, our research study has specifically explored the health benefits of incorporating standing time for office workers using measurable health and survey data. Also, a discomfort survey was designed and approved by the Human Subject Review Board at the University of Houston-Clear Lake for use with data collection for this study.
Materials and Methods
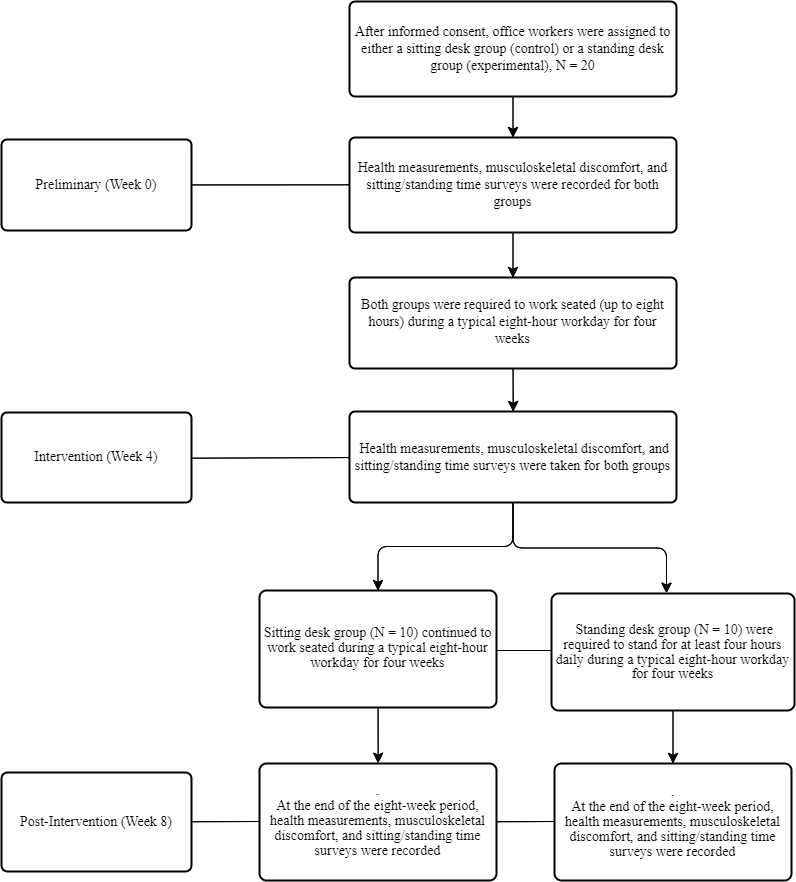
In this study, office workers were recruited and assigned to either a sitting desk group (control) or a standing desk group (experimental). The sitting desk group worked seated for eight weeks, and the standing desk group worked seated for the first four weeks and incorporated standing time for the next four weeks. Surveys measuring health, musculoskeletal discomfort, and sitting/standing time were conducted initially (preliminary), after four weeks (intervention), and after eight weeks. One-sample T-tests were conducted to analyze the two groups, assessing changes and differences in weight, blood pressure, heart rate, body mass index (BMI), and level of musculoskeletal discomfort. The level of musculoskeletal discomfort was rated on a scale of 1 to 20 across five body regions – head/neck, back/torso, arms, legs, and feet. Moreover, the null hypothesis (H_0_) was identified as “no significant change or difference in health parameter data in the standing desk group after the study period.” The alternative hypothesis (H_a_) was defined as “a significant change or difference in health parameter data in the standing desk group after the study period.” (Figures 1 & 2).

Participants
A power analysis determined the sample size needed to detect significant changes or differences in the studied population. With an alpha level of 0.05 and a beta level of 0.8, it was found that a sample size of 20 participants was adequate to detect any changes or differences in the two groups with a reasonable level of confidence. Participants from various office settings, ages ranging from 18 to 69, were recruited, assessed, and divided into two groups: a controlled sitting desk group (n = 10) and an experimental standing desk group (n = 10). The participants’ workplaces were typical office environments where desk-based work is performed. This included corporate offices, government offices, academic institutions, small businesses, home offices, or any other organization where office work is common. The specific type of work performed by the participants was a wide range of office-based tasks, such as administrative work, data analysis, customer service, and other desk- based activities. Before participants were involved in this study, approval by the Human Subject Review Board at a local university was consulted and provided approval. The Institutional Review Board (IRB) classified this study as Exempt Research (Category 2), and participants were required to sign a consent form before being involved in this study.
Experiment Design
Preliminary health measurements, musculoskeletal discomfort, and sitting/standing time surveys were recorded first, using parameters such as weight, blood pressure, heart rate, BMI, and level of musculoskeletal discomfort (1 to 20). Instruments used were an Omron - 3 Series - Automatic Upper Arm Blood Pressure Monitor and a ZIQING - Digital Wrist Blood Pressure Monitor, BP Cuff, LCD Heart Rate Machine. Normal ranges for these measurements adhered to the American Heart Association’s established medical guidelines and standards, such as a normal blood pressure of around 120/80 mm Hg, normal resting heart rate range between 60 and 100 bpm, and a BMI between 18.5 to 24.9. Afterwards, both groups were required to work seated (up to eight hours) during a typical eight-hour workday for four weeks. Instruments used to monitor compliance included timesheet logs to track the time spent sitting and standing. After the four-week sitting period, health measurements, musculoskeletal discomfort, and sitting/standing time surveys were recorded for both groups and compared to the preliminary results using the same parameters. For the next four weeks, the sitting desk group continued to work seated (up to eight hours), and the standing desk group were required to stand for at least four hours daily during a typical eight-hour workday. Timesheet logs were used to monitor compliance for the time spent sitting and standing.
At the end of the eight-week period, health measurements, musculoskeletal discomfort, and sitting/standing time surveys were recorded for both groups to compare the effects of the standing intervention. The parameters assessed included the same ones as in the preliminary and baseline measurements, such as weight, blood pressure, heart rate, BMI, and level of musculoskeletal discomfort (1 to 20). The instruments used were consistent with the earlier measurements, and normal ranges for these measurements adhered to the established AHA medical guidelines. This experiment aimed to explore if the standing desk group had better health parameters at the end of the eight-week study period (Figure 3).
Data Analysis
Data was collected through objective health measurements and subjective musculoskeletal, sitting/ standing time surveys. Statistical methods included the use of one-sample t-tests, to compare health parameters in the two groups, with informed consent obtained from all participants. One-sample t-tests were chosen to compare the means of health parameters in the sitting desk (control) and standing desk (experimental) groups at different intervals, specifically after four weeks (baseline) and after eight weeks. In this case, t-tests determined whether there were statistically significant differences in health parameters among participants who incorporated standing time into their work routine. A significance level of 0.05 was used to determine statistical significance. If the p-value obtained from the t-test was less than 0.05, it indicated that there was sufficient evidence to reject the null hypothesis and accept the alternative hypothesis, suggesting that there are significant changes or differences in health parameter data in the standing desk group after the study period. Conversely, if the p-value is greater than or equal to 0.05, it suggests that there is insufficient evidence to reject the null hypothesis, indicating that there are no significant changes or differences in health parameter data in the standing desk group after the study period.
Results
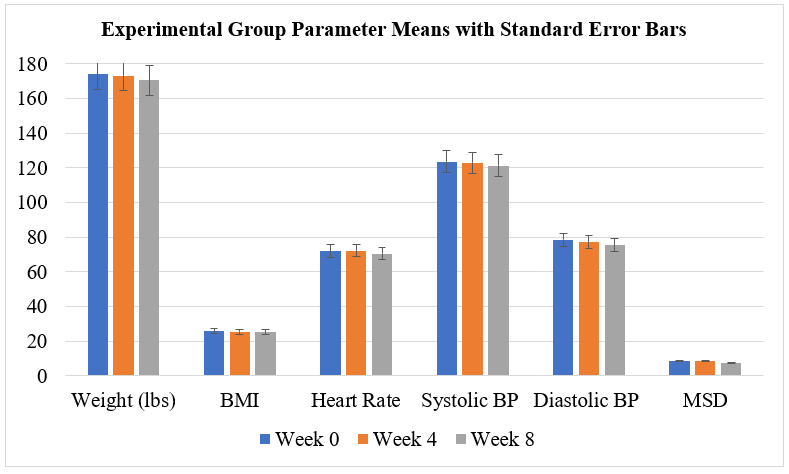
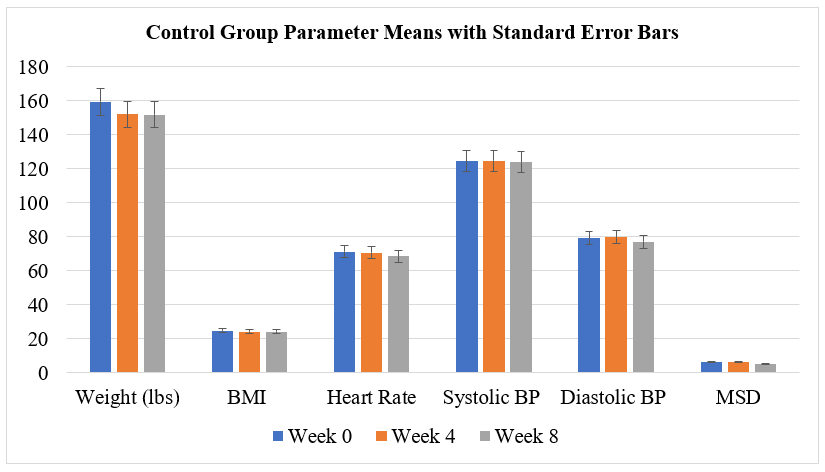
Tables 1,2 below show the weekly mean sitting and standing hours for the sitting desk (control) and standing desk (experimental) groups over the eight-week study period. At week 4 (intervention period), the control group (sitting desk) worked seated for an average of 35.35 hours and worked standing for an average of 4.65 hours, while the experimental group (standing desk) worked seated for an average of 34.40 hours and worked standing for an average of 5.60 hours. At week 8, the control group worked seated for an average of 36.65 hours and worked standing for an average of 3.35 hours, whereas the experimental group worked seated for an average of 20.65 hours and worked standing for an average of 19.35 hours. Tables 3,4, and Figures 4,5 report the mean values and standard errors for the following parameters: weight, BMI, resting heart rate, systolic and diastolic blood pressure, and musculoskeletal discomfort rating for both groups at Week 0, Week 4, and Week 8. Moreover, Tables 5,6 below show the results of the one-sample t-tests comparing the post intervention period of Week 4 and Week 8 means for each parameter for both the control group (sitting desk) and the experimental group (standing desk) at a significance level of 0.05. A t-distribution with 9 degrees of freedom (N-
1) for the critical values was used. The t-statistic measures the magnitude of differences between the means of Week 4 and Week 8 relative to the variability in the data. A higher absolute value of the t-statistic indicates larger differences between the means. The p-value indicates the probability of obtaining the observed results if the null hypothesis (no significant changes or differences in health parameter data in the standing desk group after the study period) is true. A lower p-value suggests stronger evidence against the null hypothesis, considered statistically significant if below 0.05.
- Control Group: Mean Sitting and Standing Hours
- Week
- Mean Sitting Hours
- Mean Standing Hours
- 1
- 36.5
- 3.5
- 2
- 34.35
- 5.65
- 3
- 36.25
- 3.75
- 4
- 35.35
- 4.65
- Intervention Period – No Change
- 5
- 34.45
- 5.55
- 6
- 34.65
- 5.35
- 7
- 35.5
- 4.5
- 8
- 36.65
- 3.35
Table 1: Control Group: Mean Sitting and Standing Hours.
- Experimental Group: Mean Sitting and Standing Hours
- Week
- Mean Sitting Hours
- Mean Standing Hours
- 1
- 35.25
- 4.75
- 2
- 35.45
- 4.55
- 3
- 36
- 4
- 4
- 34.4
- 5.6
- Intervention Period – Work Standing
- 5
- 18.75
- 21.25
- 6
- 19.25
- 20.75
- 7
- 25.2
- 14.8
- 8
- 20.65
- 19.35
Table 2: Experimental Group: Mean Sitting and Standing
- Control Group Parameter Means and Standard Errors
- Parameter
- Week 0 Mean Week 0 Std Error Week 4 Mean Week 4 Std Error Week 8 Mean Week 8 Std Error
- Weight (lbs)
- 159.5
- 10.3
- 152.1
- 9.2
- 151.8
- 9.1
- BMI
- 24.9
- 0.7
- 24.1
- 0.6
- 24.1
- 0.6
- Resting heart rate
- 71.2
- 1.8
- 70.7
- 1.5
- 68.5
- 1.7
- Systolic BP (mmHg)
- 124.6
- 3
- 124.8
- 2
- 124
- 1.9
- Diastolic BP (mmHg)
- 79.2
- 2.2
- 79.8
- 1.5
- 77.2
- 1.4
- MSD
- 6.4
- 0.6
- 6.5
- 0.4
- 5.1
- 0.5
Table 3: Control Group Parameter Means and Standard Errors.
- Experimental Group Parameter Means and Standard Errors
- Parameter
- Week 0 Mean
- Week 0 Std
- Error
- Week 4 Mean
- Week 4 Std
- Error
- Week 8 Mean
- Week 8 Std
- Error
- Weight (lbs)
- 174.1
- 6.3
- 173.1
- 5.6
- 170.5
- 5.5
- BMI
- 25.7
- 0.8
- 25.3
- 0.7
- 25.1
- 0.7
- Resting heart rate
- 71.9
- 2.4
- 72.1
- 2.1
- 70.3
- 2.4
- Systolic BP (mmHg)
- 123.6
- 2.9
- 122.9
- 2.8
- 121.3
- 2.6
- Diastolic BP (mmHg)
- 78.4
- 2.3
- 77.1
- 2
- 75.3
- 1.9
- MSD
- 8.5
- 0.9
- 8.3
- 0.7
- 7.1
- 0.8
Table 4: Experimental Group Parameter Means and Standard Errors.
| Control Group One-Sample t-tests | |||
|---|---|---|---|
| Parameter | t-statistic | p-value | Week 4 vs Week 8 |
| Weight | 0.137 | 0.894 | Not significant |
| BMI | 0 | 1 | Not significant |
| Resting heart rate | 1.46 | 0.184 | Not significant |
| Systolic BP | 0.202 | 0.844 | Not significant |
| Diastolic BP | 0.467 | 0.654 | Not significant |
| MSD | 2.147 | 0.062 | Not significant |
Table 5: Control Group One-Sample _t_-tests.
| Experimental Group One-Sample t-tests | |||
|---|---|---|---|
| Parameter | t-statistic | p-value | Week 4 vs Week 8 |
| Weight | 1.044 | 0.325 | Not significant |
| BMI | 1.118 | 0.294 | Not significant |
| Resting heart rate | 1.604 | 0.149 | Not significant |
| Systolic BP | 1.408 | 0.195 | Not significant |
| Diastolic BP | 1.65 | 0.143 | Not significant |
| MSD | 3.368 | 0.009 | Significant (p < 0.05) |
Table 6: Experimental Group One-Sample _t_-tests.
The results of the one-sample t-tests comparing Week 4 and Week 8 means for each parameter in both the control and experimental groups suggest that, overall, there are no significant differences between the means of these parameters over the four-week interval, except for musculoskeletal discomfort (MSD) in the experimental group. In summary, the statistical analysis suggests that while there were no significant changes in most parameters between Week 4 and Week 8 for both groups, individuals using standing desks experienced a significant change in musculoskeletal discomfort levels over the four-week period.
In addition to the analysis seen in Tables 5 6, we further examined the changes in health parameters from Week 0 to Week 8 within each group. Table 7 shows the results of one-sample t-tests comparing Week 0 and Week 8 means for the control group (sitting desk), while Table 8 shows the same analysis for the experimental group (standing desk). Notably, in Table 7, significant differences were observed in musculoskeletal discomfort (MSD) levels for the control group, indicating a decrease in musculoskeletal discomfort from Week 0 to Week 8. Conversely, Table 8 shows significant changes in systolic and diastolic blood pressures, and musculoskeletal discomfort for the experimental group. These findings suggest that while the control group experienced a reduction in musculoskeletal discomfort over the eight-week period, the experimental group demonstrated significant improvements in both blood pressure parameters and musculoskeletal discomfort, indicating potential health benefits associated with using standing desks.
| Control Group One-Sample T-tests | |||
|---|---|---|---|
| Parameter | t-statistic | p-value | Week 0 vs Week 8 |
| Weight | 0.221 | 0.831 | Not significant |
| BMI | 0 | 1 | Not significant |
| Resting heart rate | 1.961 | 0.083 | Not significant |
| Systolic BP | 0.581 | 0.58 | Not significant |
| Diastolic BP | 0.775 | 0.475 | Not significant |
| MSD | 3.377 | 0.009 | Significant (p < 0.05) |
Table 7: Control Group One-Sample T-tests.
| Experimental Group One-Sample t-tests | |||
|---|---|---|---|
| Parameter | t-statistic | p-value | Week 0 vs Week 8 |
| Weight | 1.546 | 0.179 | Not significant |
| BMI | 1.273 | 0.244 | Not significant |
| Resting heart rate | 1.572 | 0.157 | Not significant |
| Systolic BP | 2.5 | 0.039 | Significant (p < 0.05) |
| Diastolic BP | 3.04 | 0.017 | Significant (p < 0.05) |
| MSD | 4.031 | 0.003 | Significant (p < 0.05) |
Table 8: Experimental Group One-Sample _t_-tests.
Discussion
The results of this study provide valuable insights into the potential health benefits of incorporating standing time for office workers. Previous literature has consistently highlighted the negative effects of prolonged sitting on various health parameters. Biswas, et al. [1] demonstrated a significant association between sedentary behavior and adverse health outcomes, including obesity, cardiovascular diseases, and musculoskeletal discomfort. Similarly, Dunstan DW, et al. [2] emphasized the potential benefits of breaking up prolonged sitting with standing or light activity, showing improvements in blood pressure and reduced risk of cardiovascular problems.
The results of this study indicate several noteworthy observations. First, while both groups showed very little changes in most health parameters over the eight-week period, the experimental group which incorporated standing time, showed significant improvements in musculoskeletal discomfort (MSD) and systolic as well as diastolic blood pressure improvements. This aligns with the findings of Parry, et al. [3], Wilks, et al. [4], Amick, et al. [6], and Ma, et al. [5], who emphasized the positive effects of standing workstations on musculoskeletal discomfort and posture. Similarly, the experimental group showed trends towards lower systolic and diastolic blood pressures which confirms previous research by Dunstan, et al. [2], suggesting potential cardiovascular benefits associated with standing time. Moreover, several limitations and challenges must be addressed to accurately interpret and apply our findings. One of the primary limitations of the study is the relatively small sample size. With only twenty participants divided into two groups, the study may lack the statistical power to detect subtle differences in health parameters in the sitting and standing desk groups. In addition, the short duration of the intervention, lasting only eight weeks, may not have been long enough to see significant changes in certain health parameters [7, 8, 9, 10, 11, 12].
Another limitation of our study is the potential for variability in participant compliance with the intervention. While timesheet logs were utilized to monitor the time spent sitting and standing, participants’ willingness and ability to consistently use a standing workstation may have influenced the results. The study also did not control confounding variables such as physical activity levels outside of work, dietary habits, and pre-existing health conditions. Without accounting for all these factors, it is challenging to attribute any observed changes solely to the use of standing desks.
Conclusion
This study showed significant differences in health parameter data in the standing desk group after the study period. The parameters of systolic and diastolic blood pressure as well as musculoskeletal discomfort proved statistically significant in the standing desk group. Nevertheless, there is a complexity of factors influencing health outcomes. Further research with larger sample sizes, longer intervention periods, and better control of confounding variables are needed to fully interpret the effects of standing desks on health parameters. Based on our findings, organizations should consider providing standing desks as an option for office workers to promote a more active work environment. Additionally, future studies should investigate the long-term use of standing desks and their effectiveness in reducing health issues associated with prolonged sitting.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Dr. Magdy Akladios, upon reasonable request.
References
-
Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, et al. (2015) Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med 162(2): 123-132. 2. Dunstan DW, Kingwell BA, Larsen R, Healy GN, Cerin E, et al. (2012) Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care 35(5): 976-983. 3. Parry SP, Coenen P, Shrestha N, O’Sullivan PB, Maher CG, et al. (2019) Workplace interventions for increasing standing or walking for decreasing musculoskeletal symptoms in sedentary workers. Cochrane Database Syst Rev 2019(11): CD012487. 4. Wilks S, Mortimer M, Nylén P (2006) The introduction of sit-stand worktables; aspects of attitudes, compliance and satisfaction. Appl Ergonom 37(3): 359-365. 5. Ma J, Ma D, Li Z, Kim H (2021) Effects of a Workplace Sit-Stand Desk Intervention on Health and Productivity. Int J Environ Res Public Health 18(21): 11604. 6. Amick BC, Robertson MM, DeRango K, Bazzani L, Moore A, et al. (2003) Effect of office ergonomics intervention on reducing musculoskeletal symptoms. Spine 28(24): 2706-2711. 7. David GC (2005) Ergonomic methods for assessing exposure to risk factors for work- related musculoskeletal disorders. Occup Med (Lond) 55(3): 190-199. 8. Niekerk SMV, Louw QA, Hillier S (2012) The effectiveness of a chair intervention in the workplace to reduce musculoskeletal symptoms. A systematic review. BMC Musculoskeletal Disord 13: 145. 9. Song Z, Baicker K (2019) Effect of a Workplace Wellness Program on Employee Health and Economic Outcomes: A Randomized Clinical Trial. JAMA 321(15): 1491-1501. 10. Hamberg-van Reenen HH, Beek AJVD, Blatter BM, Grinten MPVD, Mechelen WV, et al. (2008) Does musculoskeletal discomfort at work predict future musculoskeletal pain? Ergonomics 51(5): 637-648. 11. Parry S, Straker L (2013) The contribution of office work to sedentary behaviour associated risk. BMC Public Health 13: 296. 12. Rosenkranz SK, Mailey EL, Umansky E, Rosenkranz RR, Ablah E (2020) Workplace Sedentary Behavior and Productivity: A Cross- Sectional Study. Int J Environ Res Public Health 17(18): 6535.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30