Haematological Profile in COVID-19 Infection
In COVID-19 transitory and reversible perturbation of myelopoeisis and granulopoiesis is disordered. Characteristic changes on peripheral blood smear can help in diagnosis, may be in prognosis and treatment protocols. Decrease in lymphocyte count and increase in the neutrophilic lymphocytic ratio (NLR ratio) are the obvious abnormalities detected. Coronovirus mainly affects lungs as most of the ACE-2 receptors are present in lung. Corona has S spikes which helps in attaching it to the ACE -2 Receptor mainly affecting the type II pneumocytes causing capillary leakage and alveolar edema leading to breathing difficulty. COVID-19 is a global pandemic more research is required for prognostication, treatment and diagnostic protocols as disease was an unknown entity before its occurrence.
Introduction
Coronaviruses family of viruses causes human illness and animal illness. In human beings, various coronaviruses are well known to cause respiratory infections stretching from common cold to Middle East Respiratory Syndrome (MERS), Severe Acute Respiratory Syndrome (SARS). The most recently discovered coronavirus causes coronavirus disease COVID-19 named SARS Cov-2. This virus was an unknown entity before the outbreak that occurred in Wuhan sea food market in China the outbreak transpired in 2019 December. COVID-19 is now a pandemic affecting many countries globally [1].
COVID-19 infection is a systemic disease affecting respiratory system, and other systems such as cardiovascular, Commentary neurological, haematopoietic, gastrointestinal and immune. Here we summarize the hematologic findings on full blood count focusing more on leukocytes and thrombocytes analysing their utilization for identifying the patients more prone for a progression of the severe disease. Studies proved that surveillance of these hematologic parameters can help to recognize subjects who may require specialised care [2].
Many studies had shown that patients who were COVID-19 positive by RT-PCR, on admission blood picture showed lymphocytopenia, thrombocytopenia and leukopenia. Lymphopenia which was defined as a lymphocyte count of less than 1500 mm3). A study by Singh, et al. showed that ACE2 receptors were expressed in lymphocytes in lungs and digestive system. The direct cytopathic effect of the virus on the lymphocytes can lead to their lysis. So, lymphocytopenia is a powerful predictor for disease severity [2].
Thrombocytopenia was defined as a platelet count of less than 150,000 mm3 was also seen in 30% of the COVID-19 positive patients. Subjects having COVID-19 infection induced thrombocytopenia had elevated D-dimer levels & impaired coagulation profile more prone to develop to thrombosis leading disseminated intravascular coagulation. The reason for thrombosis is as there is capillary fluid leakage to interstitial oedema and finally alveolar oedema. The cellular content is more in the capillaries as the fluid portion is moving out leading to increased chances of thrombosis [2].
Regarding Leukopenia (WBC less than 4000 mm3), it was evident in 20% patients. Mostly Neutrophilia was observed in 90% of positive patients. The reason for neutrophilia as suggested by literatures is because of the cytokine storm. Cytokine storm includes release of cytokines particularly IL-6, IL-1. As the Coronavirus binds to ACE-2 receptors on type II pneumocytes and utilizes ribosomes and RdRp (RNA dependent RNA polymerase) for its proliferation when it is attaching to ACE-2 Receptor it release cytokines particularly IL-6 leading to cytokine storm and after attaching to ACE-2 receptors it induce more neutrophils could be one reason for neutrophilia. The increase of neutrophils accounts for decrease in other white blood cells (WBC’s) such as lymphocytes, monocytes and eosinophils) [3].
In one study it was noted that patients who were admitted in ICU had significant neutrophilia during their hospitalization as compared to patients admitted in Non- ICU group. Neutrophil-to-lymphocyte ratio (NLR), platelet- to-lymphocyte ratio (PLR) can be utilized for assessing the magnitude of systemic inflammation. Few studies on eosinophils showed that most critically ill patients had decreased absolute eosinophil counts (normal range (absolute eosinophil counts 40-440). Eosinophil levels improved in all patients at the time of discharge this suggests that eosinopenia resolving can be an indicator of improving clinical condition. In critically ill patients, flow cytometry showed decreased counts of lymphocyte, CD3+ T cell, CD4+ T cell and CD8+ T cells respectively in compairson with mild patients [4].
The studies clearly demarcate the patients, having severe disease, tends to have more profound abnormalities in comparison with mild disease patients. All the studies advocates that leukocyte count with differential count should be examined on a regular basis as these markers play a role in effectual triaging of the patients on admission and also during their hospitalization [5] (Figures 1-5).
Peripheral blood smear in COVID Positive patients shows neutrophilic changes, Figure 1a) shows projections in nucleus; Figure 1b) shows toxic granulations and vacuolations; Figure 1c) shows elongated nucleus; Figure 1d) shows foetus like shaped nucleus; Figure 1e) shows ring shaped nucleus [2].
Figure 1A: Nuclear Projections.
Figure 1B: Toxic Granulations and Vacuolation.
Figure 1C: Elongated Nucleoplasm.
Figure 1D: Shaped, Fetus-Like Covid Nuclei.
Figure 1E: Ring Nuclei.
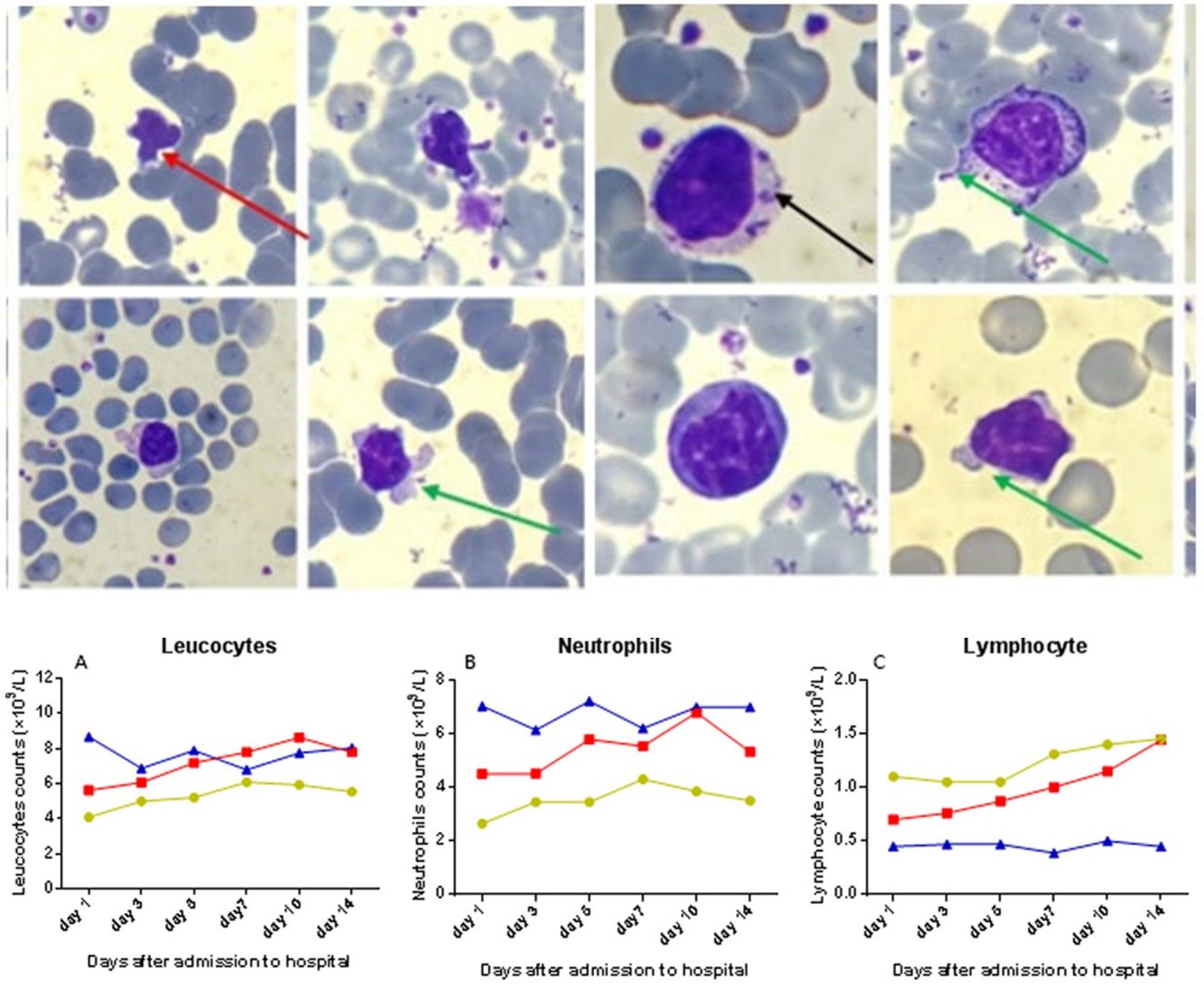
Figure 2: Changes in lymphocytes in Peripheral smear shows large granular lymphocytes. Round to indented nucleus, chromatin is condensed, with prominent nucleoli in few cells and abundant pale blue cytoplasm with azurophilic granules are seen. (Black arrow). Pod formation in cytoplasm (green arrows) and lymphocytes show apoptotic changes (red arrow) highlighted. Giemsa ×200–400 [2].
Figure 3a): Shows leukocytes number variation in patients listed in severe ICU and severe Non ICU group; Figure 3b): Shows neutrophilia in severe ICU group than severe NON-ICU group; Figure 3c): Lymphocytopenia seen in severe ICU group than in severe NON ICU group [3].
![Figure 2: Changes in lymphocytes in Peripheral smear shows large granular lymphocytes. Round to indented nucleus, chromatin is condensed, with prominent nucleoli in few cells and abundant pale blue cytoplasm with azurophilic granules are seen. (Black arrow). Pod formation in cytoplasm (green arrows) and lymphocytes show apoptotic changes (red arrow) highlighted. Giemsa ×200–400 [2].](/fulltextimages/6173/fig_2.jpeg)
Figure 4a) Shows monocytopenia in severe ICU group; Figure 4b) shows eosinophilia in severe ICU group than in severe non-ICU group; Figure 4c) shows haemoglobin decreased in severe ICU group [3].
Figure 5a): Shows Monocyte to Lymphocyte Ratio had a high diagnostic value in differentiating COVID‐19 patients from healthy subjects, but not from ICU and NON ICU patients; Figure 5b): Neutrophil to Lymphocyte Ratio showed significant positive correlations [3].
Neutrophil to Lymphocyte Ratio showed positive correlations which was significant. Monocyte‐to‐lymphocyte ratio could separate efficiently COVID‐19 subjects from healthy subjects, but to separate out ICU and NON ICU group subjects was not possible. So, NLR can be a reliable marker for evaluating the severity of COVID‐19 disease.
References
-
Cheng MP, Papenburg J, Desjardins M, Kanjilal S, Quach C, et al. (2020) Diagnostic testing for severe acute respiratory Syndrome–Related Coronavirus-2: a narrative review. Ann Intern Med 172(11): 726-734.
-
Singh A, Sood N, Narang V, Goyal A (2020) Morphology of COVID-19–affected cells in peripheral blood film. BMJ Case Rep 13(5): 236117.
-
Sun S, Cai X, Wang H, He G, Lin Y, et al. (2020) Abnormalities in peripheral blood system in patients with COVID-19, wenzhou, China. Clinica Chimica Acta 507: 174-180.
-
Yang M, Hon KL, Li K, Fok TF, Li CK (2003) The effect of SARS coronavirus on blood system: its clinical findings and the pathophysiologic hypothesis. 11: 217-221.
-
Bal A, Agarwal R, Vaideeswar P, Arava S, Jain A (2020) COVID-19: An up-to-date review-from morphology to pathogenesis. Indian J Pathol Microbiol 63(3): 358-366.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies