Determining Transfusion Needs: Expectations and Realities?
Transfusion medicine (TM) is a vein-to-vein multidisciplinary bridging science and related practice,[1] comprising both procurement (manufacturing) and provision (supply) of safe and efficacious blood and blood products, as well as appropriate clinical application and related outcome (WHO, 1991) [2]. The need for safe blood and blood products is bedside-determined. The process is based on proper diagnosis, indication setting and decision making; including consideration of alternatives, knowledge and experience of benefits and risks of blood transfusion and above all a clear and understandable informed consent following explanation of the pros and cons of a transfusion intervention (supportive hemotherapy). Evidence-based TM is paramount to determine the ultimate need dynamically and accurately over time.
Commentary
Transfusion medicine (TM) is a vein-to-vein multidisciplinary bridging science and related practice,[1] comprising both procurement (manufacturing) and provision (supply) of safe and efficacious blood and blood products, as well as appropriate clinical application and related outcome (WHO, 1991) [2]. The need for safe blood and blood products is bedside-determined. The process is based on proper diagnosis, indication setting and decision making; including consideration of alternatives, knowledge and experience of benefits and risks of blood transfusion and above all a clear and understandable informed consent following explanation of the pros and cons of a transfusion intervention (supportive hemotherapy). Evidence-based TM is paramount to determine the ultimate need dynamically and accurately over time.
Reality
Unfortunately, most medical education curricula do not provide tailored transfusion medicine education, in particular in clinical application [3]. This leaves prescribing clinicians and registrars with a paucity of background knowledge to come to rational decision making when prescribing and transfusing blood. There is a distinct gap in communication between prescribers and suppliers (blood establishments). Hence, suppliers have no real idea of what the needs to supply are, how these develop over time, how to predict and anticipate to be able to accommodate evidence-based the ultimate customer the patient. Irrespective of the UNDP Human Development Index (HDI) state of development [4] there are only limited hospitals and supplying blood establishments that have established a well-functioning and properly managed clinical interface, operating as a well- designed bridge linking the health care consumer institute (hospital) firmly and sustainably to the care facilitating manufacturer (blood establishment). The consultative role of the supplier is seldom comprehensive and centred around Commentary the clinical problem.
Expectation
To generate attention and perception among blood prescribing clinicians the 1991 WHO definition deserves to allow the construction of a universal system to determine clinical needs to be met in a country. The clinical in-hospital transfusion chain has 3 elements (Figure 1)
- Diagnosis, indication, decision, informed consent and prescription (ordering; ward-bedside);
- Selection and compatibility testing (blood transfusion laboratory);
- Bedside patient identification and transfusion (ward- bedside practice) [5].
With the decision to transfuse, the expected outcome is defined. With transfusion of the selected blood or blood product, the outcome is observed allowing a benchmark for evidence-based practice (hemovigilance) and determining of realistic needs. The fast majority of clinical situations leading to a decision to transfuse are actually determined by a temporary need, a bridging of a relative shortage of circulating blood components, while metabolism gears up to compensate for the shortage; bone marrow and liver. This simple pathophysiologic phenomenon is often neglected while equally often clinicians tend to treat laboratory data rather than the patient expressing and presenting clinical symptomatology.
Without underestimating the importance of the procurement and provision part of the chain, the manufacturing of blood products for clinical consumption, determining of needs starts at the bedside; patients are transfused and not so much test tubes. Most ‘safe blood’ programs and projects are focused on technical procurement with a small element of provision. However, the clinical part is hardly ever addressed from inside hospitals and grossly neglected from supplier side. That illustrates the paucity of market principles within the transfusion medicine discipline. Documentation is paramount and competency of staff (knowledge and skills) involved instrumental to implementation, where a well-developed supplier-consumer relationship (marketing) will lead to ultimate success. In other words, a well-designed and actively implemented vein-to-vein Quality System Management and a quality culture environment form the fundament for a realistic determination of the real need demonstrating the reality as benchmarked against the expectation; evidence-based [6].
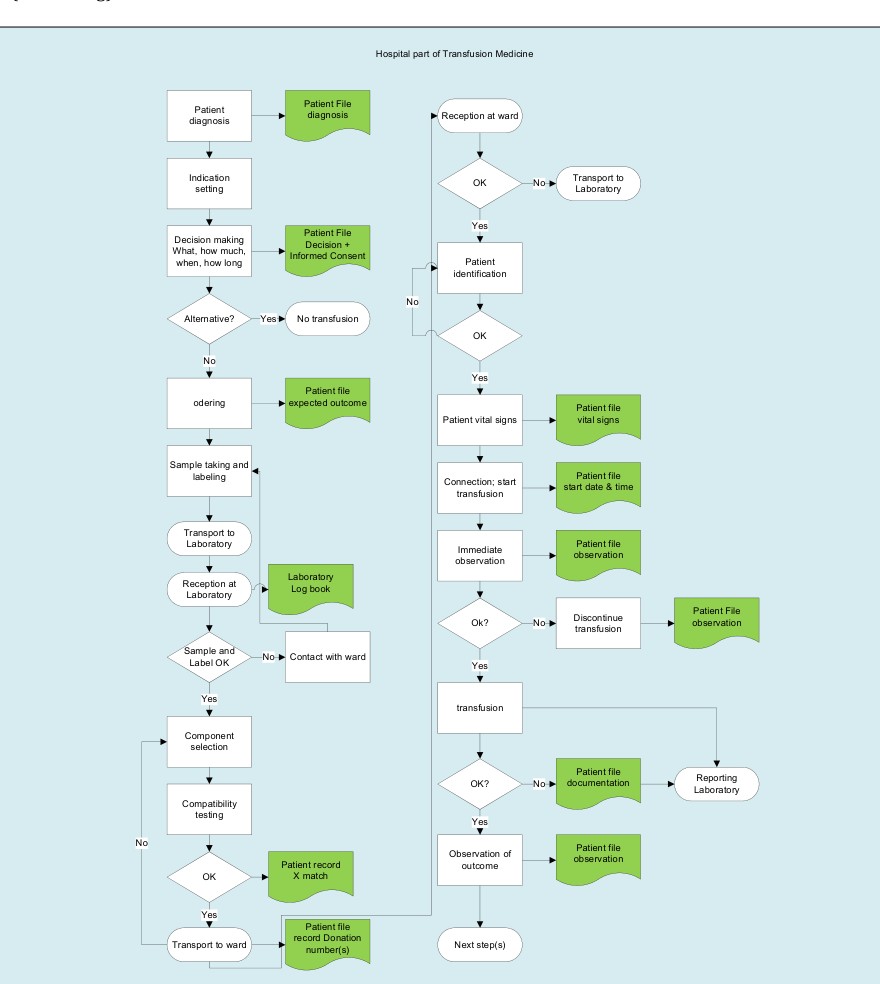
Figure 1: In-Hospital process of blood transfusion. The 12 green symbols represent documentation. The 7 diamond symbols are decision or critical control points (CCP). First three green documentation symbols represent the first element of the process – ordering (bedside/expectation); the second three represent the selection (laboratory); the last six represent the ultimate bedside transfusion element (reality). Of the 7 critical control points, there is one in de ordering element – ‘are there alternatives available?’; two in the selection element: ‘are request, sample and label traceable?’; the last four are essential for the transfusion evidence: ‘is the right patient receiving the right blood product?’.
| N | o |
|---|
The WHO Global Status Report on Blood Safety and Availability 2016 [7] and recent literature and surveys illustrate the magnitude of the gap.[8, 9, 10] More recently this has been translated by WHO in a global action framework to advance access to safe, effective and quality-assured blood products 2020-2023 [11].
Conclusion
In the development of a safe and sustainable blood supply and transfusion system, there is an urgent need to reverse some of the current laboratory oriented approaches. Based on the WHO initiatives [11, 12] a general road map could be developed with the following elements: a) Mutual respect and confidence (clinical interface, Hospital Transfusion Committee); b) In-hospital awareness and culture to prescribe, select and transfuse within the setting of a hospital transfusion policy and evidence-based clinical guidelines drafted and endorsed by clinicians (documentation, hemovigilance); c) In-hospital transfusion practice-based quality system to be managed by all staff involved – clinicians, nurses, technicians and others (patient blood management); d) Appropriate and continued education in clinical use of blood and blood products (Continuous Professional Development and Continuous Medical Education).
Such road map justifies the expectation that for the future an evidence-based and accurate determining of transfusion needs will become reality.
References
-
Smit Sibinga CTh, Abdella YE (2018) Transfusion Medicine-a bridging science. Intern Med Rev 4: 1-30.
-
Report of the WHO Global Blood Safety Initiative (GBSI) Informal Consultation on ‘Collaboration in Training in Transfusion Medicine’ 23-27 September 1991, Geneva, CH.
-
Al-Riyami AZ, Louw VJ, Indrikovs A, Nedelcu E, Bakhtary S, et al. (2020) Global Survey on Transfusion Medicine Curricula in Medical Schools-Challenges and Opportunities. Transfusion (accepted).
-
(2018) UNDP Human Development Indices and Indicators. 2018 Statistical Update, New York.
-
Murphy ME, Saxena S, Smit Sibinga CTh (2013) Patient Safety and Quality Management at the Clinical Interface. In: Smit Sibinga CTh (Eds.), Quality Management in Transfusion Medicine, Nova Science Publ, New York, pp: 283-314.
-
Smit Sibinga CTh, Hasan F (2020) Quality Management or the Need for a Quality Culture in Transfusion Medicine. Glob J Transfus Med 5(1): 9-16.
-
(2016) Global Status Report on Blood Safety and Availability, WHO, Geneva.
-
Gallagher Swann M, Ingleby B, Cole C, Barr A (2011) Improving transfusion practice: ongoing education and audit at two tertiary speciality hospitals in Western Australia. Transfus Med 21(1): 51-56.
-
Graham J, Grant Casey J, Alston R, Baker P, Pendry K (2014) Assessing transfusion competency in junior doctors: a retrospective cohort study. Transfusion 54(1): 128-136.
-
Duguid J, Copplestone JA (2008) Teaching transfusion in UK medical schools: a survey by the National Blood Transfusion Committee. Med Educ 42(4): 439.
-
(2020) Action framework to advance universal access to safe, effective and quality-assured blood products 2020- 2023. Geneva, CH: World Health Organization.
-
(2017) Strategic framework for blood safety and availability 2016-2025. Cairo, Egypt: WHO Regional Office for the Eastern Mediterranean.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies