Extramedullary Multiple Myeloma in the Kidney: A Case Report
Extramedullarymyeloma (EMM) is defined by the presence of plasma cells outside the bone marrow in a patient with multiple myeloma (MM). EMM is classified under four headings as bone-associated plasmacytoma, extramedullary disease (EMD), plasma cell leukemia and solitary plasmacytoma. EMD is more common in the nasopharynx, larynx, and upper respiratory tract. It is rarely seen in the kidney. We presented extramedullary disease of kidney, at relapsed myeloma patient.
Sinan Demircioğlu1* and Pembe Oltulu2
Hematology, Van Yüzüncü Yıl University, Turkey, Tel: 5554324474; Email:
sinandemircioglumd@gmail.com myeloma patient.
Keywords: Multiple Myeloma; Extramedullary Myeloma; Extramedullary disease
Introduction
Multiple myeloma (MM) is characterized by the proliferation of uncontrolled proliferating plasma cells, usually limited to the bone marrow. The extramedullary spread of MM may occur either during diagnosis or during the course of disease [1, 2]. Extramedullary myeloma (EMM) has been recently classified by being divided into four groups. There are 1-Bone-associated plasmacytoma, 2- Extramedullary disease (EMD) with a hematogenous spread that occurs in the tissues remote from the bone marrow, 3- Plasma cell leukemia, 4- Solitary plasmacytoma [3, 4, 5, 6]. It is necessary to demonstrate that the lesion is not associated with solitary plasmacytoma and bone to describe extramedullary disease [4].
Extramedullary disease and plasma cell leukemia have a worse course than the other 2 EMM subtypes. The presence of EMD in recurrence is associated with a survival of <6 months. This negative prognosis is less apparent in bone-associated EMM [7]. Prognosis is quite good after the treatment of solitary plasmacytoma with radiotherapy [8]. EMM is observed by around 6-8% during the first diagnosis of myeloma [9, 10]. The incidence of EMM increases in the course of the disease, and this ratio increases to 10-30% [3, 11].
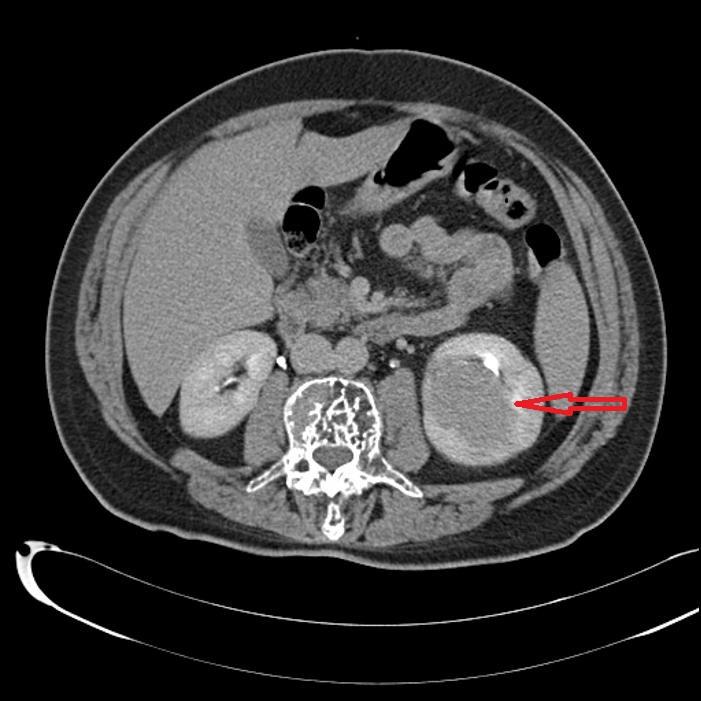
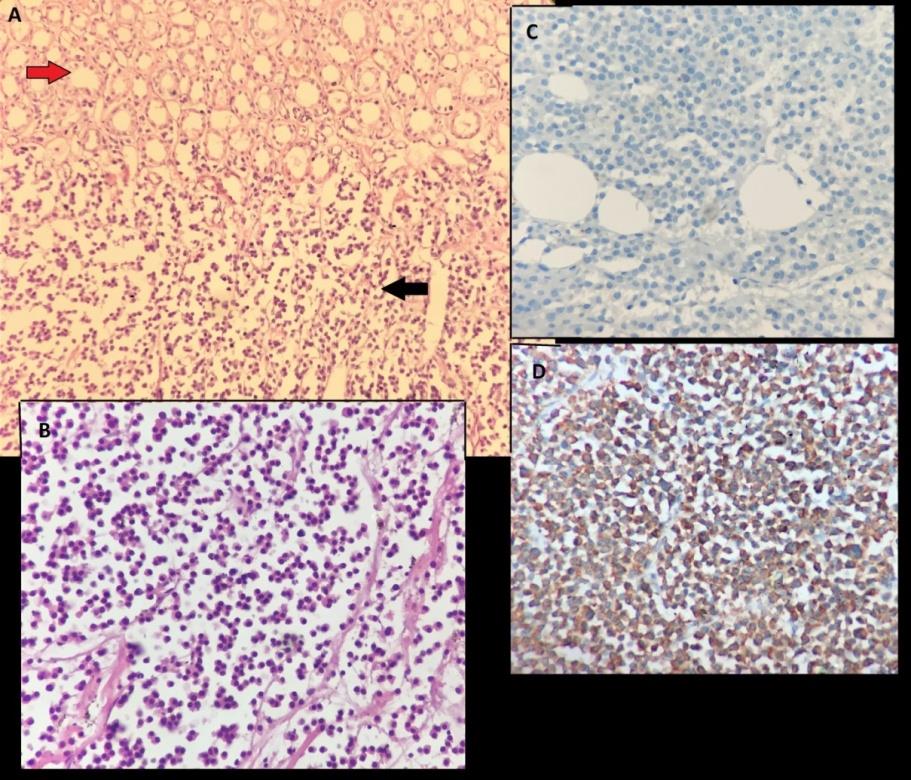
A 48-year-old male patient was diagnosed with multiple myeloma in 2005. He entered into remission after administering four cycles of VAD (vincristine- adriamycin-dexamethasone) chemotherapy, and radiotherapy to the thoracic region. He was followed up without medication since he did not accept the autologous stem cell transplantation. During the ultrasonography performed due to abdominal pain while being followed up in remission for ten years, a mass was detected in the left kidney. Dynamic renal tomography was performed. The lesion which was approximately 52 mm in diameter in the lower middle part of the left kidney and observed to be slightly hyperdense from kidney parenchyma, contrast- enhancing in the arterial phase, and wash out in the late phase in the portal phase in unenhanced images was radiologically interpreted as renal cell carcinoma (Figure 1). Then, left radical nephrectomy was performed. The surgical pathology was evaluated as a kappa-positive plasmacytoma. It was determined that the leukocyte count was 5800/mm3, hemoglobin value was11.6 g/dl, thrombocyte count was 263.000/mm3, immunoglobulins compressive, free kappa/lambda ratio was 5, and calcium and creatinine values were within normal limits. Monoclonal kappa light chain staining was observed in serum urine immunofixation. On PET CT, common lytic lesions were detected in the bone structure. Monoclonal plasma cell increase with kappa positive, lambda negative staining pattern was observed in bone marrow biopsy (Figure 2). Bortezomib, cyclophosphamide, dexamethasone chemotherapy, and zoledronic acid were initiated for the patient who was considered symptomatic MM.
Discussion and Conclusion
Although renal failure is observed in about half of the patients with multiple myeloma, extramedullary disease of the kidney is rarely observed [12]. EMD is more common in the nasopharynx, larynx, and upper respiratory tract [13]. Furthermore, it may also be observed in the gastrointestinal system, pleura, testis, skin, peritoneum, liver, brain, endocrine glands and lymph nodes [14, 15, 16, 17, 18, 19, 20, 21]. In the literature, plasmocytoma in the kidney has been reported less than 30 cases without multiple myeloma [22].
In the study carried out by Weinstock, et al. on 663 MM patients, the researchers detected EMD in 55 (8.3%) patients. While it was detected in the head and neck region (31.6%), abdomen (26.3%), chest (21.1%) and central nervous system (12%) during diagnosis, it was observed to be common in the abdomen (40%) and chest (23,9%) in recurrent disease. In abdominal involvement, it was common in pancreas, peritoneum, kidney, and intestines during diagnosis. In recurrent patients, liver involvement was most common in the abdomen [23]. In another study, EMD was detected in 42 (9%) of 467 patients. While EMD was most commonly observed in the soft tissue and pleura/peritoneum, kidney involvement was not encountered in this study. In this study, it was shown that the cumulative incidence of EMD in MM was 9%, and that treatment responses were poor in the presence of EMD. Furthermore, it was also shown that the survival of patients with simultaneous EMD during diagnosis was even worse [24].
In conclusion, along with the available information, EMD may occur in many different tissues as in our case. Although MM-associated renal failure is common, it is rarely seen in the kidneys in plasmacytoma. Plasmocytomas can be detected with imaging methods in MM patients.
References
-
Blade J, Lust JA, Kyle RA (1994) Immunoglobulin D multiple myeloma: presenting features, response to therapy, and survival in a series of 53 cases. J Clin Oncol 12(11): 2398-2404.
-
Blade J, Kyle RA, Greipp PR (1996) Presenting features and prognosis in 72 patients with multiple myeloma who were younger than 40 years. Br J Haematol 93(2): 345-351.
-
Blade J, Fernández de Larrea C, Rosiñol L, Cibeira MT, Jiménez R, et al. (2011) Soft-tissue plasmacytomas in multiple myeloma: incidence, mechanisms of extramedullary spread, and treatment approach. J Clin Oncol 29(28): 3805-3812.
-
Weinstock M, Ghobrial IM (2013) Extramedullary multiple myeloma. Leuk Lymphoma 54(6): 1135- 1141.
-
De Larrea CF, Rosiñol L, Cibeira MT, Rozman M, Rovira M, et al. (2010) Extensive soft-tissue involvement by plasmablastic myeloma arising from displaced humeral fractures. Eur J Haematol 85(5): 448-451.
-
Fernandez de Larrea C, Kyle RA, Durie BG, Ludwig H, Usmani S, et al. (2013) Plasma cell leukemia: consensus statement on diagnostic requirements, response criteria and treatment recommendations by the International Myeloma Working Group. Leukemia 27(4): 780-791.
-
Pour L, Sevcikova S, Greslikova H, Kupska R, Majkova P, et al. (2014) Soft-tissue extramedullary multiple myeloma prognosis is significantly worse in comparison to bone-related extramedullary relapse. Haematologica 99(2): 360-364.
-
Hadjiliadis D, Madill J, Chaparro C, Tsang A, Waddell TK, et al. (2005) Incidence and prevalence of diabetes mellitus in patients with cystic fibrosis undergoing lung transplantation before and after lung transplantation. Clin Transplant 19(6): 773-738.
-
Varettoni M, Corso A, Pica G, Mangiacavalli S, Pascutto C, et al. (2010) Incidence, presenting features and outcome of extramedullary disease in multiple myeloma: a longitudinal study on 1003 consecutive patients. Ann Oncol 21(2): 325-330.
-
Zamagni E, Patriarca F, Nanni C, Zannetti B, Englaro E, et al. (2011) Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood 118(23): 5989-5995.
-
Varga C, Xie W, Laubach J, Ghobrial IM, O'Donnell EK, et al., (2015) Development of extramedullary myeloma in the era of novel agents: no evidence of increased risk with lenalidomide-bortezomib combinations. Br J Haematol 169(6): 843-850.
-
Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, et al. (2003) Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc 78(1): 21-33.
-
Uppal HS, Harrison P (2001) Extramedullary plasmacytoma of the larynx presenting with upper airway obstruction in a patient with long-standing IgD myeloma. J Laryngol Otol 115(9): 745-746.
-
Chetty R, Bramdev A, Reddy AD (2003) Primary extramedullary plasmacytoma of the esophagus. Ann Diagn Pathol 7(3): 174-179.
-
Chim CS, Wong WM, Nicholls J, Chung LP, Liang R (2002) Extramedullary sites of involvement in hematologic malignancies: case 3. Hemorrhagic gastric plasmacytoma as the primary presentation in multiple myeloma. J Clin Oncol 20(1): 344-347.
-
Kintzer JS, Rosenow EC, Kyle RA (1978) Thoracic and pulmonary abnormalities in multiple myeloma, A review of 958 cases. Arch Intern Med 138(5): 727- 730.
-
Fernandez LA, Couban S, Sy R, Miller R (2001) An unusual presentation of extramedullary plasmacytoma occurring sequentially in the testis, subcutaneous tissue, and heart. Am J Hematol 67(3): 194-196.
-
Giuliani N, Caramatti C, Roti G, Geata A, Colla S, et al. (2003) Hematologic malignancies with extramedullary spread of disease. Case 1. Multiple myeloma with extramedullary involvement of the pleura and testes. J Clin Oncol 21(9): 1887-1888.
-
Green T1, Grant J, Pye R, Marcus R (1992) Multiple primary cutaneous plasmacytomas. Arch Dermatol 128(7): 962-965.
-
Demircioglu S, Aydogdu D, Ceneli O (2018) Expansion of a Myeloma-associated Lesion from Orbita to the Cerebrum. Turk J Haematol 35(1): 92-93.
-
Fujikata S, Tanji N, Aoki K, Ohoka H, Hojo N, et al. (2002) Extramedullary plasmacytoma arising from an adrenal gland. Urology 60(3): 514.
-
Lawrence BJ, Petersen EL, Riches WG, Pfeiffer DC (20018) Clinical Course of a Patient with Kidney Failure Due to Isolated Bilateral Renal Extramedullary Plasmacytomas. Am J Kidney Dis 6386(18): 30642-30645.
-
Weinstock M, Aljawai Y, Morgan EA, Laubach J, Gannon M, et al. (2015) Incidence and clinical features of extramedullary multiple myeloma in patients who underwent stem cell transplantation. Br J Haematol 169(6): 851-858.
-
Chen HF, Wu TQ, Li ZY, Shen HS, Tang JQ, et al. (2012) Extramedullary plasmacytoma in the presence of multiple myeloma: clinical correlates and prognostic relevance. Onco Targets Ther 5: 329-334.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies