Long-Term Rather than Short-Term Survival Benefit in Mantle Cell Lymphoma Patients Treated With Intensive ChemoImmunotherapy and Hematopoietic Stem Cell Transplantation in Real World Experience
Purpose: Mantle cell lymphoma is an aggressive B cell lymphoma with initially responded but easy to relapse and difficult to cure without survival plateau. The present recommendation of treatment includes induction chemo-immunotherapy followed by high dose chemotherapy plus autologous hematopoietic stem cell transplantation for transplant-eligible patients and chemoimmunotherapy followed by rituximab maintenance for transplant-ineligible patients. However, the best induction regimen remains to be defined and median five-year overall survival is around 60% on phase II trials of multi-center experiences. Materials & Methods: We investigated the real world outcome of our patients undergoing different regimens of induction chemo-immunotherapy and analyzed whether the intensity of treatment as one of prognostic factors upon the impact of survival. Results: Between 1997 and 2018, we analyzed 50 patients as the cohort with median age 62 (range 34 to 77), and male to female was 40 versus 10. Advanced stage of diseases were 86% (stage III 10% and stage IV 76%) of all patients. Ki-67 more than 30% of lymphomas were seen in 50% of patients and 34% with Ki-67 less than 30% and 16% were unknown. Thirty-four per cents of patients underwent intensive induction chemo-immunotherapy with or without ASCT and 66% received nonintensive treatment. Six of 31 relapsed patients had undergone allogeneic hematopoietic stem cell transplantation. Five-year overall survival was 52% with median OS 5.15 years. There was no significant survival difference between intensive versus non-intensive induction therapy with 53% versus 46% in first 5 years, however, better overall survival was seen in intensive therapy group when follow up longer. High Ki-67 patients had shorter 5-year overall survival (37% vs 63%). Transplant patients had better overall survival with 68% vs 47% in 5 years with median OS 10.86 vs 4.34 years. Conclusion: There was no statistically significant difference of survival during the initial five years but intensive induction chemo-immunotherapy with or without HDC/ASCT could achieve better survival in longer follow-up according to our real world experience.
Introduction
Mantle cell lymphoma is one of aggressive B cell lymphoma and most patients presented in advanced stage of disease with bone marrow or peripheral blood involvement, characterized by chemo-sensitive initially but easy to relapse and poor long term survival. Phase II and randomized phase III studies showed improved outcome after the addition of rituximab and more intensive chemotherapy, e.g. high dose cytarabine containing regimen during induction therapy [1]. Besides, rituximab maintenance for 2 years or more could improve event free survival, progression free survival, and overall survival after induction immuno-chemotherapy in transplant-ineligible elderly patients in European multicenter study [2] and in transplant-eligible patients in French experience [3]. As a result, the standard recommendation of treatment includes intensive induction chemo-immunotherapy followed by high dose chemotherapy and autologous hematopoietic stem cell transplantation (HDC/ASCT) followed by rituximab maintenance for transplant-eligible patients, which may improve the progression free and overall survival but still cannot cure the disease. However, the median age of mantle cell lymphoma patients is older than 60s and more than half of them cannot tolerate intensive induction therapy or even HDC/ASCT. As a result, most elderly or unfit patients just received conventional dose of R-CHOP, R-CVP, or R-FC, with or without rituximab maintenance [4]. An early report from European MCL network showed even early consolidation by myeloablative radio-chemotherapy followed by autologous hematopoietic stem cell transplantation in first remission could significantly prolong progression-free survival but not significantly improved overall survival in initially 3 years follow-up [5]. Therefore, we retrospectively review our real world data to compare the long-term outcome of intensive induction chemo-immunotherapy plus/minus consolidation HDC/ASCT versus non-intensive chemo-immunotherapy in the treatment of mantle cell lymphoma patients.
Methods
We had consecutive 65 mantle cell lymphoma patients between 1997 and 2018 and excluded 15 unevaluable patients and there were 50 patients in our cohort, which was 3% of all our lymphoma patients. Whether patients underwent intensive or non-intensive chemo-immunotherapy was according to patient age and co-morbid association and at the discretion of treating physicians. Intensive regimen included R-Hyper-CVAD, R-CHOP/R-DHAP, VR-CAP/VR-DHAP followed by HDC/ASCT; non-intensive regimen included R-CHOP, R-CVP, or VR-CAP. The primary efficacy end points were PFS after the completion of treatment. The secondary end point was OS. The Kaplan–Meier method and log-rank test were used to compare PFS and OS rates of either Ki-67 higher or lower than 30%, early or late stages of disease, intensity of induction therapy, and HSCT or not in these patients. All p values < 0.05 were considered significant.
Results
Fifty patients were analyzed and the patients demographic seen in Table 1. Median age was 62 (range 34 to 77) and 40 were male and 10 female patients (M/F 80% vs 20%) with advanced stage in 86% (stage III 10% and stage IV 76%). Ki-67 higher than 30% was in 25 patients (50% of all) and lower than 30% in 17 (34%) and 8 (16%) were unavailable. Seventeen patients were alive and free of disease over 10-year follow-up. Seventeen patients (34% of all) received intensive induction therapy including 5 received frontline high dose chemotherapy and autologous HSCT as consolidation. For 31 patients underwent salvage therapy on relapse of disease, 6 of them underwent allogeneic HSCT.
| Total | % | Total | % | ||
|---|---|---|---|---|---|
| Mantle Cell Lymphoma pts. | 50 | 100% | Mantle Cell Lymphoma pts. | 50 | 100% |
| Sex | Mortality | ||||
| Female | 10 | 20% | Alive | 17 | 34% |
| Male | 40 | 80% | Death | 33 | 66% |
| Age | Cause of Death | ||||
| Mean/Median/Range | 60/62/34-77 | Disease relapse | 21 | 64% | |
| Stage | GVHD+infection | 1 | 3% | ||
| II | 4 | 8% | Pneumonia | 1 | 3% |
| III | 5 | 10% | Suicide but disease free | 1 | 3% |
| IV | 38 | 76% | Hepatic failure | 1 | 3% |
| X | 3 | 6% | Unknown | 8 | 24% |
| Ki_67 | |||||
| <30% | 17 | 34% | |||
| >=30% | 25 | 50% | |||
| X | 8 | 16% |
Table 1: Demographic of 50 mantle cell lymphoma patients in KF-SYSCC.
Data source: Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Table 1: Demographic of 50 mantle cell lymphoma patients in KF-SYSCC.
Overall survival of all patients were 52% at 5 years and 31% at 10 years with median overall survival 5.15 years (Figure 1) and non-stage IV disease of patients had better survival as compared with stage IV patients with median
10.86 years versus 4.34 years (Figure 2). Patients with lower Ki-67 had marginal better overall survival but no difference in progression free survival (Figures 3A and 3B).
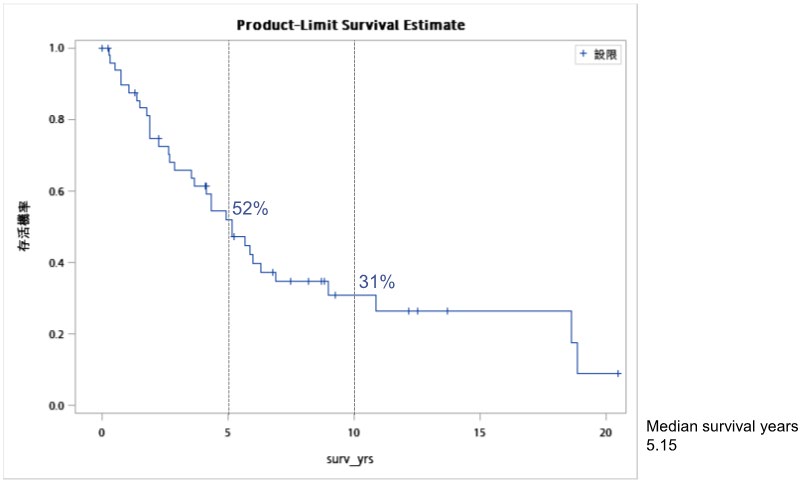
Data source: Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 1: Overall survival of 50 patients of mantle cell lymphoma.
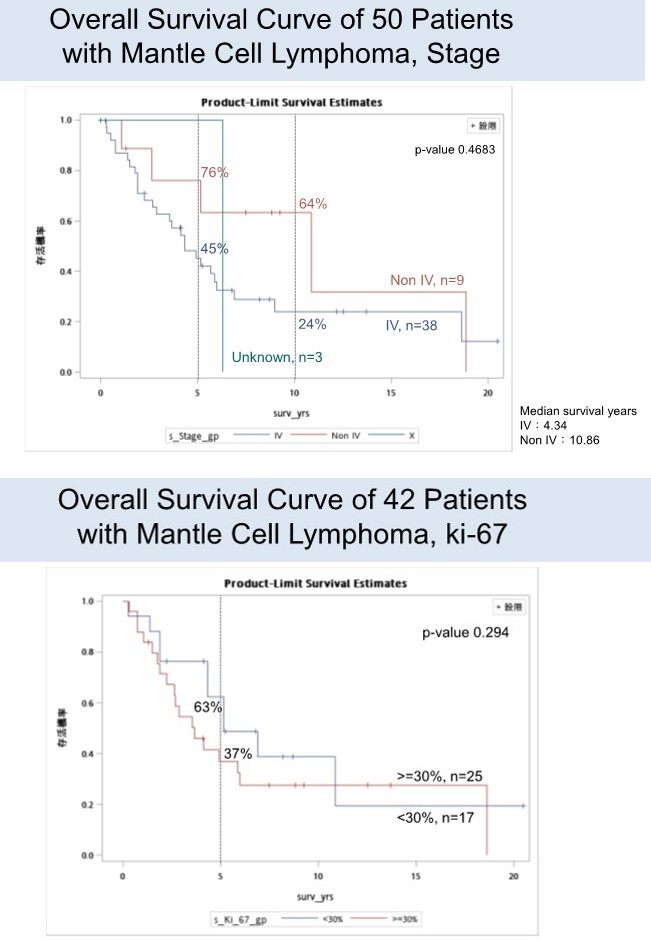
Data source: Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 2: Overall survival of patients according to stages, non-stage versus stage IV disease of patients.
Data source: Exclude Missing value. Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 3A: Overall survival of patients according to Ki-67.
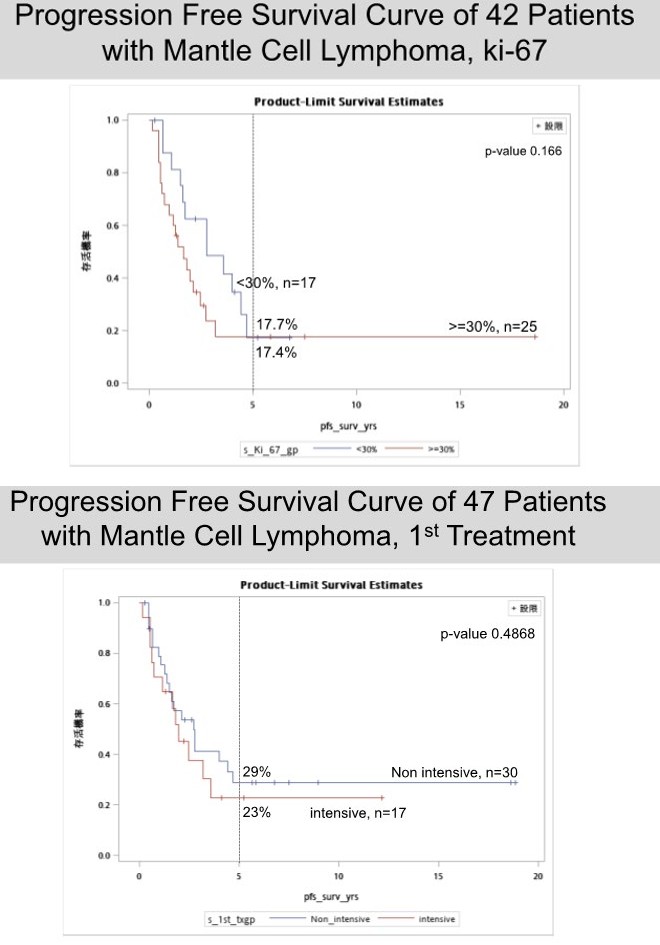
Data source: Exclude Missing value. Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 3B: Progression free survival of patients according to Ki-67.
On account of intensity of induction therapy, there is no difference in progression free survival (Figure 4A) and overall survival during the initial 5 years, however, there was trend to have better overall survival after 5 years (Figure
4B). For patients who had undergone hematopoietic stem cell transplantation, there was better median overall survival with 10.86 years versus 4.34 years (Figure 5).
Data source: Exclude Missing value. Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 4A: Outcome of patients underwent intensive versus non-intensive induction chemo-immunotherapy in terms of PFS.
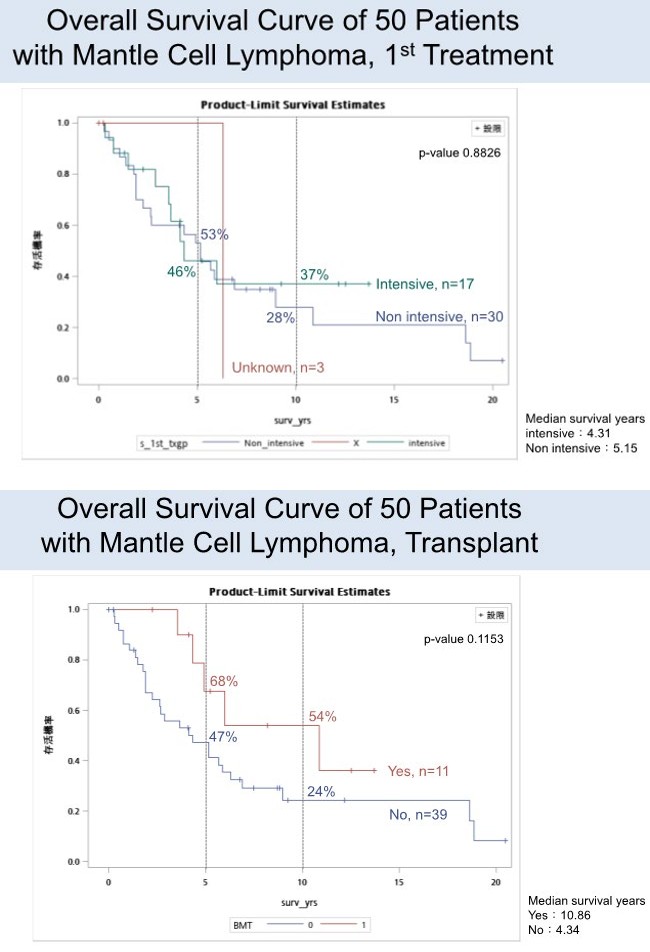
Data source: Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 4-B: Outcome of patients underwent intensive versus non-intensive induction chemo-immunotherapy in terms of OS.
Data source: Patient’s last follow-up date: KF-SYSCC HIS data updated on December 13, 2019. Taiwan mortality data updated by December 31, 2018, received on September 2019. Figure 5: Overall survival of patients received HSCT versus no transplant.
Thirty-three patients passed away with twenty one patients died of relapse of disease (64%), one died of GVHD after salvage allogeneic HSCT (3%), one died of pneumonia (3%), one died of fulminant hepatic failure due to hepatitis B reactivation (3%), and one committed suicide because of extensive chronic GVHD (3%), and 8 patients were unknown about causes of death (24%).
Discussion
We know that mantle cell lymphoma is a heterogenous group of disease with a variety of clinical manifestations and Abrisqueta reported that 17% can be smoldering nodal/ extra-nodal or asymptomatic non-blastoid leukemic non- nodal manifestation and these clinical variants generally do not need immediate systemic treatment and watchful observation is safely pursued [6]. In their series, median time to treatment was 35 months (range 5-79 months). On the other hand, most MCL patients presented with symptomatic lymphadenopathy or symptomatic extra-nodal disease requiring systemic therapy as soon as possible.
Currently, MCL patients classified by MIPI risk score or simplified MIPI score based on variables of age, LDH, leukocyte count, and ECOG performance status. The prognostic value of the simplified MIPI score is further improved by adding the percentage of Ki-67 (obtained from lymphoma-rich areas on non-bone marrow involved tissue biopsies) which is also called biologic MIPI [7]. But is it time to risk-stratify treatment based on the proliferative signature? Despite being widely used in scientific studies, Ki- 67 biomarkers based on standard IHC techniques suffer from poor reproducibility, challenging the use of these techniques for clinical decision making and most of the interobserver variability might be due to the varying procedure of analysis [8]. As a matter of fact, in our cohort, there is just borderline better outcome but no statistically significant difference in terms of progression free survival and overall survival between below and above 30% of Ki-67. Dreyling proposed a tailored therapeutic approach and limited consolidation high dose chemotherapy and autologous stem cell transplantation in younger and fit with high Ki-67 patients and maintenance therapy for MRD+ patients but needs longer follow-up to see the benefit.
As we know, it is difficult to cure mantle cell lymphoma, even complete remission achieved after induction chemo- immunotherapy with or without consolidation high dose chemotherapy plus hematopoietic stem cell transplantation, there was still no plateau of survival curve seen in the literature reports. Despite initial NORDIC MCL-2 trial, as compared with MCL-1, the event-free, overall, progression-free survival, the duration of molecular remission, and the proportion of PCR-negative stem cell products were significantly improved and may lead to long-term progression-free survival and perhaps cure [9], however, the 15-year updated results after a median follow-up of 11.4 years, they observed a continuous pattern of relapse and the survival curves never reached a plateau even among patients experiencing long remissions [10]. In our real world experience, median overall survival was 5.15 years but up to 10.86 years in transplant group of patients, quite similar to 12.7 years in MCL-2 trial and 34% in our patients were still in disease free and alive on over 10- year of follow-up, similar to 40% in Nordic study. Besides, the intensive induction therapy and HDC/ASCT related survival benefit was not seen until 5 years after the finish of treatment.
According to the prior experiences of treatment, the inclusion of more intensive chemotherapy and CD20 monoclonal antibody could achieve better overall and complete response, remission duration, and overall survival. For example, the addition of high dose methotrexate and high dose cytarabine in MD Anderson’s Hyper-CVAD/MA is better than conventional CHOP chemotherapy and the high dose cytarabine alone could have better outcome proven in MCL-2 trial, as compared in MCL-1 trial [1, 9]. According to North America experience, R-DHAP alternating with R-CHOP followed by HDC/ASCT or R-Hyper-CAVD is better than R-CHOP followed by HDC/ASCT. French LYSA group reported just 4 cycles of induction R-DHAP rather than alternating R-CHOP/R-DHAP, followed by R-BEAM plus ASCT could achieve good outcome [3].
The choice of aggressive induction therapy recommended by NCCN treatment guideline includes CALGB regimen (augmented CHOP plus methotrexate, etoposide, and cytarabine), Hyper-CVAD (augmented CHOP plus high dose methotrexate and high dose cytarabine), NORDIC regimen (augmented CHOP plus high dose cytarabine), sequential R-CHOP/R-DHAP, or R-CHOP/R-ICE. But what is the best induction regimen and how intensive is adequately intensive? Widmer from Zurich reported in 20 years of a single center experience showed with a mean follow-up of 5.7 years, 10-year progression-free survival for all patients was 32% and overall survival was 76%, with no difference between R-hyper-CVAD/MA and R-CHOP /cytarabine groups [11]. However, complication-induced hospitalization rate, hematological toxicity and economic burden were significantly higher in the R-hyper-CVAD/MA treatment group.
Interestingly, a recent report from North American S1106 study [12] to compare R-hyper-CVAD and R-bendamustine in transplant-eligible mantle cell lymphoma patients and five-year follow-up demonstrated similar efficacy, MRD negativity, and 5-year survival between these two groups but R-hyper-CVAD was more toxic than R-bendamustine, besides, R-hyper-CVAD had higher stem cell mobilization failure rate and prompted protocol-specified early study closure [13]. From the result of SWOG S1106 study, we can realize that under more intensive induction therapy, there is no guarantee to always have better outcome. By the way, we know the less intensive chemo-immunotherapy R-BAC (rituximab, bendamustine, and cytarabine) for elderly mantle cell lymphoma patients to have 74% of disease free survival after a median follow-up of 35 months even cytarabine dosage reduced from 2400 mg/m2 to 1500 mg/m2 [14, 15].
Another recent report from Dana-Farber Cancer Institute and Washington University at St. Louis also used less intensive induction chemo-immunotherapy with alternating rituximab/bendamustine and rituximab/ cytarabine followed by high dose chemotherapy and autologous hematopoietic stem cell transplantation [16], which showed RB/RC induction followed by ASCT is well tolerated overall with 92% of patients completed induction and 84% underwent planned consolidative ASCT and the end-of-induction overall and complete response rates were 97% and 90%, respectively and 3-year progression-free survival and overall survival were 83% and 92%, respectively, better than the result of SWOG S1106 trial which devoid of high dose cytarabine during induction and not inferior or even superior to R-Hyper-CVAD/MA induction. Interestingly, the sequential RB/RC rather than alternating induction treatment had better outcome in their comparison. The median age of patients with mantle cell lymphoma is 65 years old and most of them cannot enroll intensive chemo-immunotherapy or even high dose chemotherapy and autologous hematopoietic stem cell transplantation and less intensive induction therapy like R-BAC regimen is mandatory for those elderly, unfit, and transplant-ineligible patients; in addition, R-CHOP rather than R-FC followed by rituximab maintenance or even longer period of maintenance is an option as well [4]. Besides, other novel therapy such as Bortezomib containing (VR-CAP vs R-CHOP) [17] could achieve 24 months of median progression free survival, and chemo-free regimen e.g. lenalidomide plus rituximab as induction and maintenance can achieve durable MRD- negative complete remission and 64% of 5-year progression free survival [18].
Ibrutinib and venetoclax are both very effective targeted salvage therapy for relapsed refractory mantle cell lymphoma [19] and is it possible to add on or even replace chemotherapy with targeted therapy during induction? Wang and Jain reported phase II trial with ibrutinib plus rituximab combination alone for newly diagnosed MCL older than 65 years or the same regimen followed by short course of R-Hyper-CVAD/MTX for younger than 65 years patients [20, 21] with overall response rate close to 100% and complete response rate 60~88% and median PFS/OS were not reached on 22~28 months of follow up.
Conclusion
In summary, in the induction phase of MCL treatment, the strongest R-Hyper-CVAD is no more meant to translate to better outcome, R-Maxi-CHOP plus high dose cytarabine is no more meant to have survival plateau which indicated cure either. On the contrary, R-CHOP is inferior to VR-CAP, and there was similar efficacy between R-CHOP/R-DHAP and R-DHAP alone. Whether an effective but a little stronger enough e.g. bendamustine and high dose cytarabine based therapy may be more effective and less toxic for patients. Coming to the age of targeted therapy for mantle cell lymphoma, does patients still need autologous hematopoietic stem cell transplantation? That would be answered by the Triangle trial of European MCL Network [22] about whether ibrutinib added on R-CHOP/R-DHAP induction followed by 2 years of ibrutinib maintenance could eliminate the role of ASCT and we hope that next generation novel therapy could achieve not only better outcome but also less toxicity for our patients.
References
-
Hermine O, Hoster E, Walewski J, Bosly A, Stilgenbauer S, et al. (2016) Addition of high-dose cytarabine to immune-chemotherapy before autologous stem-cell transplantation in patients aged 65 years or younger with mantle cell lymphoma (MCL Younger): a randomized, open-label, phase 3 trial of the European Mantle Cell Lymphoma Network. Lancet 388(10044): 565-575.
-
Kluin Nelemans HC, Hoster E, Hermine O, Walewski J, Trneny M, et al. (2012) Treatment of older patients with mantle cell lymphoma. N Engl J Med 367: 520-531.
-
Le Gouill S, Thieblemont C, Oberic L, Moreau A, Bouabdallah K, et al. (2017) Rituximab after autologous stem-cell transplantation in mantle-cell lymphoma. N Engl J Med 377: 1250-1260.
-
Kluin Nelemans HC, Hoster E, Hermine O, Walewski J, Geislern CH, et al. (2019) Treatment of older patients with mantle cell lymphoma (MCL): long-term follow-up of the randomized European MCL Elderly trial. J Clinical Oncology 38(3): 248-256.
-
Dreyling M, Lenz G, Hoster E, Van Hoof A, Gisselbrecht C, et al. (2005) Early consolidation by myeloablative radio-chemotherapy followed by autologous stem cell transplantation in first remission significantly prolongs progression-free survival in mantle-cell lymphoma: results of a prospective randomized trial of the European MCL Network. Blood 105(7): 2677-2684.
-
Abrisqueta P, Scott DW, Slack GW, Steidl C, Mottok A, et al. (2017) Observation as the initial management strategy in patients with mantle cell lymphoma. Annals of Oncology 28(10): 2489-2495.
-
Jain P, Wang M (2019) Mantle cell lymphoma: 2019 update on the diagnosis, pathogenesis, prognostication, and management. Am J Hematol 94(6): 710-725.
-
Eskelund CW, Kolstad A, Jerkeman M, Raty R, Laurell A, et al. (2016) 15-year follow-up of the Second Nordic Mantle Cell Lymphoma trial (MCL2): prolonged remissions without survival plateau. British Journal of Hematology 175(3): 410-418.
-
Geisler CH, Kolstad A, Laurell A, Andersen NS, Pedersen LB, et al. (2008) Long-term progression-free survival of mantle cell lymphoma after intensive front-line immune- chemotherapy with in vivo-purged stem cell rescue: a nonrandomized phase 2 multicenter study by the Nordic Lymphoma Group. Blood 112(7): 2687-2693.
-
Dreyling M, Ferrero S, Vogt N, Klapper W (2014) New paradigms in mantle cell lymphoma: is it time to risk- stratify treatment based on the proliferative signature? Clin Cancer Res 20(20): 5194-5206.
-
Widmer F, Balabanov S, Soldini D, Samaras P, Gerber B, et al. (2018) R-hyper-CVAD versus R-CHOP/cytarabine with high-dose therapy and autologous hematopoietic stem cell support in fit patients with mantle cell lymphoma: 20 years of single-center experience. Ann Hematol 97(2): 277-287.
-
Kamdar M, Li H, Chen RW, Rimsza LM, Leblanc ML, et al. (2019) Five-year outcomes of the S1106 study of R-hyper-CVAD vs R-bendamustine in transplant-eligible patients with mantle cell lymphoma. Blood Advance 3(20): 3132-3135.
-
Chen RW, Li H, Bernstein SH, Kahwash S, Rimsza LM, et al. (2017) RB but not R-HCVAD is a feasible induction regimen prior to auto-HCT in frontline MCL: results of SWOG Study S1106. Br J Haematol 176(5): 759-769.
-
Visco C, Finotto S, Zambello R, Paolini R, Menin A, et al. (2013) Combination of rituximab, bendamustine, and cytarabine for patients with mantle-cell non- Hodgkin lymphoma ineligible for intensive regimens or autologous transplantation. J Clin Oncol 31(11): 1442- 1449.
-
Visco C, Chiappella A, Nassi L, Patti C, Ferrero S, et al. (2017) Rituximab, bendamustine, and low-dose cytarabine as induction therapy in elderly patients with mantle cell lymphoma: a multicenter phase 2 trial from Fondazione Italiana Linfomi. Lancet Haematol 4(1): 15- 23.
-
Merryman RW, Edwin N, Redd R, Bsat J, Chase M, et al. (2020) Rituximab/bendamustine and rituximab/ cytarabine induction therapy for transplant-eligible mantle cell lymphoma. Blood Advance 4(5): 858-867.
-
Robak T, Huang H, Jin J, Zhu J, Liu T, et al. (2015) Bortezomib-based therapy for newly diagnosed mantle- cell lymphoma. N Engl J Med 372(10): 944-953.
-
Ruan J, Martin P, Christos P, Cerchietti L, Tam W, et al. (2018) Five-year follow-up of lenalidomide plus rituximab as initial treatment of mantle cell lymphoma. Blood 132(19): 2016-2025.
-
Tam CS, Anderson MA, Pott C, Agarwal R, Handunnetti S, et al. (2018) Ibrutinib plus venetoclax for the treatment of mantle-cell lymphoma. N Engl J Med 378(13): 1211- 1223.
-
Wang M, Jain P, Lee HJ, Hagemeister FB, Samaniego F, et al. (2019) Frontline treatment with ibrutinib plus rituximab (IR), until CR or 12 cycles maximally, followed by short course R-Hyper-CVAD/MTX x 4 cycles is extremely potent and safe in patients (age<65 years) with MCL – results of phase II Window-1 clinical trial. Blood 134(1).
-
Jain P, Lee HJ, Steiner RE, Hagemeister FB, Westin JR, et al. (2019) Frontline treatment with ibrutinib with rituximab (IR) combination is highly effective in elderly (>65 years) patients with MCL–results from a phase II trial. Blood 134(1).
-
Dreyling M, Ferrero S (2016) The role of targeted treatment in mantle cell lymphoma: is transplant dead or alive? Haematologica 101(2): 104-114.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies