Prevalence of Transfusion Transmissible Infections and Associated Risk Factors among Blood Donors in Bamenda Cameroon
Introduction: Blood transfusion is considered a life-saving procedure but the presence of transfusion transmitted infections (TTIs) is a major public health concern. TTIs such as hepatitis B virus (HBV), hepatitis C virus (HCV), human immunodeficiency virus (HIV), and Treponema pallidum (syphilis) are among the greatest threats to blood safety. In Cameroon, most of the patients remain undiagnosed as they are asymptomatic. This study aimed at determining the prevalence of TTIs and its associated risk factors in blood donors from the Northwest region of Cameroon. Methodology: A retrospective study of blood donors’ records from a rural and urban towns between 2015 to 2017 was reviewed. The data were analyzed using SPSS vs 23.0 and a p-value <0.05 was considered statistically significant. Results: A total of 4020 (91.5%) blood donors were included in the study. The mean age was 27.8years and the proportion of male was 78.3% (3143). The prevalence of TTIs was 7.3% (292) and showed a significant (P=0.001) decreasing trend from 10.2% to 5.7 %. The prevalence of HBV, HCV, HIV and syphilis were 0.7% (27), 1.8% (73) and 1.9% (77) respectively. Except for HCV, all TTIs showed a decreasing trend. From the results, the positive rate of anyone of the TTIs was significantly (p< 0.05) higher among male 8.1% (255), replacement donors 9.1% (240) and those who had attained only basic education 8.5% (91). Co-infection was detected among 0.5% (19) blood donors and the highest prevalence was between HIV and Syphilis 0.15% (6). Independent predictors of anyone of the TTIs were; living in rural towns, males, age group >20 years replacement donors, civil servants, and those who had attained either basic or secondary education. Conclusion: Our data provides important findings that contribute to a better understanding of TTIs epidemiology in Bamenda. Further investigations are needed to assess the prevalence and determinants of these infections in other communities to support the development of effective prevention and control strategies. There is a need for stringent selection of blood donors. High sensitive and specific screening tests such as Nucleic acid testing enzyme immunoassays should be used to diagnose the high-risk donors.
Introduction
Blood transfusion is practiced to save the lives of humans with chronic and life-threatening disorders associated with accidents, sickle cell anemia, or anemia [1, 2, 3, 4]. There is an exponential rise in blood donors and about 118.4 million blood donations are collected worldwide [5, 6]. Although blood safety has greatly improved over the past 15 years, it remains a major public health issue in sub-Saharan Africa (SSA) countries, due to financial constraints that have led to lack of appropriate infrastructures, basic equipment, supplies, trained personnel, shortage of blood donors and retention programs [7].
Although timely transfusion is lifesaving, adequate supplies of safe and affordable blood products remain a serious challenge due to the high prevalence of transfusion transmissible infections (TTIs) which is known to cause fatal, chronic, and life-threatening disorders [1, 8]. These TTIs include HIV, HBV, HCV, and hepatitis E virus, Cytomegalovirus, Treponema pallidum, (syphilis), malaria, Trypanosoma cruzi, and T. brucei, etc [8, 9, 10]. The impact of these infections on individuals and the economy resulted in the creation of a global safety blood initiative by the World Health Organization (WHO) in 1983. Thus, WHO recommends that all blood donations should be mandatorily screened for HIV, HBV, HCV, and syphilis [4, 7, 10, 11, 12]. This act of screening has significantly decreased the prevalence of TTIs [4]. Despite the existence of approved national hemovigilance protocols in most countries blood transfusion continues to carry a certain margin of risk due to the window period (a period where-in an infective pathogen though present cannot be detected) [9, 13].
The transfusion of contaminated blood varies within countries and regions and ranges from 5.1- 43.2% [4, 6, 11, 14, 15]. HIV remains a major threat to transfusion medicine, especially in Africa where about 10-15 % of HIV transmission had been correlated with blood transfusions. Of these, about 25% and 40% occur in pediatric and among children over 1 year of age respectively [2, 3, 6, 7, 10, 14, 15]. Although HBV and HCV control measures have shown to be effective, these infections remains a major health problem in many countries [10, 16]. The transfusion risk of HBV and HCV remains high in developing countries. The prevalence of HBV reported among donors ranges from 1.7 to 23% while HCV ranges from 0.19 -12.5% [3, 6, 7, 10, 15, 16, 17, 18, 19, 20].
Syphilis causes infertility issues, stillbirth, serious neonatal infections as well as increases the chances of acquiring HIV, HBV, and HCV through sexual contact. Previous reports showed that Syphilis is less readily transmitted by blood and the prevalence ranges from 1.2 to 12.8% [6, 7, 15, 16].
In Cameroon, about 400,000 pints of blood is given each year to meet the medical needs of her 25 million people [21, 22]. In Cameroon, the current blood safety guidelines demand blood banks to routinely perform serological testing for HIV, HBV, HCV, and syphilis [6]. Being a country with one of the highest prevalence of TTIs, there is limited published data from most towns in Cameroon. Previous records indicate that the prevalence of TTIs range from 9.5% to 29.05% with the an overall prevalence range of 2.6-3.5% for HIV, 4.8- 10.0% for HBV, 1.9-5.7% for HCV, and 1.07-3.8% for syphilis [6, 16, 19, 23, 24]. However, there is no published report on the trends of TTIs among blood donors in Bamenda. The purpose of this study, therefore, was to determine the prevalence and trend of HBV, HCV, HIV, and syphilis among blood donors in two health districts in Bamenda. Results from this study will provide a better understanding of the epidemiology of these infections, guide policymakers to create a long-term strategy needed to manage the burden of these infections.
Methodology
A retrospective hospital-based, cross-sectional study was conducted in the blood transfusion units of Ndop Health District a rural town and Bamenda Health District an urban town of the Northwest region of Cameroon from May 2015- May 2017. Ethical approval for the study was obtained from the hospitals institutional review board. Secondary data comprising socio-demographic and biological variables (age, sex, level of education, marital status, occupation, type of blood donation, ABO blood group) and results of HBV, HCV, HIV, and Syphilis tests were obtained from the registration records using an anonymous data collection form. Criteria for donors were; age ≥ 17years, ≥ 50kg, showing no clinical signs of fever or have been treated recently for any pathology. Female donors were non-pregnant, non-breastfeeding, and non-menstruating participants.
Data were entered and analyzed using SPSS version 23.0 (SPSS, Inc, Chicago, IL). The prevalence of TTIs was expressed in percentages. Pearson Chi-squire (χ 2) test or Fisher’s exact test was used to evaluate categorical variables. Logistic regression and estimates of the Odds Ratio (OR) were computed to assess the statistical association between TTI (dependent variable) and the influencing factors. A p-value < 0.05 was considered statistically significant.
Socio-demographic Characteristics of Study Participants
Of the 4194 blood donor’s data collected, a total of 95.9% (4020) had complete information and were considered for the analysis. More than half of the participants came from the urban facility 2971 (73.9%). The age ranged between 17 to 65 years with a mean (±Standard error) age of 27.8(± 0.1) years and the majority of the donors belonged to the 21-25years age group 31.4% (1262). More men 3143 (78.2%) participated in the survey with a male-to-female gender ratio of 3.6. More than half of the participants were unmarried; 2988(74.3%) and replacement blood donors 2641(65.7%). The majority of the screened donors were self-employed; 1732 (43.1%) and had attained secondary education 1808(45.0%). Regarding the ABO and Rhesus (RH) group description, most participants had blood group O+ 2026(50.4%) and were rhesus positive 3968(98.7%) as shown in Table 1.
| Characteristics | Variable | Frequency | Percent (%) |
|---|---|---|---|
| place | Rural | 1049 | 26.1 |
| Urban | 2971 | 73.9 | |
| Age group in years | <21 | 837 | 20.8 |
| 21-25 | 1262 | 31.4 | |
| 26-35 | 1206 | 30 | |
| 36-45 | 504 | 12.5 | |
| >45 | 210 | 5.2 | |
| Gender | Female | 877 | 21.8 |
| Male | 3143 | 78.2 | |
| Marital status | Married/Divorced/cohabiting/widow/widower | 1033 | 25.7 |
| Single | 2987 | 74.3 | |
| Donor type | Replacement | 2641 | 65.7 |
| Voluntary | 1379 | 34.3 | |
| Occupation | Civil servant | 599 | 14.9 |
| Self-employed | 1732 | 43.1 | |
| Student | 1689 | 42 | |
| Education | Primary | 1069 | 26.6 |
| Secondary | 1808 | 45 | |
| Tertiary | 1143 | 28.4 | |
| Blood type | A- | 3 | 0.1 |
| A + | 1187 | 29.5 | |
| AB+ | 181 | 4.5 | |
| B- | 4 | 0.1 | |
| B+ | 619 | 15.4 | |
| O- | 41 | 1 | |
| O+ | 1985 | 49.4 |
Table 1: Socio-demographic and biological characteristics of blood donors (N=4020).
NB: + is RhD positive, -is RhD Negative. Table 1: Socio-demographic and biological characteristics of blood donors (N=4020).
The overall prevalence of TTIs was 292(7.3%). The yearly prevalence decreased significantly (χ2 =16.7, p=0.001) and was found to be 10.2% (97), 7.4% (90) and 5.7% (105) in 2015, 2016 and 2017 respectively. The prevalence of HBV, HCV, HIV and syphilis were 3.4% (136), 0.7% (27), 1.8% (73) and 1.9% (77) respectively. As the years increase, the prevalence of HIV, syphilis, and HBV decrease while the prevalence of HCV increases (Figure 1) with significant differences (P<0.05) seen in the prevalence of syphilis and HBV. The prevalence of at least one of TTIs in blood donors was highest among donors from rural towns 8.3%(87), age groups >45 years 8.6%(18), male gender 8.1%(255), married donors 8.6%(89), replacement donors 9.1%(240), civil servants 8.7%(52), primary level of education 8.5%(91) and blood group AB+ 9.9% (18). However, a significant association (P < 0.05) was seen only among gender, donation type and level of education. The 2.2% (23) prevalence of HIV was higher in donors from Rural towns, while HBV 3.6% (107) and Syphilis 2.1% (22) were higher in those from Urban towns. HCV 7(0.7%) was the same in the two towns. HIV; 2.5% (30) showed a higher prevalence in the 21–25years age group while Syphilis; 2.8% (14), HCV; 0.8 % (1) and HBV; 4.0 % (20) were higher in the 36-45years.
With the exception of HIV (p=0.04), the differences were not significant (P > 0.05). Our data revealed that male donors had a higher prevalence of all the TTIs with a significant difference (P<0.05) seen with Syphilis 2.3% (73) and HBV 3.9% (122). Similarly, replacement donors had a significantly (P<0.05) higher prevalence of TTI compared to voluntary donors. A non-significant association (p>0.05) was observed between the different occupation categories with a high prevalence of HBV 3.6% (60) and syphilis 2.1% (36) seen among students while higher prevalence of HIV; 2.8% (17) and HCV; 1.2% (7) were seen among civil servants. Except for HCV 0.8% (15) that was high in those who had attained secondary education, TTI were insignificantly (p > 0.05) highest in those who had attained primary education. The highest prevalence of HIV 3.3% (6) and Syphilis 2.8% (5) was seen in donors with the AB RhD positive (+) blood group, while O RhD negative (-) 2.4% (1) and B+4.5% (28) were highest for HCV and HBV respectively (Table 2).
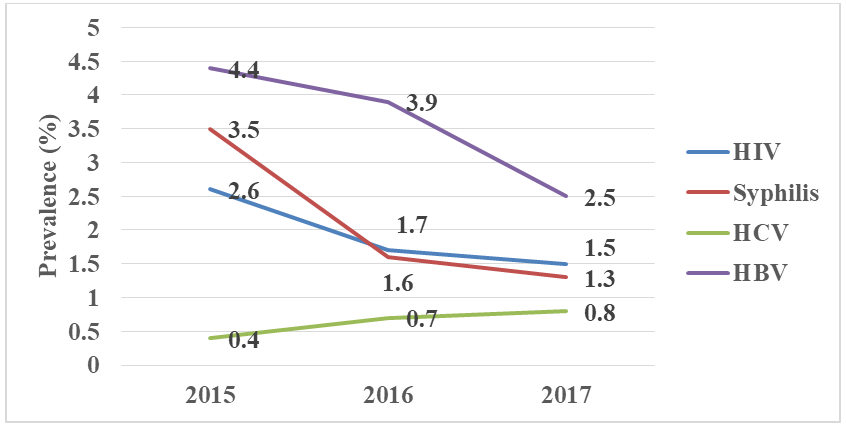
HIV (χ2 =6.8, p=0.089), syphilis (χ2 =16.3, p=0.001), HCV (χ2 =1.2, p=0.55), HBV( χ2 =8.7, p=0.01) Figure 1: The trend of HIV, syphilis, HCV, and HBV across 2015-2017.
| Characteristics | TTIs (%) | HIV (%) | Syphilis (%) | HCV (%) | HBV (%) | |
|---|---|---|---|---|---|---|
| Place (n) | ||||||
| Rural (1049) | 87(8.3) | 23(2.2) | 55(1.9) | 20(0.7) | 29(2.8) | |
| Urban (2971) | 205(6.9) | 50(1.7) | 22(2.1) | 7(0.7) | 107(3.6) | |
| χ2; P-value | 2.24;0.14 | 1.13;0.29 | 0.25; 0.62 | 0.00;0.98 | 1.66;0.20 | |
| Age group (years) | ||||||
| <21(837) | 48(5.7) | 14(1.7) | 8(1.0) | 8(1.0) | 20(2.4) | |
| 21-25(1262) | 89(7.1) | 25(2.0) | 27(2.1) | 9(0.7) | 42(3.3) | |
| 26-35(1206) | 101(8.4) | 30(2.5) | 24(2.0) | 5(0.4) | 46 (3.8) | |
| 36-45(504) | 36 (7.1) | 2(0.4) | 14 (2.8) | 1(0.8) | 20(4.0) | |
| >45(210) | 18(8.6) | 2(1.0) | 4 (1.9) | 4(0.3) | 8 (3.8) | |
| χ2; P-value | 5.77;0.22 | 9.91;0.04 | 6.3; 0.17 | 9.1; 0.06 | 3.88;0.42 | |
| Gender | ||||||
| Female(877) | 37(4.2) | 14(1.6) | 4(0.5) | 5(0.6) | 14(1.6) | |
| Male(3143) | 255(8.1) | 59(1.9) | 73(2.3) | 22(0.7) | 122(3.9) | |
| χ2; P-value | 15.44;0.001 | 0.30;0.58 | 12.7(0.001) | 0.17;0.68 | 10.96;0.001 | |
| Marital status | ||||||
| Married/Divorced/ cohabiting/widow/ widower(1033) | 89(8.6) | 26(2.5) | 32(3.1) | 7(0.7) | 30(2.9) | |
| Single(2987) | 203(6.8) | 47(1.6) | 45(1.5) | 20(0.7) | 106(3.5) | |
| χ2; P-value | 3.77;0.052 | 3.8; 0.05 | 10.35;0.01 | 0.01; 0.98 | 0.98;0.32 | |
| Donor type | ||||||
| Replacement(2641) | 240(9.1) | 63(2.4) | 63(2.4) | 23 (0.9) | 108(4.1) | |
| Voluntary(1379) | 52(3.8) | 10(0.7) | 14(1.0) | 4(0.3) | 28(2.0) | |
| χ2 ; P-value | 38.02;0.001 | 14.0; 0.001 | 9.05;0.003 | 4.58; 0.032 | 11.7; 0.01 | |
| Occupation | ||||||
| Civil servants(599) | 52(8.7) | 17(2.8) | 12(2.0) | 7(1.2) | 18(3.0) | |
| Self-employed(1732) | 117(6.8) | 30(1.7) | 29(1.7) | 6(0.3) | 58(3.3) | |
| Students(1689) | 123(7.3) | 26(1.5) | 36(2.1) | 14(0.8) | 60(3.6) | |
| χ2; P-value | 2.45;0.29 | 4.3; 0.12 | 0.98; 0.61 | 5.6;0.06 | 0.42;0.81 | |
| Education | ||||||
| Primary(1069) | 91(8.5) | 24(2.2) | 26(2.4) | 4(0.4) | 45(4.2) | |
| Secondary(1808) | 107(5.9) | 28(1.5) | 27(1.5) | 15(0.8) | 49(2.7) | |
| Tertiary(1143) | 94(8.2) | 21(1.8) | 24(2.1) | 8(0.7) | 48(3.6) | |
| χ2; P-value | 8.89;0.012 | 1.8; 0.4 | 3.44;0.18 | 2.11; 0.35 | 5.05;0.08 | |
| Blood type | ||||||
| A-(3) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | |
| A+(1187) | 87(7.3) | 21(1.8) | 22(1.9) | 5(0.4) | 46(3.9) | |
| AB+(181) | 18(9.9) | 6(3.3) | 5(2.8) | 1(0.6) | 6(3.3) | |
| B-(4) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | |
| B +(619) | 46(7.4) | 10(1.6) | 11(1.8) | 2(0.3) | 28(4.5) | |
| O-(41) | 3(7.3) | 0(0) | 1(1.4) | 1(2.4) | 0(0) | |
| O+(1985) | 138(7.0) | 36(1.8) | 39(2.4) | 18(0.9) | 56(2.8) | |
| χ2 ; P value | 2.80;0.83 | 3.4; 0.76 | 2.61; 0.86 | 5.9;0.43 | 6.1;0.41 |
Table 2: The positivity rate of HIV, syphilis, HCV, and HBV by demographical and biological characteristics.
NB: + is RhD positive, - is RhD Negative. Table 2: The positivity rate of HIV, syphilis, HCV, and HBV by demographical and biological characteristics.
A total of 19(0.5%) participants had serological evidence of dual infections which were as follows; HIV/syphilis 6 (0.15%), HBV/Syphilis 5 (0.12%), HCV/syphilis 3(0.07%), HCV/HBV 2(0.05%), HIV/HBV 2(0.05%) and HCV/HIV 1(0.02%). Co-infection TTI was common in donors from urban town; 0.5% (15), age group 21-25 years; 1.2% (15), males 0.6% (19), replacement donor 0.6% (16), Students 0.7% (12), those who had attained tertiary education 0.7% (8) and in blood group AB+1.1% (2). With the exception of age group and gender these differences were not significant (p > 0.05) (Table 3).
Place
Age group (years)
<21 837 837(100) 0(0.0)
21-25 1262 1247(98.8) 15(1.2)
26-35 1206 1202(99.7) 4(0.3)
36-45 504 504(100) 0(0.0) >45 210 210(100) 0(0.0)
Gender
Marital status
Married/Divorced /widow/widower 1033 1028(99.5) 5(0.5) 0.95 Single 2987 2973(99.5) 14(0.5) Donor type Replacement 2641 2615(99.4) 16(0.6) 0.09 Voluntary 1379 1376(99,8) 3(0.2) Occupation Civil servants 599 597(99.7) 2(0.3)
0.17 Self-employed 1732 1727(99.7) 5(0.3)
Students 1689 1677 (99.3) 12(0.7)
Education
Primary 1069 1065(99.6) 4(0.4)
Tertiary 1143 1135(99.3) 8(0.7)
Blood type
A- 3 3(100) 0(0)
A + 1187 1181(99.5) 6(0.5)
AB+ 181 180(0.6) 2(1.1)
B- 4 0(0) 0(0)
B+ 619 615(0.6) 3(0.5)
O- 41 41(100) 0(0.0)
O+ 1985 1977(99.6) 8(0.4)
Characteristics Frequency co-infections Chi-square test
No (%) Yes (%) P-value
rural 1049 1045(99.6) 4(0.4) 0.61 Urban 2971 2956(99.5) 15(0.5)
0.001 Female 877 877(100) 0(0.0) 0.021 Male 3143 3124(99.4) 19(0.6)
0.42 Secondary 1808 1801(99.6) 7(0.4)
0.99
- NB: + is RhD positive, - is RhD Negative.
Table 3: The positivity rate of co-infections by demographical and biological characteristics, n (%).
To assess the risk factors of any one of the TTIs, multivariate analysis showed that, the prevalence of any TTI was significantly lower among donors from urban towns (p=0.04) and among female blood donors (p=0.02). The risk was significantly higher among replacement donors (p=0.01) and those who had attained both primary and secondary education (p<0.05). The likelihood of not having any TTI infection was 1.9(1.38-3.84) odds in female donors compared to the male donors and in the age group <21 years
2.04(1.11-3.75). Being a civil servant was 2 times higher 1.5(1.03-2.22) to be infected with at least one of the TTI infections (Table 4).
| Characteristics | Frequency | Positive for any TTIs | |||
|---|---|---|---|---|---|
| N (%) | COR (95%CI) | AOR(95%CI) | P-value | ||
| Place | |||||
| Rural | 1049 | 77(7.3) | 1.4(1.0-1.7) | 0.7(0.57-0.98) | 0.04 |
| Urban | 2971 | 215(7.2) | *1 | *1 | |
| Age group (years) | |||||
| <21 | 837 | 48(5.7) | 0.49(0.27-0.90) | 2.04(1.11-3.75) | 0.02 |
| 21-25 | 1262 | 89(7.1) | 0.59(0.34-1.06) | 1.69(0.95-3.01) | 0.07 |
| 26-35 | 1206 | 101(8.4) | 0.72(0.41-1.27) | 1.40(0.80-2.47) | 0.24 |
| 36-45 | 504 | 36 (7.1) | 0.62(0.33-1.17) | 1.62(0.96-3.06) | 0.14 |
| >45 | 210 | 18(8.6) | *1 | *1 | |
| Gender | |||||
| Female | 877 | 37(4.2) | 0.5(0.34-0.71) | 1.9(1.38-3.84) | 0.02 |
| Male | 3143 | 255(8.1) | *1 | *1 | |
| Marital status | |||||
| Married/Divorced/widow/widower | 1033 | 90(8.7) | 0.8(0.6-1.14) | 1.3(0.89-1.69) | 0.21 |
| Single | 2987 | 202(6.8) | *1 | *1 | |
| Donor type | |||||
| Replacement | 2641 | 240(9.1) | 1.6(1.19-2.27) | 0.6(0.46-0.87) | 0.005 |
| Voluntary | 1379 | 52(3.8) | *1 | *1 | |
| Occupation | |||||
| Civil servants | 599 | 54(9.0) | 0.65(0.44-.95) | 1.5(1.03-2.22) | 0.03 |
| Self-employed | 1732 | 126(7.3) | 0.75(0.49-1.13) | 1.3(0.86-1.95) | 0.21 |
| Students | 1689 | 112(6.6) | *1 | *1 | |
| Education | |||||
| Primary | 1069 | 96(9.0) | .65(0.48-0.89) | 1.59(1.15-2.21) | 0.005 |
| Secondary | 1808 | 117(6.5) | 1.84(1.14-2.95) | 0.54(0.34-0.87) | 0.011 |
| Tertiary | 1143 | 79(6.9) | *1 | *1 | |
| Blood type | |||||
| A- | 3 | 0(0) | ** | ** | 1 |
| A + | 1183 | 87(7.4) | 1.07(0.8-1.4) | 0.6(0.9-1.4) | 0.09 |
| AB+ | 181 | 18(9.8) | 1.5(0.87-2.51) | 0.9(0.6-2.2) | 0.14 |
| B- | 8 | 0(0) | ** | ** | 1 |
| B+ | 619 | 46(7.4) | 1.1(0.8-1.6) | 1.0(0.71-1.44) | 0.96 |
| O- | 41 | 0(0) | 1.0(0.31-3.5) | 0.64(0.25-1.68) | 0.34 |
| O+ | 19850 10 | 138(7.8) | *1 | *1 |
Table 4: Univariate and Multivariate Logistic regression model for demographicaland biological predictors of TTI.
NB: + is RhD positive, - is RhD Negative * Reference category, **this parameter is set to zero because the cell count was < 5 and is considered redundant. Table 4: Univariate and Multivariate Logistic regression model for demographicaland biological predictors of TTI.
Discussion
The overall prevalence of TTIs was 7.3% (292) with a significant decreasing trend of 10.2%, 7.4%, and 5.7% respectively in 2015, 2016, and 2017. Reports from similar studies in different towns in Cameroon and other countries showed a higher prevalence range of 8.2-21.2% [6, 25, 26] and 8.2-29.5% respectively [3, 7, 10, 27]. However, our prevalence was higher compared to the 1.1-7.1% range reported in another study in Douala-Cameroon [28] and other countries [4, 8, 9, 15, 21]. The decreasing trend seen in our data has also been reported in other countries [8, 29]. The decreased trend can be accredited to the different intervention measures taken to prevent the spread of TTIs. In the era of HIV, intense prevention and control programs such as frequent and free HIV screening and the distribution of condoms have a positive impact on the other TTIs since they are all sexually transmitted. Secondly, more people nowadays are aware of the eligibility criteria to donate blood as such they assess their own risk of being infected with TTIs before visiting the Blood Bank Facilities. The differences in the prevalence rate and trend in the different countries can be attributed to the differences in social and cultural characteristics, type of educational programs, preventive measures, public awareness programs, selection criteria of the donors, and the sensitivity and specificity of the test kits being used [9, 30, 31]. Alternatively, the study do not necessarily represent the true TTIs prevalence; since these facilities used rapids test kids which have shown to have some degree of poor sensitivity and specificity in detecting viral TTIs during the long window period [32]. Thus advanced methods like Nucleic acid testing (NAT), enzyme immunoassays (EIA) are needed to diagnose TTIs during the silent window period. Viral infections (HIV, and HBV) associated with blood transfusion are the most feared infection due to the lack of an effective treatment [6]. The prevalence HBV, HCV, HIV and syphilis were 3.4% (136), 0.7% (27), 1.8% (73) and 1.9% (77) respectively. The study demonstrated an upward trend in HCV unlike with the other TTIs over the years similar to findings by Siraj N, et al. [9].
The prevalence of HIV (1.8%) in this study was far lower than the 3.1% reported in the national HIV prevalence (https://knoema.com/atlas/Cameroon/HIV-prevalence) and the 2.2-8.2% range reported among blood donors in other towns (Edéa, Douala or Yaoundé) in Cameroon [11, 25, 26, 32, 33] as well as the 2.6-3.9% range reported in other countries [3, 14, 30]. It was nevertheless higher compared to the 0.04-1.6% range as reported in other countries [7, 8, 21, 27, 29, 34, 35]. The possible reason for low prevalence in this study is due to self-status awareness and frequent free screening activity. As such most donors are aware of their status.
The prevalence of HBV was 3.4% (136) with a decreasing trend seen across the years. The high HBV prevalence compared to the other viral infection has been reported in other studies which state that HBV infection is the most common TTIs [9, 15]. Other studies in other towns in Cameroon have shown higher HBV prevalence of the range 6.1- 16.0% among blood donors. In contrast, the prevalence was far lower compared to the > 8% prevalence reported in [3, 7, 8, 26, 30]. The 0.7% prevalence of HCV seen in this study was far lower than the 6.5% reported in the general population of Cameroon Bigna Kowo and the 0.8- 6.0% range reported among blood donors in Cameroon and other countries [6, 25, 26, 30, 32, 36]. Serum samples from blood donors were tested by quantitative enzyme-linked immunosorbent assays (ELISA]. However, it was higher than the 0.25% and 0.6% reported by Chandekar, et al_._ [34] and Birhaneselassie [21] respectively. Although HBV and HCV virus are transmitted through the same routes (body fluids, blood, saliva, semen, sweat, breast milk, tears, and urine) [10, 34], a decreasing trend seen in HBV contrary to HCV has also been reported elsewhere [8, 17]. This can be attributed to the effectiveness of the hepatitis B vaccination program in Cameroon. As such free HBV vaccination should be given to voluntary blood donors who tested negative as this will minimize HBV transmission in the general population as well.
Even though an effective treatment for syphilis has been available since the 1940s, more than 90% of people in developing countries still acquire new cases of the disease [36, 37]. Our data revealed that the prevalence of syphilis was 1.9% (77) and showed a decreasing trend which was indifferent with results from other African studies [9, 32]. Higher values of the range 5.2-8.1% have been reported previously in Cameroon [6, 19, 36, 38]. However, this result was higher compared to the 0.20-1.1% range reported by [4, 7, 8, 21, 25, 30, 34] but lower than the 2.1- 5.2% range [3, 29] compared to other countries. Although Syphilis is overlooked in Cameroon and there is no awareness campaign, the decreasing prevalence recorded in this study could be due to an increased awareness associated with viral TTIs prevention interventions. This is effective because like viral TTIs, syphilis is also sexually transmitted. Additionally, free antenatal screening and treatment have also contributed to the low prevalence of syphilis. It is worth mentioning that syphilis treatment is cheap, easy, and very effective, and positive diagnosed persons are treated alongside their sexual partners. Lastly, the serological test being used in Cameroon is specific and reliable as such it can identify early syphilis infection.
Studies on the sexually transmitted infection (STI) have shown regional variation among urban and rural cities in Cameroon [28, 39]. Donors in rural settings were more prevalent for TTIs as seen in other studies [7, 40]. There is a high probability that individuals from urban settings usually have access to free screening prior to testing at the Blood Bank as such this account for self-status awareness. Free screening for HIV, HBV, and HCV is a regular exercise in most urban towns in Cameroon [24]. Secondly, health talk programs are common in urban cities than in rural cities leading to poor prevention practices. In addition, it has been reported that people with multiple sex partners are more common in rural areas where the use of condoms is low [39, 40]. This regional variation can be attributed to the level of education, the population of pregnant women, cultural differences, or the population of blood donors [24, 28].
High 155(8.1%) TTIs prevalence seen in blood donors in the age range 26-35years is consistent with studies done elsewhere [7, 8, 21] and contrary to studies by Adu-poku F, et al. [3] which state that donors >50 years have lower infection rates while other studies have reported higher prevalence in the age group < 25 years [9, 31]. The observed pattern may be associated with behavioral characteristics associated with exposure risk exceptional for these age groups. Considering that all the TTIs are sexually transmitted there is a need to assess the potential risk factors of TTIs among different age groups to account for this variation.
The male to female sex ratio of 3.6 seen in this study has been supported by Birhaneselassie, Kowo MP, Sharew B, Mbanya DN, Sehgal S [21, 25, 31, 33, 35]. The high participation of the male gender may be explained by the fact that in the African context there is a general belief that men are healthier than women and thus are more suitable for blood donation. Alternatively fewer women contribute to blood donations because of physiological factors such as menstruation, lactation, pregnancy, and childbirth [4, 6, 10, 32]. A TTI prevalence of 4.2% for females and 8.1% for males was recorded in this study. A similar trend has been reported in Cameroon and other countries [3, 4, 6, 9, 24, 31]. High prevalence in males can be as a result of behavioral and socio-cultural activities exposing them to several risk factors of TTIs [2, 15]. According to Banong-Le, et al. [37] males usually have more sexual partners, for fame and to gain social status as influential men among their male peers. The low TTIs prevalence in females can also be elucidated by the fact that during antenatal care (ANC) most pregnant women are screened for the presence of these TTIs. As such, female blood donors who are of childbearing age usually know their status before blood donation. Furthermore, the low prevalence can be attributed to the fact that the number of female donors is fewer compared to male donors. Married donors were found to have a higher prevalence of TTIs 8.7% (90). Such findings have been reported in literature [10, 39].
Considering that TTIs are sexually transmitted infections these individuals practice unprotected sexual activity most of the time and some of them might have multiple sexual partners.
TTIs prevalence was high in the replacement donors 9.1% (240) compared to voluntary donors 3.8% (52). On the contrary higher occurrence in volunteer donors have been reported in Yaoundé the capital of Cameroon [6] and in another country [34]. Our findings are consistent with previous observations in Cameroon and other countries [7, 8, 9, 21, 29, 32, 35]. Replacement donors are persons who donate blood intending to help relatives or acquaintances (colleagues and friends) who need a blood transfusion. In addition, they can be paid donors posing as relatives [6, 8, 10]. The low TTIs prevalence in voluntary blood donors is because these individuals have committed themselves in donating blood as such do not have high-risk behaviors such as multiple sex partners, intravenous drug abuse, or unprotected sexual intercourse [7, 10]. Conversely, replacement donors habitually will not provide accurate and truthful disclosure of their risky behavior as they might be paid donors posing as relatives. As recommended by WHO, policymakers should encourage voluntary donation with certain benefits (offering them reduced charges in medical bills, financial benefit) to diminish the transfusion of TTIs. Unfortunately, Cameroon like other countries is facing a dramatic drop in donations over the past year [21]. To alleviate this situation, it is good to encourage voluntary donors through the stringent selection of blood donors during outreach campaigns in community, schools, churches, and other institutions.
The occurrence of TTIs was highest among civil servants 8.2% (52) and least among self-employed 6.8% (117) similar to other studies [15, 21] and contrary to studies by Abdella, et al_. [7], Bartonjo, et al. [10] which state that unemployed blood donors have higher TTIs prevalence. The low prevalence in student can be explained by the fact that sex education is now part of the school curriculum. Thus enabling them to understand different prevention methods High prevalence in civil servants may be a result of socio- economic factors that have shown to contribute to high-risk behavior such as having multiple sexual partners by person, who are financially viable as they are involved in sexual activity for economic reasons. Primary education recorded a significantly (P =0.001) high prevalence of 8.5%(91) of TTIs comparable to studies by [9, 10]. The level of education has been shown to correlate positively with preventive measures as such those with a primary level of education may not be aware of the preventive measures put in place [10]. Secondly, most educated people with risky behavior will not go in for blood donation. TTIs were more common in the AB+ blood type 9.9%(18), contrary to O+ as reported by Birhaneselassie M [21] and A+ by Ankouane, et al._ [41]. Based on this discrepancy more research is needed to clarify the precise role of the ABO blood group in TTIs. We reported a co-infection rate of 0.5% which was higher compared to the 0.2% reported by Eboumbou M, et al. [6] but lower compared to the 4.2% - 4.8% range in Cameroon [32, 38] and the 0.008 - 0.8% range reported in another country [21, 34, 41]. The study showed that co-infection was common among persons who tested positive for syphilis with HIV/ syphilis and HBV/Syphilis as the most common combination as reported by [6, 15, 21, 34]. It was, however, contrary to the report by Birhaneselassie M [21], Grillo M, et al. [32] and Noubiap J, et al. [38] who reported a higher infection rate between HBV/HCV and HBV/HIV. It has been reported that infection with syphilis may increase the risk of HBV, HCV, and HIV transmission through the genital sore/ulcer associated with syphilis [31]. This explains the high prevalence of syphilis co-infection seen in this study.
Considering that the first step in ensuring blood safety is the selection of low-risk blood donors, rural towns, males, replacement donors, and primary education exhibited a statistically significant association with any one of the TTIs. On the contrary, Eboumbou M, et al. [6] did not identify any risk factor. Several studies from different countries identify different risk factors such as replacement donors, being married, or single [3, 10, 21, 39]. Thus the identification of these risk factors is imperative not only to monitor the safety of blood supply but the success of the screening procedures. The disparity in these results does not fully convince researchers as being universally applicable based on diverse regions, cultures, and specific human adaptations. It is for this reason that similar studies should be carried out in other towns of Cameroon to identify possible risk factors associated with TTIs to provide baseline information on the selection of blood donors before the screening.
Limitations
Due to the retrospective nature of the study design, other risk factors such as number of blood donations per person, number of sexual partners, skin scaring, drug users, were not collected as such we could not embellish all the possible predictors that may influence the prevalence of TTIs.
Conclusion
The prevalence of TTI infection among blood donors is high in this study and needs constant monitoring to evaluate prevention and control strategies. The indicated prevalence is uncertain because of the lack of more sensitive screening methods. The results from this study can be used as a reliable tool to identify donors at risk of transmitting TTIs thus reducing the possibility of window period transmission.
Recommendations
There is a need to improve the awareness of disease prevention in the general population and strengthened prevention strategies in rural areas. The government should promote the use of voluntary donors and also encourage the number of female donors. More comprehensive methods using the identified risk factors are needed to improve the recruitment of blood donors. The use of more sensitive donor screening tests such as NAT and ELISA should be encouraged in all blood donation sites at a price affordable to the person in need of blood. There is need to build up a quality assurance program in all blood donating sites. Early treatment of all identified sero-positive blood donors is, therefore, encouraged to significantly reduce TTIs related morbidity and mortality.
Acknowledgement
We acknowledge the blood bank staff of the Ndop district hospital and Regional hospital Bamenda services for good collaboration during data collection.
References
-
Okoroiwu HU, Okafor IM, Asemota EA, Okpokam DC (2018) Seroprevalence of transfusion-transmissible infections (HBV, HCV, syphilis and HIV) among prospective blood donors in a tertiary health care facility in Calabar, Nigeria; An eleven years evaluation. BMC Public Health 18(1): 645.
-
Tigabu A, Engda T, Mekonnen F (2019) Seroprevalence of transfusion transmissible viral infections (HIV, HBV and HCV) among voluntary blood donors at University of Gondar Comprehensive Specialized Hospital, Gondar; Northwest Ethiopia. BMC Infect Dis 19(1): 393.
-
Adu-poku F, Agboli E, Tarkang EE, Region HV, Region HV (2020) Seroprevalence of transfusion-transmissible infections among blood donors in the Hohoe Municipal Hospital, Ghana: 2015-2016: a retrospective hospital- based cross-sectional study. Pan Afr Med J Clin Med 2: 12.
-
Aabdien M, Selim N, Himatt S, Hmissi S, Merenkov Z, et al. (2020) Prevalence and trends of transfusion transmissible infections among blood donors in the State of Qatar, 2013-2017. BMC Infect Dis 20(1): 617.
-
WHO (2020) Blood safety and availability. World Health Organization.
-
Eboumbou Moukoko CE, Ngo Sack F, Essangui Same EG, Mbangue M, Lehman LG (2014) HIV, HBV, HCV and T. pallidum infections among blood donors and transfusion-related complications among recipients at the Laquintinie hospital in Douala, Cameroon. BMC Hematol 14(1): 5.
-
Abdella S, Berheto TM, Tolera G, Belete W, Deressa T, et al. (2020) Sero-prevalence of transfusion transmittable infections: HIV, Hepatitis B, C and Treponema pallidum and associated factors among blood donors in Ethiopia: A retrospective study. PLoS One 15(10): e0241086.
-
Azerefegn E, Worku M, Hailemariam M (2018) Transfusion-Transmissible Infections among Blood Donors at Hawassa Regional Blood Bank Center, South Ethiopia. IJRSMB 4(3): 10-16.
-
Siraj N, Achila OO, Issac J, Menghisteab E, Hailemariam M, et al. (2018) Seroprevalence of transfusion-transmissible infections among blood donors at National Blood Transfusion Service, Eritrea: A seven-year retrospective study. BMC Infect Dis 18(1): 264.
-
Bartonjo G, Oundo J, Ng’ang’a Z (2019) Prevalence and associated risk factors of transfusion transmissible infections among blood donors at regional blood transfusion center nakuru and tenwek mission hospital, Kenya. Pan Afr Med J 34: 31.
-
Ndo C, Ngalle JTE, Ewodo S, Olemba C, Adiogo D (2019) Hepatitis B and C, HIV, Syphilis Seroprevalences and Asymptomatic Carriage of Hemoparasites Among Blood Donors at the Douala General Hospital in Cameroon, Central Africa. Biomed J Sci Tech Res 18(5): 13968- 13974.
-
WHO (2008) Report of the Regional Director. World Health Organization (54): 1-9.
-
Moor ACE, Dubbelman TM, VanSteveninck J, Brand A (1999) Transfusion-transmitted diseases: Risks, prevention and perspectives. Eur J Haematol 62(1): 1-18.
-
Negash M, Ayalew M, Geremew D, Workineh M (2019) Seroprevalence and associated risk factors for HIV, Hepatitis B and C among blood Donors in South Gondar District blood Bank, Northwest Ethiopia. BMC Infect Dis 19(1): 430.
-
Teklemariam Z, Mitiku H, Weldegebreal F (2018) Seroprevalence and trends of transfusion transmitted infections at Harar blood bank in Harari regional state, Eastern Ethiopia: Eight years retrospective study BMC Hematol 18: 24.
-
Kabemba BH, Kasendue EP, Shiku MA, Mukena TS, Kasolva TC, et al. (2017) Seroprevalence of Hepatitis B Virus Infection (HBsAg) in Rural Blood Donors, Moba, Tanganyika Province, Democratic Republic of Congo (2014 to 2016). OALib 4(3): 1-5.
-
Choudhuri G, Gupta V, Negi TS, Ojha R (2019) Potential Implications of Detecting HBsAg in Asymptomatic People in an Endemic Community Through Medical Camps. J Clin Exp Hepatol 9(1): 43-49.
-
Qowaider SRM, Ali MS, Moftah SAM, Kahald FA (2017) Prevalence of HBV and HCV Infections among Blood Donors in Northeast Libya. Int Blood Res Rev 7(1): 1-5.
-
Fopa D, Candotti D, Tagny CT, Doux C, Mbanya D, et al. (2019) Occult hepatitis B infection among blood donors from Yaoundé, Cameroon. Blood Transfus 24: 1-6.
-
Mbendi NC, Longo Mbenza B, Mbendi NS, Muyembe TJJ, Nanituma HS, et al. (2001) Prevalence of HIV and HBS Antigen in Blood Donors, Residual Risk of Contamination in Recipients of Blood of East Kinshasa, Democratic Republic of Congo. Med Trop 61(2): 139-142.
-
Birhaneselassie M (2016) Prevalence of transfusion- transmissible infections in donors to an Ethiopian blood bank between 2009 and 2013 and donation factors that would improve the safety of the blood supply in underdeveloped countries. Lab Med 47(2): 134-139.
-
Kindzeka ME (2021) Cameroon Begs Civilians to Donate Blood on World Blood Donor Day.
-
Kengne M, Tsata DCW, Ndomgue T, Nwobegahay JM (2018) Prevalence and risk factors of HTLV-1/2 and other blood borne infectious diseases among blood donors in yaounde central hospital, Cameroon. Pan Afr Med J 30: 125.
-
Noah Noah D, Njouom R, Bonny A, Pirsou P, Meli J, et al. (2011) HBs antigene prevalence in blood donors and the risk of transfusion of hepatitis B at the central hospital of yaounde, cameroon. Open J Gastroenterol 1(2): 23-27.
-
Kowo MP, Andoulo FA, Ngek LT, Sizimboue DT, Ndam AN, et al. (2019) Prevalence of Hepatitis C Virus and Associated Risk Factors among Inmates at New Bell Prison, Douala, Cameroon. Open J Epidemiol 9(2): 119- 128.
-
Bigna JJ, Amougou MA, Asangbeh SL, Kenne AM, Noumegni SRN, et al. (2017) Seroprevalence of hepatitis B virus infection in Cameroon: a systematic review and meta-analysis. BMJ Open 7(6): e015298.
-
Onyango CG, Ogonda L, Guyah B, Okoth P, Shiluli C, et al. (2018) Seroprevalence and determinants of transfusion transmissible infections among voluntary blood donors in Homabay, Kisumu and Siaya counties in western Kenya. BMC Res Notes 11: 171.
-
Dionne Odom J, Mbah R, Rembert NJ, Tancho S, Halle Ekane GE, et al. (2016) Hepatitis B, HIV, and Syphilis Seroprevalence in Pregnant Women and Blood Donors in Cameroon. Infect Dis Obstet Gynecol pp: 4359401.
-
Arshad A, Borhany M, Anwar N, Naseer I, Ansari R, et al. (2016) Prevalence of transfusion transmissible infections in blood donors of Pakistan. BMC Hematol 16: 27.
-
Buseri FI, Muhibi MA, Jeremiah ZA (2009) Sero- epidemiology of transfusion-transmissible infectious diseases among blood donors in Osogbo, south-west Nigeria. Blood Transfus 7(4): 293-299.
-
Sharew B, Mulu A, Teka B, Tesfaye T (2017) HIV-sero- prevalence trend among blood donors in north east Ethiopia. Afr Health Sci 17(3): 712-718.
-
Grillo M, Tran BR, Tamoufe U, Djoko CF, Saylors K, et al. (2017) HIV and Syphilis Prevalence and Associated Risks in the Cameroonian Armed Forces. Curr HIV Res 15(2): 137-145.
-
Mbanya DN, Takam D, Ndumbey PM (2003) Serological findings amongst first-time blood donors in Yaounde, Cameroon: Is safe donation a reality or a myth? Transfus Méd 13(5): 267-273.
-
Chandekar SA, Amonkar GP, Desai HM, Valvi N, Puranik GV (2017) Seroprevalence of transfusion transmitted infections in healthy blood donors: A 5-year tertiary care hospital experience. J Lab Physicians 9(4): 283-287.
-
Sehgal S, Shaiji PS, Brar RK (2017) Seroprevalence and trends of transfusion transmissible infections in blood donors in Andaman and Nicobar Islands- An institutional retrospective study. J Clin Diagn Res 11(4): 21-24.
-
Mogtomo K, Louandji FML, Fotso KH, Ngane NA (2009) Détection des agents infectieux dans les banques de sang de Douala (1995-2004). Santé 19(1): 3-8.
-
Banong Le M, Ofosu SK, Anto F (2019) Factors associated with syphilis infection: A cross-sectional survey among outpatients in Asikuma Odoben Brakwa District, Ghana. BMC Infect Dis 19: 360.
-
Noubiap JJN, Joko WYA, Nansseu JRN, Tene UG, Siaka C (2013) Sero-epidemiology of human immunodeficiency virus, hepatitis B and C viruses, and syphilis infections among first-time blood donors in Edéa, Cameroon. Int J Infect Dis 17(10): e832-e837.
-
Kengne Nde C, de Dieu Anoubissi J, Loni Ekali G, Nguefeu Nkenfou C, Moussa Y, et al. (2020) Highlighting a population-based re-emergence of Syphilis infection and assessing associated risk factors among pregnant women in Cameroon: Evidence from the 2009, 2012 and 2017 national sentinel surveillance surveys of HIV and syphilis. PLoS One 15(11): e0241999.
-
Xu T, Yi ZM, Luo JM, Yu HL, Fan YH, et al. (2019) Prevalence and trends of transfusion-transmittable infections among blood donors in Southwest China. J Public Heal (Oxf) 41(1): 55-61.
-
Ankouane F, Noah DN, Atangana MM, Simo RK, Guekam PR, et al. (2016) Seroprevalence of hepatitis B and C viruses, HIV-1/2 and syphilis among blood donors in the Yaoundé Central Hospital in the centre region of Cameroon. Transfus Clin Biol 23(2): 72-77.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies